Crossed Brainstem Syndrome Revealing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Approach to a Case of Congenital Heart Disease
BAI JERBAI WADIA HOSPITAL FOR CHILDREN PEDIATRIC CLINICS FOR POST GRADUATES PREFACE This book is a compilation of the discussions carried out at the course for post-graduates on ” Clinical Practical Pediatrics” at the Bai Jerbai Wadia Hospital for Children, Mumbai. It has been prepared by the teaching faculty of the course and will be a ready-reckoner for the exam-going participants. This manual covers the most commonly asked cases in Pediatric Practical examinations in our country and we hope that it will help the students in their practical examinations. An appropriately taken history, properly elicited clinical signs, logical diagnosis with the differential diagnosis and sound management principles definitely give the examiner the feeling that the candidate is fit to be a consultant of tomorrow. Wishing you all the very best for your forthcoming examinations. Dr.N.C.Joshi Dr.S.S.Prabhu Program Directors. FOREWARD I am very happy to say that the hospital has taken an initiative to organize this CME for the postgraduate students. The hospital is completing 75 years of its existence and has 2 done marvelous work in providing excellent sevices to the children belonging to the poor society of Mumbai and the country. The hospital gets cases referred from all over the country and I am proud to say that the referrals has stood the confidence imposed on the hospital and its faculty. We do get even the rarest of the rare cases which get diagnosed and treated. I am sure all of you will be immensely benefited by this programme. Wish you all the best in your examination and career. -
INTRODUCTION Time, Are Discussed in Full, for Without Accurate
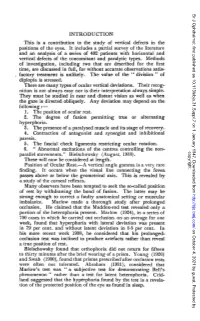
Br J Ophthalmol: first published as 10.1136/bjo.31.Suppl.7 on 1 January 1947. Downloaded from INTRODUCTION This is a contribution to the study of vertical defects in the positions of the eyes. It includes a partial survey of the literature and an analysis of a series of 402 patients with horizontal and vertical defects of the concomitant and paralytic types. Methods of investigation, including two that are described for the first time, are discussed in full, for without accurate observations satis- factory treatment is unlikely. The value of the " division " of diplopia is stressed. There are many types of ocular vertical deviations. Their recog- nition is not always easy nor is their interpretation always simple. They must be studied in near and distant vision as well as when the gaze is directed obliquely. Any deviation may depend on the following: 1. The position of ocular rest. 2. The degree of fusion permitting true or alternating hyperphoria. 3. The presence of a paralysed muscle and its stage of recovery. 4. Contraction of antagonist and synergist and inhibitional paresis. 5. The fascial check ligaments restricting ocular rotation. 6. " Abnormal excitations of the centres controlling the non- copyright. parallel movements." Bielschowsky (August, 1938). These will now be considered at length. Position of Ocular Rest.-A vertical angle gamma is a very rare finding. It occurs when the visual line connecting the fovea passes above or below the geometrical axis. This is revealed by a study of the corneal reflexes. Many observers have been tempted to seek the so-called position of rest by withdrawing the bond of fusion. -
Basilar Artery and Its Branches Called Pontine Arteries
3 Farah Mohammad Ahmad Al-Tarefe Mohammad Al salem تذكر أ َّن : أولئك الذين بداخلهم شيء يفوق كل الظروف ، هم فقط من استطاعوا أ ّن يحققوا انجازاً رائعاً .... كن ذا همة Recommendation: Study this sheet after you finish the whole anatomy material . Dr.Alsalem started talking about the blood supply for brain and spinal cord which are mentioned in sheet#5 so that we didn't write them . 26:00-56:27/ Rec.Lab#3 Let start : Medulla oblengata : we will study the blood supply in two levels . A- Close medulla (central canal) : It is divided into four regions ; medial , anteromedial , posteriolateral and posterior region. Medially : anterior spinal artery. Anteromedial: vertebral artery posterolateral : posterior inferior cerebellar artery ( PICA). Posterior : posterior spinal artery which is a branch from PICA. B-Open medulla ( 4th ventricle ) : It is divided into four regions ; medial , anteromedial , posteriolateral region. Medially : anterior spinal artery. Anteromedial: vertebral artery posterolateral : posterior inferior cerebellar artery ( PICA). 1 | P a g e Lesions: 1- Medial medullary syndrome (Dejerine syndrome): It is caused by a lesion in anterior spinal artery which supplies the area close to the mid line. Symptoms: (keep your eyes on right pic). Contralateral hemiparesis= weakness: the pyramid will be affected . Contralateral loss of proprioception , fine touch and vibration (medial lemniscus). Deviation of the tongue to the ipsilateral side when it is protruded (hypoglossal root or nucleus injury). This syndrome is characterized by Alternating hemiplegia MRI from Open Medulla (notice the 4th ventricle) Note :The Alternating hemiplegia means ; 1- The upper and lower limbs are paralyzed in the contralateral side of lesion = upper motor neuron lesion . -

