Antimicrobial Therapy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of New Drugs Approved in India from 1991 to 2000
LIST OF NEW DRUGS APPROVED IN INDIA FROM 1991 TO 2000 S. No Name of Drug Pharmacological action/ Date of Indication Approval 1 Ciprofloxacin 0.3% w/v Eye Indicated in the treatment of February-1991 Drops/Eye Ointment/Ear Drop external ocular infection of the eye. 2 Diclofenac Sodium 1gm Gel March-1991 3 i)Cefaclor Monohydrate Antibiotic- In respiratory April-1991 250mg/500mg Capsule. infections, ENT infection, UT ii)Cefaclor Monohydrate infections, Skin and skin 125mg/5ml & 250mg/5ml structure infections. Suspension. iii)Cefaclor Monohydrate 100mg/ml Drops. iv)Cefaclor 187mg/5ml Suspension (For paediatric use). 4 Sheep Pox Vaccine (For April-1991 Veterinary) 5 Omeprazole 10mg/20mg Short term treatment of April-1991 Enteric Coated Granules duodenal ulcer, gastric ulcer, Capsule reflux oesophagitis, management of Zollinger- Ellison syndrome. 6 i)Nefopam Hydrochloride Non narcotic analgesic- Acute April-1991 30mg Tablet. and chronic pain, including ii)Nefopam Hydrochloride post-operative pain, dental 20mg/ml Injection. pain, musculo-skeletal pain, acute traumatic pain and cancer pain. 7 Buparvaquone 5% w/v Indicated in the treatment of April-1991 Solution for Injection (For bovine theileriosis. Veterinary) 8 i)Kitotifen Fumerate 1mg Anti asthmatic drug- Indicated May-1991 Tablet in prophylactic treatment of ii)Kitotifen Fumerate Syrup bronchial asthma, symptomatic iii)Ketotifen Fumerate Nasal improvement of allergic Drops conditions including rhinitis and conjunctivitis. 9 i)Pefloxacin Mesylate Antibacterial- In the treatment May-1991 Dihydrate 400mg Film Coated of severe infection in adults Tablet caused by sensitive ii)Pefloxacin Mesylate microorganism (gram -ve Dihydrate 400mg/5ml Injection pathogens and staphylococci). iii)Pefloxacin Mesylate Dihydrate 400mg I.V Bottles of 100ml/200ml 10 Ofloxacin 100mg/50ml & Indicated in RTI, UTI, May-1991 200mg/100ml vial Infusion gynaecological infection, skin/soft lesion infection. -

