Cerebellar Ataxia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Spinocerebellar Ataxia Type 29 Due to Mutations in ITPR1: a Case Series and Review of This Emerging Congenital Ataxia Jessica L
Zambonin et al. Orphanet Journal of Rare Diseases (2017) 12:121 DOI 10.1186/s13023-017-0672-7 RESEARCH Open Access Spinocerebellar ataxia type 29 due to mutations in ITPR1: a case series and review of this emerging congenital ataxia Jessica L. Zambonin1*, Allison Bellomo2, Hilla Ben-Pazi3, David B. Everman2, Lee M. Frazer2, Michael T. Geraghty4, Amy D. Harper5, Julie R. Jones2, Benjamin Kamien6, Kristin Kernohan1,4, Mary Kay Koenig7, Matthew Lines4, Elizabeth Emma Palmer8,9, Randal Richardson10, Reeval Segel11, Mark Tarnopolsky12, Jason R. Vanstone4, Melissa Gibbons13, Abigail Collins14, Brent L. Fogel15, Care4Rare Canada Consortium, Tracy Dudding-Byth16 and Kym M. Boycott1,4 Abstract Background: Spinocerebellar ataxia type 29 (SCA29) is an autosomal dominant, non-progressive cerebellar ataxia characterized by infantile-onset hypotonia, gross motor delay and cognitive impairment. Affected individuals exhibit cerebellar dysfunction and often have cerebellar atrophy on neuroimaging. Recently, missense mutations in ITPR1 were determined to be responsible. Results: Clinical information on 21 individuals from 15 unrelated families with ITPR1 mutations was retrospectively collected using standardized questionnaires, including 11 previously unreported singletons and 2 new patients from a previously reported family. We describe the genetic, clinical and neuroimaging features of these patients to further characterize the clinical features of this rare condition and assess for any genotype-phenotype correlation for this disorder. Our cohort consisted of 9 males and 12 females, with ages ranging from 28 months to 49 years. Disease course was non-progressive with infantile-onset hypotonia and delays in motor and speech development. Gait ataxia was present in all individuals and 10 (48%) were not ambulating independently between the ages of 3–12 years of age. -

Diagnostic Clues in Multiple System Atrophy
DO I:10.4274/Tnd.82905 Case Report / Olgu Sunumu Diagnostic Clues in Multiple System Atrophy: A Case Report and Literature Review Multisistem Atrofi Tanısında İpuçları: Bir Olgu Sunumu ve Literatürün Gözden Geçirilmesi Mehmet Yücel, Oğuzhan Öz, Hakan Akgün, Semai Bek, Tayfun Kaşıkçı, İlter Uysal, Yaşar Kütükçü, Zeki Odabaşı Gülhane Military Medical Academy, Ankara, Turkey Sum mary Multiple system atrophy (MSA) is an adult-onset, sporadic, progressive neurodegenerative disease. Based on the consensus criteria, patients with MSA are clinically classified into cerebellar (MSA-C) and parkinsonian (MSA-P) subtypes. In addition to major diagnostic criteria including poor response to levodopa, and presence of pyramidal or cerebellar signs (ataxia) or autonomic failure, certain clinical features or ‘‘red flags’’ may raise the clinical suspicion for MSA. In our case report we present a 67-year-old female patient admitted to our hospital due to inability to walk, with poor response to levodopa therapy, whose neurological examination revealed severe Parkinsonism, ataxia and who fulfilled all criteria for MSA, as rarely seen in clinical practice.(Turkish Journal of Neurology 2013; 19:28-30) Key Words: Multiple system atrophy, autonomic failure, diagnostic criteria Özet Multisistem atrofi (MSA) erişkin dönemde başlayan, ilerleyici, nedeni bilinmeyen sporadik nörodejeneratif bir hastalıktır. MSA kabul görmüş tanı kriterlerine göre klinik olarak serebellar (MSA-C) ve parkinsoniyen (MSA-P) alt tiplerine ayrılmaktadır. Düşük levadopa yanıtı, piramidal, serebellar bulguların (ataksi) ya da otonomik bozukluk olması gibi majör tanı kriterlerininin yanında “red flags” olarak isimlendirilen belirgin klinik bulgular ya da uyarı işaretlerinin olması MSA tanısı için klinik şüpheyi oluşturmalıdır. Olgu sunumunda 67 yaşında yürüyememe şikayeti ile polikliniğimize müracaat eden ve levadopa tedavisine düşük yanıt gösteren ciddi parkinsonizm bulguları ile ataksi bulunan kadın hasta MSA tanı kriterlerini tam olarak karşıladığı ve klinik pratikte nadir görüldüğü için sunduk. -

Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies
17_Lupski 3/30/06 1:47 PM Page 243 NeuroMolecular Medicine Copyright © 2006 Humana Press Inc. All rights of any nature whatsoever reserved. ISSN0895-8696/06/08:243–254/$30.00 doi: 10.1385/NMM:8:1:243 REVIEW ARTICLE Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies Kinga Szigeti,1 Eva Nelis,2,3 and James R. Lupski*,1,4 1Departments of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX; 2Molecular Genetics, Flanders Interuniversity Institute for Biotechnology, Institute Born-Bunge, University of Antwerp, Antwerpen, Belgium; 3Laboratory of Neurogenetics, Institute Born-Borge, University of Antwerp, Antwerpen, Belgium; and 4Pediatrics, Baylor College of Medicine, and Texas Children Hospital, Houston, TX 77030 Received January 10, 2006; Revised January 13, 2006; Accepted January 13, 2006 Abstract DNAdiagnostics plays an important role in the characterization and management of patients manifesting inherited peripheral neuropathies. We describe the clinical integration of molecular diagnostics with medical history, physical examination, and electrophysiological studies. Mole- cular testing can help establish a secure diagnosis, enable genetic counseling regarding recurrence risk, potentially provide prognostic information, and in the near future may be important for the choice of therapies. doi: 10.1385/NMM:8:1:243 Index Entries:Molecular diagnostics; Charcot-Marie-Tooth disease; CMT; hereditary neuropathy with liability to pressure palsies; HNPP; Dejerine-Sottas neuropathy; DSN; congenital hypomyelinating neuropathy; CHN; CMT1A duplication; HNPP deletion. Introduction genetic testing, one needs to be familiar with the diagnostic tests available, choose the appropriate Molecular genetic diagnosis has become an inte- patients for testing, and utilize the diagnostic tools gral part of the evaluation of patients with hered- in a logical fashion to optimize the use of resources. -

Efficacy of Rhythmic Auditory Stimulation on Ataxia and Functional Dependence Post- Cerebellar Stroke" (2020)
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Yale School of Medicine Physician Associate Program Theses School of Medicine 5-22-2020 Efficacy of Rhythmicudit A ory Stimulation on Ataxia and Functional Dependence Post-Cerebellar Stroke Kaitlin Fitzgerald Yale Physician Associate Program, [email protected] Follow this and additional works at: https://elischolar.library.yale.edu/ysmpa_theses Recommended Citation Fitzgerald, Kaitlin, "Efficacy of Rhythmic Auditory Stimulation on Ataxia and Functional Dependence Post- Cerebellar Stroke" (2020). Yale School of Medicine Physician Associate Program Theses. 13. https://elischolar.library.yale.edu/ysmpa_theses/13 This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Yale School of Medicine Physician Associate Program Theses by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. EFFICACY OF RHYTHMIC AUDITORY STIMULATION ON ATAXIA AND FUNCTIONAL DEPENDENCE POST-CEREBELLAR STROKE A Thesis Presented to The Faculty of the School of Medicine Yale University In Candidacy for the degree of Master of Medical Science May 2020 Kaitlin Fitzgerald, PA-SII Dr. Diana Richardson, MD Class of 2020 Assistant Clinical Professor Yale Physician Associate Program. Yale School of Medicine, Neurology i Table of Contents ABSTRACT -