Alternating Hemiplegia of Childhood Syndrome
orphananesthesia Anaesthesia recommendations for Alternating Hemiplegia of Childhood syndrome Disease name: Alternating hemiplegia of childhood syndrome (AHC) ICD 10: G98 Synonyms: AHC syndrome (An ATP1A3-related neurologic disorder). AHC was named for its most striking and diagnostic motor symptom; however, the range of manifestations show it to be a CNS disorder affecting function broadly in various brain circuits, heart and the disease evolves with age. Disease summary: AHC is a very rare neurological disorder first described in 1971 which has received increasing interest recently [1]. It is characterized by hemiplegia of either side of the body, paroxysmal tonic or dystonic spells, oculomotor abnormalities and developmental delay.2-4 Onset occurs before 18 months of age. This condition is diagnosed based on the occurrence of the above combination of symptoms, is usually due to de novo pathogenic variant in ATP1A3 and has also been reported in a few families [2-3]. Onset and progression of neurological symptoms have been well characterized. While the course and severity of deficits can vary considerably, there appears to be progression over time, at least in some patients. The differential diagnosis of AHC includes familial hemiplegic migraine (FHM) syndromes (e.g. FHM1-CACNA1A; FHM2-ATP1A2), episodic ataxia type 6, glutamate transporter disorders (SLC1A3), glucose transporter defects, GLUT1 deficiency (SLC2A1), infantile onset epileptic encephalopathies, severe myoclonic epilepsy of infancy (Dravet syn- drome), SCN1A mutations, mitochondrial disorders, and disorders of dopamine biosynthesis/ neurotransmitter disorders. The prevalence has been estimated at 1:1,000,000 with most cases being due to de novo mutations [4-6]. Triggers in AHC and other ATP1A3 related diseases that can induce paroxysmal episodes in AHC are frequent. -

Multiple Intracerebral Hemorrhages in an Old Patient with Rheumatoid Arthritis
Multiple Intracerebral Hemorrhages in an Old Patient with Rheumatoid Arthritis INIMIOARA MIHAELA COJOCARU1, 2, V. ŞTEFĂNESCU2, DANIELA TRAŞCĂ2, ADELINA ŞERBAN-PEREŢEANU2, B. CHICOŞ3, M. COJOCARU3,4 1“Carol Davila” University of Medicine and Pharmacy, Bucharest 2Department of Neurology, “Colentina” Clinical Hospital 3“Dr. Ion Stoia” Clinical Center for Rheumatic Diseases 4“Titu Maiorescu” University, Faculty of Medicine, Bucharest, Romania A 78-year-old Caucasian man was admitted in the Department of Neurology for visual disturbances, started two days before. The next day the patient experienced headache, fever and gait disturbances. He had hypertension, diabetes mellitus, an ischemic stroke 13 years ago, longstanding seronegative rheumatoid arthritis (17 years), polynodular goiter, right ischio-pubian fracture and right femoral vein thrombosis a year ago due to a car accident, since he is treated with oral anticoagulants associated to antiaggregant, hypotensors, statin and oral antidiabetics. The neurologic examination had evidenced nuchal rigidity, left homonymous hemianopsia, left central facial palsy, ataxia of the inferior limbs with wide-based gait, achilean reflexes abolished bilaterally, bilaterally abolished plantar reflexes, ideomotor apraxia, dysarthria, hypoprosexia, and preserved consciousness patient. A non-contrast cerebral CT scan had shown right temporal and parieto-occipital intraparenchymatous hemorrhages, a right frontal sequelar lesion, multiple old lacunar infarcts, cortical atrophy. Laboratory findings included an inflammatory syndrome, absence of rheumatoid arthritis positive serology, normal coagulogram, an elevated proteinuria. The cerebral IRM performed on the seventh day of hospitalisation was suggestive for subacute right parietal hemorrhage, old cerebral infarction in the right anterior cerebral artery area, old lacunar infarcts and cerebral atrophy. The anticoagulant and antiaggregant treatment was stopped after a generalized tonic-clonic seizure occurred. -