Biofilm Forming Bacteria in Adenoid Tissue in Upper Respiratory Tract Infections
Recent Advances in Otolaryngology and Rhinology Case Report Open Access | Research Biofilm Forming Bacteria in Adenoid Tissue in Upper Respiratory Tract Infections Mariana Pérez1*, Ariana García1, Jacqueline Alvarado1, Ligia Acosta1, Yanet Bastidas1, Noraima Arrieta1 and Adriana Lucich1 1Otolaryngology Service Hospital de niños” JM de los Ríos” Caracas, Venezuela Abstract Introduction: Biofilm formation by bacteria is studied as one of the predisposing factors for chronicity and recurrence of upper respiratory tract infections. Objective: To determine the presence of Biofilm producing bacteria in patients with adenoid hypertrophy or adenoiditis. Methodology: A prospective and descriptive field study. The population consisted of 102 patients with criteria for adenoidectomy for obstructive adenoid hypertrophy or recurrent adenoiditis. Bacterial culture was performed, and specialized adenoid tissue samples were taken and quantified to determine by spectrophotometry the ability of Biofilm production. Five out of 10 samples were processed with electronic microscopy. Results: A The mean age was of 5.16 years, there were no significant sex predominance (male 52.94 %). There was bacterial growth in the 69.60% of the cultures, 80.39% for recurrent Adenoiditis and 19.61% for adenoid Hypertrophy, Staphylococcus Aureus predominating in 32.50% (39 samples). 88.37 % were producing bacteria Biofilm. 42.25% in Adenoiditis showed strong biofilm production, compared with samples from patients with adenoid hypertrophy where only 5.65 % were producers. The correlation was performed with electronic microscopy in 10 samples with 30 % false negatives. Conclusions: The adenoid tissue serves as a reservoir for biofilm producing bacteria, being the cause of recurrent infections in upper respiratory tract. Therapeutic strategies should be established to prevent biofilm formation in the early stages and to try to stop bacterial binding to respiratory mucosa. -
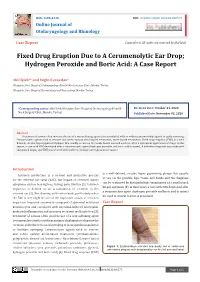
Fixed Drug Eruption Due to a Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: a Case Report
ISSN: 2688-8238 DOI: 10.33552/OJOR.2020.04.000577 Online Journal of Otolaryngology and Rhinology Case Report Copyright © All rights are reserved by Akif İşlek Fixed Drug Eruption Due to A Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: A Case Report Akif İşlek1* and Engin Karaaslan2 1Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey 2Nusaybin State Hospital, Dermatology and Venereology, Mardin, Turkey *Corresponding author: Received Date: October 24, 2020 Published Date: November 03, 2020 Akif İşlek, Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey. Abstract Treatment of earwax often involves the use of a wax softening agent (cerumenolytic) with or without antimicrobial agents to easily removing. Cerumenolytic agents used to remove and soften earwax areoil-based treatments, water-based treatments. Fixed drug eruption (FDE) is a well- defined, circular, hyperpigmented plaque that usually occurs on the trunk, hands mucosal surfaces, after a systemical application of drugs. In this report, a case with FDE developed after a cerumenolytic agent (hydrogen peroxide and boric acid in water). A definitive diagnosis was made with skin punch biopsy and FDE was treated with oral levocetirizine and topical mometasone. Introduction is a well-defined, circular, hyper pigmenting plaque that usually Cerumen production is a normal and protective process occurs on the genitals, lips, trunk, and hands and the diagnosis for the external ear canal (EAC), but impact of cerumen causes can be confirmed by histopathologic examination of a small punch symptoms such as hearing loss, itching, pain, tinnitus [1]. Cerumen biopsy specimen [5]. In this report, a case with FDE developed after impaction is defined as an accumulation of cerumen in the a cerumenolytic agent (hydrogen peroxide and boric acid in water) external ear [2]. -

Communicable Diseases of Children
15 Communicable Diseases of Children Dennis 1. Baumgardner The communicable diseases of childhood are a source of signif from these criteria, the history, physical examination, and ap icant disruption for the family and a particular challenge to the propriate laboratory studies often define one of several other family physician. Although most of these illnesses are self more specific respiratory syndromes as summarized in limited and without significant sequelae, the socioeconomic Table 15.1.3-10 impact due to time lost from school (and work), costs of medi Key points to recall are that significant pharyngitis is not cal visits and remedies, and parental anxiety are enormous. present with most colds, that most colds are 3- to 7-day Distressed parents must be treated with sensitivity, patience, illnesses (except for lingering cough and coryza for up to and respect for their judgment, as they have often agonized for 2 weeks), and that abrupt worsening of symptoms or develop hours prior to calling the physician. They are usually greatly ment of high fever mandates prompt reevaluation. Tonsillo reassured when given a specific diagnosis and an explanation of pharyngitis (hemolytic streptococci, Epstein-Barr virus, the natural history of even the most minor syndrome. adenovirus, Corynebacterium) usually involves a sore throat, It is essential to promptly differentiate serious from benign fever, erythema of the tonsils and pharynx with swelling or disorders (e.g., acute epiglottitis versus spasmodic croup), to edema, and often headache and cervical adenitis. In addition to recognize serious complications of common illnesses (e.g., var the entities listed in Table 15.1, colds must also be differenti icella encephalitis), and to recognize febrile viral syndromes ated from allergic rhinitis, asthma, nasal or respiratory tree (e.g., herpangina), thereby avoiding antibiotic misuse. -