Cognitive Impairments in Patients with Congenital Nonprogressive Cerebellar Ataxia
1/26/2011 Cognitive impairments in patients with… Articles Cognitive impairments in patients with congenital nonprogressive cerebellar ataxia Maja Steinlin, MD, Marianne Styger, LicPhil and Eugen Boltshauser, MD + Author Affiliations Address correspondence and reprint requests to Dr. Maja Steinlin, Division of Neurology, University Children’s Hospital, Inselspital, 3010 Bern, Switzerland; e-mail: [email protected] Abstract Objective: To report neuropsychologic functions and developmental problems of patients with congenital nonprogressive cerebellar ataxia. Background: Growing interest in cerebellar function has prompted closer attention to cognitive impairments in patients with cerebellar damage. Methods: The authors studied 11 patients with nonprogressive congenital ataxia (NPCA) with Wechsler’s intelligence testing, with additional tests of attention, memory, language, visual perception, and frontal functions. Results: Seven of the 11 patients had an IQ of 60 to 92, with marked nonverbal deficits and subnormal to normal verbal performance (group A). Four patients had an IQ of 30 to 49 without pronounced profile asymmetry (group B). Four of the 7 group A patients had decreased alertness and sustained attention, but all had normal selective attention. Tests of frontal functions and memory yielded higher verbal scores than nonverbal scores. There was no deficit on the Aachener Naming Test (similar to the Boston Naming Test), because there were marked difficulties in the majority with visuoconstructive tasks and visual perception. Group B was significantly abnormal in almost all subtests, having a less prominent but similar profile. Conclusion: Patients with NPCA have significant cognitive deficits with an asymmetric profile and better verbal than nonverbal performance. Effects on nonverbal performance of longstanding deficits in visuospatial input during learning, the influence of impaired procedural learning, and asymmetric plasticity of the cerebral hemispheres may contribute to this uneven neuropsychological profile. -

Ataxia Digest
Ataxia Digest 2015 Vol. 2 News from the Johns Hopkins Ataxia Center 2016 What is Ataxia? Ataxia is typically defined as the presence of Regardless of the type of ataxia a person may have, it abnormal, uncoordinated movements. This term is is important for all individuals with ataxia to seek proper most often, but not always, used to describe a medical attention. For the vast majority of ataxias, a neurological symptom caused by dysfunction of the treatment or cure for the disease is not yet available, so cerebellum. The cerebellum is responsible for many the focus is on identifying symptoms related to or motor functions, including the coordination of caused by the ataxia. By identifying the symptoms of voluntary movements and the maintenance of balance ataxia it becomes possible to treat those symptoms and posture. through medication, physical therapy, exercise, other therapies and sometimes medications. Those with cerebellar ataxia often have an “ataxic” gait, which is walking The Johns Hopkins Ataxia Center has a that appears unsteady, uncoordinated multidisciplinary clinical team that is dedicated to and staggered. Other activities that helping those affected by ataxia. The center has trained require fine motor control like writing, specialist ranging from neurologists, nurses, reading, picking up objects, speaking rehabilitation specialists, genetic counselors, and many clearly and swallowing may be others. This edition of the Ataxia Digest will provide abnormal. Symptoms vary depending you with information on living with ataxia and the on the cause of the ataxia and are multidisciplinary center at Johns Hopkins. specific to each person. Letter from the Director Welcome to the second edition of the Ataxia Digest. -

Topical Diagnosis in Neurology
V Preface In 2005 we publishedacomplete revision of Duus’ Although the book will be useful to advanced textbook of topical diagnosis in neurology,the first students, also physicians or neurobiologists inter- newedition since the death of its original author, estedinenriching their knowledge of neu- Professor PeterDuus, in 1994.Feedbackfromread- roanatomywith basic information in neurology,oR ers wasextremelypositive and the book wastrans- for revision of the basics of neuroanatomywill lated intonumerous languages, proving that the benefit even morefromit. conceptofthis book wasasuccessful one: combin- This book does notpretend to be atextbook of ing an integrated presentation of basic neu- clinical neurology.That would go beyond the scope roanatomywith the subject of neurological syn- of the book and also contradict the basic concept dromes, including modern imaging techniques. In described above.Firstand foremostwewant to de- this regard we thank our neuroradiology col- monstratehow,onthe basis of theoretical ana- leagues, and especiallyDr. Kueker,for providing us tomical knowledge and agood neurological exami- with images of very high quality. nation, it is possible to localize alesion in the In this fifthedition of “Duus,” we have preserved nervous system and come to adecision on further the remarkablyeffective didactic conceptofthe diagnostic steps. The cause of alesion is initially book,whichparticularly meets the needs of medi- irrelevant for the primarytopical diagnosis, and cal students. Modern medical curricula requirein- elucidation of the etiology takes place in asecond tegrative knowledge,and medical studentsshould stage. Our book contains acursoryoverviewofthe be taught howtoapplytheoretical knowledge in a major neurologicaldisorders, and it is notintended clinical settingand, on the other hand, to recognize to replace the systematic and comprehensive clinical symptoms by delving intotheir basic coverage offeredbystandardneurological text- knowledge of neuroanatomyand neurophysiology. -