Cerebellar Ataxia
CEREBELLAR ATAXIA Dr. Waqar Saeed Ziauddin Medical University, Karachi, Pakistan What is Ataxia? ■ Derived from a Greek word, ‘A’ : not, ‘Taxis’ : orderly Ataxia is defined as an inability to maintain normal posture and smoothness of movement. Types of Ataxia ■ Cerebellar Ataxia ■ Sensory Ataxia ■ Vestibular Ataxia Cerebellar Ataxia Cerebrocerebellum Spinocerebellum Vestibulocerebellum Vermis Planning and Equilibrium balance Posture, limb and initiating and posture eye movements movements Limb position, touch and pressure sensation Limb ataxia, Eye movement dysdiadochokinesia, disorders, Truncal and gait Dysmetria dysarthria nystagmus, VOR, ataxia hypotonia postural and gait. Gait ataxia Types of Cerebellar Ataxia • Vascular Acute Ataxia • Medications and toxins • Infectious etiologies • Atypical Infectious agents • Autoimmune disorders • Primary or metastatic tumors Subacute Ataxia • Paraneoplastic cerebellar degeneration • Alcohol abuse and Vitamin deficiencies • Systemic disorders • Autosomal Dominant Chronic • Autosomal recessive Progressive • X linked ataxias • Mitochondrial • Sporadic neurodegenerative diseases Vascular Ataxia ▪ Benedikt Syndrome It is a rare form of posterior circulation stroke of the brain. A lesion within the tegmentum of the midbrain can produce Benedikt Syndrome. Disease is characterized by ipsilateral third nerve palsy with contralateral hemitremor. Superior cerebellar peduncle and/or red nucleus damage in Benedikt Syndrome can further lead in to contralateral cerebellar hemiataxia. ▪ Wallenberg Syndrome In -

Facial Nerve Electrodiagnostics for Patients with Facial Palsy: a Clinical Practice Guideline
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Helsingin yliopiston digitaalinen arkisto European Archives of Oto-Rhino-Laryngology (2020) 277:1855–1874 https://doi.org/10.1007/s00405-020-05949-1 REVIEW ARTICLE Facial nerve electrodiagnostics for patients with facial palsy: a clinical practice guideline Orlando Guntinas‑Lichius1,2,3 · Gerd Fabian Volk1,2 · Kerry D. Olsen4 · Antti A. Mäkitie5 · Carl E. Silver6 · Mark E. Zafereo7 · Alessandra Rinaldo8 · Gregory W. Randolph9 · Ricard Simo10 · Ashok R. Shaha11 · Vincent Vander Poorten3,12 · Alfo Ferlito13 Received: 14 March 2020 / Accepted: 27 March 2020 / Published online: 8 April 2020 © The Author(s) 2020 Abstract Purpose Facial nerve electrodiagnostics is a well-established and important tool for decision making in patients with facial nerve diseases. Nevertheless, many otorhinolaryngologist—head and neck surgeons do not routinely use facial nerve electro- diagnostics. This may be due to a current lack of agreement on methodology, interpretation, validity, and clinical application. Electrophysiological analyses of the facial nerve and the mimic muscles can assist in diagnosis, assess the lesion severity, and aid in decision making. With acute facial palsy, it is a valuable tool for predicting recovery. Methods This paper presents a guideline prepared by members of the International Head and Neck Scientifc Group and of the Multidisciplinary Salivary Gland Society for use in cases of peripheral facial nerve disorders based on a systematic literature search. Results Required equipment, practical implementation, and interpretation of the results of facial nerve electrodiagnostics are presented. Conclusion The aim of this guideline is to inform all involved parties (i.e. -