Synergistic Activity of Ampicillin and Cloxacillin
144 THE JOURNAL OF ANTIBIOTICS APR. 1969 SYNERGISTIC ACTIVITY OF AMPICILLIN AND CLOXACILLIN PROTECTIVE EFFECT OF CLOXACILLIN ON ENZYMATIC DEGRADATION OF AMPICILLIN BY PENICILLINASE, AND THERAPEUTIC ACTIVITY OF MIXTURES OF AMPICILLIN AND CLOXACILLIN MlNORUNlSHIDA, YASUHIROMlNE Research Laboratories, Fujisawa Pharmaceutical Co., Ltd., Osaka, Japan and Shogo Kuwahara Department of Microbiology, Toho University School of Medicine, Tokyo, Japan (Received for publication February 15, 1969) A mixture of ampicillin (aminobenzyl penicillin, AB-PC) and cloxacillin (methylchlorophenylisoxazolyl penicillin, MCI-PC) showed an excellent bacteri- cidal activity even at low concentrations in which either of the penicillins alone did not have any activity against a clinically isolated strain of Escherichia colt, resistant to both of these penicillins. In this case, the microbial degrada- ion of AB-PC, caused by penicillinase (PC-ase), was strongly inhibited in the presence of MCI-PC. The enzymatic hydrolysis of AB-PC by extracellular nd cell-bound PC-ase, obtained from an AB-PC resistant strain of Staphylo- coccus aureus, was also inhibited in the presence of MCI-PC. Against that, t a under comparable conditions, penicillin G (PC-G) was almost completely destroyed by cell-bound PC-ase from this organism. An in vivo synergism was observed when mixtures of AB-PC and MCI-PC were applied for the treatment of mice challenged with a clinically isolated strain of E. coli resistant to both of these penicillins. Similar results were obtained in the treatment of mice experimentally infected with a strain of Staphylococcus aureus, which is highly resistant to AB-PC, but sensitive to MCI-PC. A decrease in the rate of hydrolysis of methicillin (dimethoxyphenyl penicillin, DMP-PC) by staphylococcal penicillinase (PC-ase) was first noted by Rolinson and his co-workers^. -

Allosteric Drug Transport Mechanism of Multidrug Transporter Acrb
ARTICLE https://doi.org/10.1038/s41467-021-24151-3 OPEN Allosteric drug transport mechanism of multidrug transporter AcrB ✉ Heng-Keat Tam 1,3,4 , Wuen Ee Foong 1,4, Christine Oswald1,2, Andrea Herrmann1, Hui Zeng1 & ✉ Klaas M. Pos 1 Gram-negative bacteria maintain an intrinsic resistance mechanism against entry of noxious compounds by utilizing highly efficient efflux pumps. The E. coli AcrAB-TolC drug efflux pump + 1234567890():,; contains the inner membrane H /drug antiporter AcrB comprising three functionally inter- dependent protomers, cycling consecutively through the loose (L), tight (T) and open (O) state during cooperative catalysis. Here, we present 13 X-ray structures of AcrB in inter- mediate states of the transport cycle. Structure-based mutational analysis combined with drug susceptibility assays indicate that drugs are guided through dedicated transport chan- nels toward the drug binding pockets. A co-structure obtained in the combined presence of erythromycin, linezolid, oxacillin and fusidic acid shows binding of fusidic acid deeply inside the T protomer transmembrane domain. Thiol cross-link substrate protection assays indicate that this transmembrane domain-binding site can also accommodate oxacillin or novobiocin but not erythromycin or linezolid. AcrB-mediated drug transport is suggested to be allos- terically modulated in presence of multiple drugs. 1 Institute of Biochemistry, Goethe-University Frankfurt, Frankfurt am Main, Germany. 2 Sosei Heptares, Steinmetz Building, Granta Park, Great Abington, Cambridge, UK. 3Present -

Cefalexin in the WHO Essential Medicines List for Children Reject
Reviewer No. 1: checklist for application of: Cefalexin In the WHO Essential Medicines List for Children (1) Have all important studies that you are aware of been included? Yes No 9 (2) Is there adequate evidence of efficacy for the proposed use? Yes 9 No (3) Is there evidence of efficacy in diverse settings and/or populations? Yes 9 No (4) Are there adverse effects of concern? Yes 9 No (5) Are there special requirements or training needed for safe/effective use? Yes No 9 (6) Is this product needed to meet the majority health needs of the population? Yes No 9 (7) Is the proposed dosage form registered by a stringent regulatory authority? Yes 9 No (8) What action do you propose for the Committee to take? Reject the application for inclusion of the following presentations of cefalexin: • Tablets/ capsules 250mg • Oral suspensions 125mg/5ml and 125mg/ml (9) Additional comment, if any. In order to identify any additional literature, the following broad and sensitive search was conducted using the PubMed Clinical Query application: (cephalexin OR cefalexin AND - 1 - pediatr*) AND ((clinical[Title/Abstract] AND trial[Title/Abstract]) OR clinical trials[MeSH Terms] OR clinical trial[Publication Type] OR random*[Title/Abstract] OR random allocation[MeSH Terms] OR therapeutic use[MeSH Subheading]) Only one small additional study was identified, which looked at the provision of prophylactic antibiotics in patients presenting to an urban children's hospital with trauma to the distal fingertip, requiring repair.1 In a prospective randomised control trial, 146 patients were enrolled, of which 69 were randomised to the no-antibiotic group, and 66 were randomised to the antibiotic (cefalexin) group. -