Children with Ataxia in Conductive Education
Central Journal of Neurological Disorders & Stroke Short Communication *Corresponding author Erzsébet Balogh, International Pető Association, András Pető College, Gizella út 1. 1143 Budapest, Hungary, Tel: Children with Ataxia in Conductive 003613837255; Email: [email protected] Submitted: 16 September 2020 Education Accepted: 29 September 2020 Published: 30 September 2020 1 2 Erzsébet Balogh * and Éva Feketéné Szabó ISSN: 2334-2307 1International Pető Association, András Pető College, Hungary Copyright 2 András Pető College, Semmelweis University, Hungary © 2020 Balogh E, et al. OPEN ACCESS Abstract Impaired coordination caused by cerebral, cerebellar or spinal impairment, with hypoxic or Keywords genetic causes, answer to the Pető’s conductive education quite fair. It might mean the most favorable • Pető method facilitation for developmental processes and by the so called structural cerebellar reserve or by • Conductive education extra-cerebellar parts of the brain. • Ataxia ABBREVIATIONS CP: Cerebral Palsy; CE: Conductive Education induced abnormal coordination test, become increasingly INTRODUCTION successful with repeated new trials – even in a few minutes. Some elements of classical neurological tests for coordination adapted An accumulation of children with ataxia can be observed in to age can be used extremely advantageously in rehabilitation, conductive educational services worldwide. including conductive education (CE), e.g. imitated play – finger MATERIALS AND METHODS movements on imaginary piano keys, rhythmic, bilateral synchronous or alternating movement series. These are applied facilitationalso in Pető’s tool CE in which CE is usescalled holistic, rhythmical pedagogical intention, tools intention for the global upbringing of infants and children [5,6]. The most powerful Based on the files of previously assessed children with ataxia will be create soon special conductive educational groups. -

THE SYNDROMES of the ARTERIES of the BRAIN and SPINAL CORD Part 1 by LESLIE G
65 Postgrad Med J: first published as 10.1136/pgmj.29.328.65 on 1 February 1953. Downloaded from THE SYNDROMES OF THE ARTERIES OF THE BRAIN AND SPINAL CORD Part 1 By LESLIE G. KILOH, M.D., M.R.C.P., D.P.M. First Assistant in the Joint Department of Psychological Medicine, Royal Victoria Infirmary and University of Durham Introduction general circulatory efficiency at the time of the Little interest is shown at present in the syn- catastrophe is of the greatest importance. An dromes of the arteries of the brain and spinal cord, occlusion, producing little effect in the presence of and this perhaps is related to the tendency to a normal blood pressure, may cause widespread minimize the importance of cerebral localization. pathological changes if hypotension co-exists. Yet these syndromes are far from being fully A marked discrepancy has been noted between elucidated and understood. It must be admitted the effects of ligation and of spontaneous throm- that in many cases precise localization is often of bosis of an artery. The former seldom produces little more than academic interest and ill effects whilst the latter frequently determines provides Protected by copyright. nothing but a measure of personal satisfaction to infarction. This is probably due to the tendency the physician. But it is worth recalling that the of a spontaneous thrombus to extend along the detailed study of the distribution of the bronchi affected vessel, sealing its branches and blocking and of the pathological anatomy of congenital its collateral circulation, and to the fact that the abnormalities of the heart, was similarly neglected arterial disease is so often generalized. -
Crossed Brainstem Syndrome Revealing
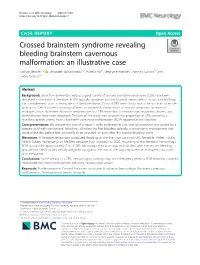
Beucler et al. BMC Neurology (2021) 21:204 https://doi.org/10.1186/s12883-021-02223-7 CASE REPORT Open Access Crossed brainstem syndrome revealing bleeding brainstem cavernous malformation: an illustrative case Nathan Beucler1,2* , Sébastien Boissonneau1,3, Aurélia Ruf4, Stéphane Fuentes1, Romain Carron3,5 and Henry Dufour1,6 Abstract Background: Since the nineteenth century, a great variety of crossed brainstem syndromes (CBS) have been described in the medical literature. A CBS typically combines ipsilateral cranial nerves deficits to contralateral long tracts involvement such as hemiparesis or hemianesthesia. Classical CBS seem in fact not to be so clear-cut entities with up to 20% of patients showing different or unnamed combinations of crossed symptoms. In terms of etiologies, acute brainstem infarction predominates but CBS secondary to hemorrhage, neoplasm, abscess, and demyelination have been described. The aim of this study was to assess the proportion of CBS caused by a bleeding episode arising from a brainstem cavernous malformation (BCM) reported in the literature. Case presentation: We present the case of a typical Foville syndrome in a 65-year-old man that was caused by a pontine BCM with extralesional bleeding. Following the first bleeding episode, a conservative management was decided but the patient had eventually to be operated on soon after the second bleeding event. Discussion: A literature review was conducted focusing on the five most common CBS (Benedikt, Weber, Foville, Millard-Gubler, Wallenberg) on Medline database from inception to 2020. According to the literature, hemorrhagic BCM account for approximately 7 % of CBS. Microsurgical excision may be indicated after the second bleeding episode but needs to be carefully weighted up against the risks of the surgical procedure and openly discussed with the patient. -