Cranial Nerves 1, 5, 7-12
Cranial Nerve I Olfactory Nerve Nerve fiber modality: Special sensory afferent Cranial Nerves 1, 5, 7-12 Function: Olfaction Remarkable features: – Peripheral processes act as sensory receptors (the other special sensory nerves have separate Warren L Felton III, MD receptors) Professor and Associate Chair of Clinical – Primary afferent neurons undergo continuous Activities, Department of Neurology replacement throughout life Associate Professor of Ophthalmology – Primary afferent neurons synapse with secondary neurons in the olfactory bulb without synapsing Chair, Division of Neuro-Ophthalmology first in the thalamus (as do all other sensory VCU School of Medicine neurons) – Pathways to cortical areas are entirely ipsilateral 1 2 Crania Nerve I Cranial Nerve I Clinical Testing Pathology Anosmia, hyposmia: loss of or impaired Frequently overlooked in neurologic olfaction examination – 1% of population, 50% of population >60 years Aromatic stimulus placed under each – Note: patients with bilateral anosmia often report nostril with the other nostril occluded, eg impaired taste (ageusia, hypogeusia), though coffee, cloves, or soap taste is normal when tested Note that noxious stimuli such as Dysosmia: disordered olfaction ammonia are not used due to concomitant – Parosmia: distorted olfaction stimulation of CN V – Olfactory hallucination: presence of perceived odor in the absence of odor Quantitative clinical tests are available: • Aura preceding complex partial seizures of eg, University of Pennsylvania Smell temporal lobe origin -

Alternating Hemiplegia of Childhood: New Diagnostic Options
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Via Medica Journals n e u r o l o g i a i n e u r o c h i r u r g i a p o l s k a 4 8 ( 2 0 1 4 ) 1 3 0 – 1 3 5 Available online at www.sciencedirect.com ScienceDirect journal homepage: http://www.elsevier.com/locate/pjnns Review article Alternating hemiplegia of childhood: New diagnostic options Aleksandra Gergont *, Marek Kaciński Department of Neurology of Children and Youth, Jagiellonian University, Collegium Medicum, Krakow, Poland a r t i c l e i n f o a b s t r a c t Article history: A syndrome of alternating hemiplegia of childhood (AHC) is a rare disorder first presented in Received 14 August 2012 1971. AHC is characterized by transient episodes of hemiplegia affecting either one or both sides Accepted 13 May 2013 of the body. Age of onset is before 18 months and the common earliest manifestations are Available online 15 February 2014 dystonic or tonic attacks and nystagmus. Hemiplegic episodes last minutes to days and the frequency and duration tend to decrease with time. Motor and intellectual development is fi Keywords: affected, de cits may also develop later. Epileptic seizures occur in some patients. Neuroimaging of the brain usually reveals no abnormalities. The variability of individual clinical presentations Alternating hemiplegia fi Children and evolution of symptoms have made diagnosis dif cult. Therefore the problems of misdiag- ATP1A3 nosis could account for the low prevalence of this syndrome. -