16. Questions and Answers
16. Questions and Answers 1. Which of the following is not associated with esophageal webs? A. Plummer-Vinson syndrome B. Epidermolysis bullosa C. Lupus D. Psoriasis E. Stevens-Johnson syndrome 2. An 11 year old boy complains that occasionally a bite of hotdog “gives mild pressing pain in his chest” and that “it takes a while before he can take another bite.” If it happens again, he discards the hotdog but sometimes he can finish it. The most helpful diagnostic information would come from A. Family history of Schatzki rings B. Eosinophil counts C. UGI D. Time-phased MRI E. Technetium 99 salivagram 3. 12 year old boy previously healthy with one-month history of difficulty swallowing both solid and liquids. He sometimes complains food is getting stuck in his retrosternal area after swallowing. His weight decreased approximately 5% from last year. He denies vomiting, choking, gagging, drooling, pain during swallowing or retrosternal pain. His physical examination is normal. What would be the appropriate next investigation to perform in this patient? A. Upper Endoscopy B. Upper GI contrast study C. Esophageal manometry D. Modified Barium Swallow (MBS) E. Direct laryngoscopy 4. A 12 year old male presents to the ER after a recent episode of emesis. The parents are concerned because undigested food 3 days old was in his vomit. He admits to a sensation of food and liquids “sticking” in his chest for the past 4 months, as he points to the upper middle chest. Parents relate a 10 lb (4.5 Kg) weight loss over the past 3 months. -

Clinical Review (Cubicin)
Clinical Review Amol Purandare, MD NDA 021572 Cubicin (Daptomycin for injection) CLINICAL REVIEW Application Type NDA supplement Application Number(s) 21572 Priority or Standard Priority Submit Date(s) June 30, 2016 Received Date(s) June 30, 2016 PDUFA Goal Date March 30, 2017 (Major amendment) Division / Office DAIP/OAP Reviewer Name(s) Amol Purandare, MD Review Completion Date March 23, 2017 Established Name Daptomycin (Proposed) Trade Name Cubicin Therapeutic Class Cyclic Lipopeptide Applicant Cubist Pharmaceuticals Formulation(s) Injection Dosing Regimen 5 mg/kg (12-<18 years), 7 mg/kg (7-11 years), 9 mg/kg (2-6 years), and 10 mg/kg (1-< 2 years) Indication(s) Complicated Skin and Skin Structure Infections 1 Reference ID: 4075320 Clinical Review Amol Purandare, MD NDA 021572 Cubicin (Daptomycin for injection) Intended Population(s) Ages 1 year to <18 years Table of Contents 1 RECOMMENDATIONS/RISK BENEFIT ASSESSMENT..........................................6 1.1 Recommendation on Regulatory Action ..............................................................6 1.2 Risk Benefit Assessment .....................................................................................6 1.3 Recommendations for Postmarket Risk Evaluation and Mitigation Strategies ....6 1.4 Recommendations for Postmarket Requirements and Commitments.................7 2 INTRODUCTION AND REGULATORY BACKGROUND .........................................7 2.1 Product Information .............................................................................................7 -