High-Yield Neuroanatomy
LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page i Aptara Inc. High-Yield TM Neuroanatomy FOURTH EDITION LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page ii Aptara Inc. LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page iii Aptara Inc. High-Yield TM Neuroanatomy FOURTH EDITION James D. Fix, PhD Professor Emeritus of Anatomy Marshall University School of Medicine Huntington, West Virginia With Contributions by Jennifer K. Brueckner, PhD Associate Professor Assistant Dean for Student Affairs Department of Anatomy and Neurobiology University of Kentucky College of Medicine Lexington, Kentucky LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page iv Aptara Inc. Acquisitions Editor: Crystal Taylor Managing Editor: Kelley Squazzo Marketing Manager: Emilie Moyer Designer: Terry Mallon Compositor: Aptara Fourth Edition Copyright © 2009, 2005, 2000, 1995 Lippincott Williams & Wilkins, a Wolters Kluwer business. 351 West Camden Street 530 Walnut Street Baltimore, MD 21201 Philadelphia, PA 19106 Printed in the United States of America. All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appearing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Lippincott Williams & Wilkins at 530 Walnut Street, Philadelphia, PA 19106, via email at [email protected], or via website at http://www.lww.com (products and services). -
True and False Localization in Neuro- Ophthalmology—A Report of Two Cases
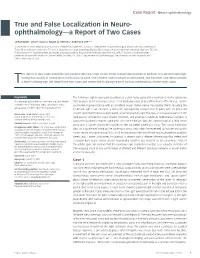
Case Report Neuro-ophthalmology True and False Localization in Neuro- ophthalmology—a Report of Two Cases Jared Raabe,1 Lance J Lyons,2 Bayan Al Othman,3 Andrew G Lee3,4,5,6 1. University of Texas Medical Branch, School of Medicine, Galveston, TX, USA; 2. Department of Ophthalmology & Visual Sciences, University of Texas Medical Branch, Galveston, TX, USA; 3. Department of Ophthalmology, Blanton Eye Institute, Houston Methodist Hospital, Houston, TX, USA; 4. Departments of Ophthalmology, Neurology, and Neurosurgery, Weill Cornell Medicine, New York, NY, USA; 5. Section of Ophthalmology, University of Texas MD Anderson Cancer Center, Houston, TX, USA; 6. Department of Ophthalmology, The University of Iowa Hospitals and Clinics, Iowa City, IA, USA his report of two cases describes two patients who each had ocular motor cranial neuropathies in addition to a second neurologic finding that usually, in combination, hold localizing value. One of these cases localized as anticipated, and the other case demonstrated Ta false localizing sign. We detail these two cases and review the localizing value of various combinations of neurologic signs. Keywords The Parkinson sign is classically described as a sixth nerve palsy and an ipsilateral Horner syndrome Oculomotor palsy, Horner syndrome, ocular motor that localizes to the cavernous sinus. 1,2 The localizing value of any afferent and efferent (e.g., Horner cranial nerve, Parkinson sign, cavernous sinus, syndrome) pupillary finding with an ipsilateral ocular motor cranial neuropathy merits revisiting the anisocoria, relative afferent pupillary defect Parkinson sign.3,4 For example, a unilateral pupil-sparing cranial nerve III palsy with an ipsilateral Disclosure: Jared Raabe, Lance Lyons, smaller pupil (rather than a larger pupil), a normal pupillary light reaction, an anisocoria worse in the Bayan Al Othman, and Andrew Lee have no dark (ocular sympathetic pupil dilation problem), and absence of aberrant regeneration suggests a relevant conflicts of interest to declare.