Topical Diagnosis in Neurology
V Preface In 2005 we publishedacomplete revision of Duus’ Although the book will be useful to advanced textbook of topical diagnosis in neurology,the first students, also physicians or neurobiologists inter- newedition since the death of its original author, estedinenriching their knowledge of neu- Professor PeterDuus, in 1994.Feedbackfromread- roanatomywith basic information in neurology,oR ers wasextremelypositive and the book wastrans- for revision of the basics of neuroanatomywill lated intonumerous languages, proving that the benefit even morefromit. conceptofthis book wasasuccessful one: combin- This book does notpretend to be atextbook of ing an integrated presentation of basic neu- clinical neurology.That would go beyond the scope roanatomywith the subject of neurological syn- of the book and also contradict the basic concept dromes, including modern imaging techniques. In described above.Firstand foremostwewant to de- this regard we thank our neuroradiology col- monstratehow,onthe basis of theoretical ana- leagues, and especiallyDr. Kueker,for providing us tomical knowledge and agood neurological exami- with images of very high quality. nation, it is possible to localize alesion in the In this fifthedition of “Duus,” we have preserved nervous system and come to adecision on further the remarkablyeffective didactic conceptofthe diagnostic steps. The cause of alesion is initially book,whichparticularly meets the needs of medi- irrelevant for the primarytopical diagnosis, and cal students. Modern medical curricula requirein- elucidation of the etiology takes place in asecond tegrative knowledge,and medical studentsshould stage. Our book contains acursoryoverviewofthe be taught howtoapplytheoretical knowledge in a major neurologicaldisorders, and it is notintended clinical settingand, on the other hand, to recognize to replace the systematic and comprehensive clinical symptoms by delving intotheir basic coverage offeredbystandardneurological text- knowledge of neuroanatomyand neurophysiology. -

THE SYNDROMES of the ARTERIES of the BRAIN and SPINAL CORD Part 1 by LESLIE G
65 Postgrad Med J: first published as 10.1136/pgmj.29.328.65 on 1 February 1953. Downloaded from THE SYNDROMES OF THE ARTERIES OF THE BRAIN AND SPINAL CORD Part 1 By LESLIE G. KILOH, M.D., M.R.C.P., D.P.M. First Assistant in the Joint Department of Psychological Medicine, Royal Victoria Infirmary and University of Durham Introduction general circulatory efficiency at the time of the Little interest is shown at present in the syn- catastrophe is of the greatest importance. An dromes of the arteries of the brain and spinal cord, occlusion, producing little effect in the presence of and this perhaps is related to the tendency to a normal blood pressure, may cause widespread minimize the importance of cerebral localization. pathological changes if hypotension co-exists. Yet these syndromes are far from being fully A marked discrepancy has been noted between elucidated and understood. It must be admitted the effects of ligation and of spontaneous throm- that in many cases precise localization is often of bosis of an artery. The former seldom produces little more than academic interest and ill effects whilst the latter frequently determines provides Protected by copyright. nothing but a measure of personal satisfaction to infarction. This is probably due to the tendency the physician. But it is worth recalling that the of a spontaneous thrombus to extend along the detailed study of the distribution of the bronchi affected vessel, sealing its branches and blocking and of the pathological anatomy of congenital its collateral circulation, and to the fact that the abnormalities of the heart, was similarly neglected arterial disease is so often generalized. -

High-Yield Neuroanatomy
LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page i Aptara Inc. High-Yield TM Neuroanatomy FOURTH EDITION LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page ii Aptara Inc. LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page iii Aptara Inc. High-Yield TM Neuroanatomy FOURTH EDITION James D. Fix, PhD Professor Emeritus of Anatomy Marshall University School of Medicine Huntington, West Virginia With Contributions by Jennifer K. Brueckner, PhD Associate Professor Assistant Dean for Student Affairs Department of Anatomy and Neurobiology University of Kentucky College of Medicine Lexington, Kentucky LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page iv Aptara Inc. Acquisitions Editor: Crystal Taylor Managing Editor: Kelley Squazzo Marketing Manager: Emilie Moyer Designer: Terry Mallon Compositor: Aptara Fourth Edition Copyright © 2009, 2005, 2000, 1995 Lippincott Williams & Wilkins, a Wolters Kluwer business. 351 West Camden Street 530 Walnut Street Baltimore, MD 21201 Philadelphia, PA 19106 Printed in the United States of America. All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appearing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Lippincott Williams & Wilkins at 530 Walnut Street, Philadelphia, PA 19106, via email at [email protected], or via website at http://www.lww.com (products and services).