The Antibacterial Activity of Cefpodoxime and the Novel Β
Session-198 b SATURDAY-279 The Antibacterial Activity of Cefpodoxime and the Novel -lactamase Inhibitor ETX1317 Against Recent Clinical Isolates of b-lactamase-producing Enterobacteriaceae Entasis Therapeutics S. McLeod1, M. Hackel2, R. Badal2, A. Shapiro1, J. Mueller1, R. Tommasi1, and A. Miller1 1-781-810-0120 1Entasis Therapeutics, Waltham, MA and 2IHMA, International Health Management Associates, Schaumburg, IL USA www.entasistx.com Abstract In vitro activity of ETX1317 vs. comparator BLIs Cumulative activity vs. 911 ESBL-enriched Enterobacteriaceae from 2013-2015 Activity vs. 35 sequenced KPC+ and/or MBL+ Enterobacteriaceae MIC (mg/L) Background β-lactamase inhibition (IC50, µM) Strain ID Species encoded bla genes IPM CAZ-AVI CPD-ETX1317 ETX1317 ETX1317 is a novel, diazabicyclooctenone inhibitor of serine β-lactamases that Number (cumulative %) of isolates inhibited at MIC (mg/L) Class A Class C Class D Drug %S* ARC3528*¥ E. cloacae AmpC [∆308-313(SKVALA)] 0.25 32 0.125 4 restores β-lactam activity against multidrug-resistant Enterobacteriaceae. ETX0282, < 0.03 0.06 0.12 0.25 0.5 1 2 4 8 16 32 > 32 ARC4165*¥ C. freundii CMY-2; AmpC [N366Y]; TEM-1; SHV-5 2 32 ≤0.03 4 the oral prodrug of ETX1317, is currently under investigation in combination with BLI CTX-M-15 SHV-5 KPC-2 TEM-1 AmpC* P99 OXA-24/40 OXA-48 0 5 6 14 19 34 20 27 17 18 18 733 3 CPD 10.8 ARC6479* K. oxytoca NDM-1 16 >32 32 32 cefpodoxime proxetil (CPDP), which is hydrolyzed in vivo to release cefpodoxime 0% 0.5% 1% 3% 5% 9% 11% 14% 16% 18% 20% 100% (CPD). -

B-Lactams: Chemical Structure, Mode of Action and Mechanisms of Resistance
b-Lactams: chemical structure, mode of action and mechanisms of resistance Ru´ben Fernandes, Paula Amador and Cristina Prudeˆncio This synopsis summarizes the key chemical and bacteriological characteristics of b-lactams, penicillins, cephalosporins, carbanpenems, monobactams and others. Particular notice is given to first-generation to fifth-generation cephalosporins. This review also summarizes the main resistance mechanism to antibiotics, focusing particular attention to those conferring resistance to broad-spectrum cephalosporins by means of production of emerging cephalosporinases (extended-spectrum b-lactamases and AmpC b-lactamases), target alteration (penicillin-binding proteins from methicillin-resistant Staphylococcus aureus) and membrane transporters that pump b-lactams out of the bacterial cell. Keywords: b-lactams, chemical structure, mechanisms of resistance, mode of action Historical perspective Alexander Fleming first noticed the antibacterial nature of penicillin in 1928. When working with Antimicrobials must be understood as any kind of agent another bacteriological problem, Fleming observed with inhibitory or killing properties to a microorganism. a contaminated culture of Staphylococcus aureus with Antibiotic is a more restrictive term, which implies the the mold Penicillium notatum. Fleming remarkably saw natural source of the antimicrobial agent. Similarly, under- the potential of this unfortunate event. He dis- lying the term chemotherapeutic is the artificial origin of continued the work that he was dealing with and was an antimicrobial agent by chemical synthesis [1]. Initially, able to describe the compound around the mold antibiotics were considered as small molecular weight and isolates it. He named it penicillin and published organic molecules or metabolites used in response of his findings along with some applications of penicillin some microorganisms against others that inhabit the same [4]. -

Who Expert Committee on Specifications for Pharmaceutical Preparations
WHO Technical Report Series 902 WHO EXPERT COMMITTEE ON SPECIFICATIONS FOR PHARMACEUTICAL PREPARATIONS A Thirty-sixth Report aA World Health Organization Geneva i WEC Cover1 1 1/31/02, 6:35 PM The World Health Organization was established in 1948 as a specialized agency of the United Nations serving as the directing and coordinating authority for international health matters and public health. One of WHO’s constitutional functions is to provide objective and reliable information and advice in the field of human health, a responsibility that it fulfils in part through its extensive programme of publications. The Organization seeks through its publications to support national health strat- egies and address the most pressing public health concerns of populations around the world. To respond to the needs of Member States at all levels of development, WHO publishes practical manuals, handbooks and training material for specific categories of health workers; internationally applicable guidelines and standards; reviews and analyses of health policies, programmes and research; and state-of-the-art consensus reports that offer technical advice and recommen- dations for decision-makers. These books are closely tied to the Organization’s priority activities, encompassing disease prevention and control, the development of equitable health systems based on primary health care, and health promotion for individuals and communities. Progress towards better health for all also demands the global dissemination and exchange of information that draws on the knowledge and experience of all WHO’s Member countries and the collaboration of world leaders in public health and the biomedical sciences. To ensure the widest possible availability of authoritative information and guidance on health matters, WHO secures the broad international distribution of its publica- tions and encourages their translation and adaptation.