Physical Assessment for Pharmacists
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Stethoscope: Some Preliminary Investigations
695 ORIGINAL ARTICLE The stethoscope: some preliminary investigations P D Welsby, G Parry, D Smith Postgrad Med J: first published as on 5 January 2004. Downloaded from ............................................................................................................................... See end of article for Postgrad Med J 2003;79:695–698 authors’ affiliations ....................... Correspondence to: Dr Philip D Welsby, Western General Hospital, Edinburgh EH4 2XU, UK; [email protected] Submitted 21 April 2003 Textbooks, clinicians, and medical teachers differ as to whether the stethoscope bell or diaphragm should Accepted 30 June 2003 be used for auscultating respiratory sounds at the chest wall. Logic and our results suggest that stethoscope ....................... diaphragms are more appropriate. HISTORICAL ASPECTS note is increased as the amplitude of the sound rises, Hippocrates advised ‘‘immediate auscultation’’ (the applica- resulting in masking of higher frequency components by tion of the ear to the patient’s chest) to hear ‘‘transmitted lower frequencies—‘‘turning up the volume accentuates the sounds from within’’. However, in 1816 a French doctor, base’’ as anyone with teenage children will have noted. Rene´The´ophile Hyacinth Laennec invented the stethoscope,1 Breath sounds are generated by turbulent air flow in the which thereafter became the identity symbol of the physician. trachea and proximal bronchi. Airflow in the small airways Laennec apparently had observed two children sending and alveoli is of lower velocity and laminar in type and is 6 signals to each other by scraping one end of a long piece of therefore silent. What is heard at the chest wall depends on solid wood with a pin, and listening with an ear pressed to the conductive and filtering effect of lung tissue and the the other end.2 Later, in 1816, Laennec was called to a young characteristics of the chest wall. -

Myocardial Hamartoma As a Cause of VF Cardiac Arrest in an Infant a Frampton, L Gray, S Bell
590 CASE REPORTS Emerg Med J: first published as 10.1136/emj.2003.009951 on 26 July 2005. Downloaded from Myocardial hamartoma as a cause of VF cardiac arrest in an infant A Frampton, L Gray, S Bell ............................................................................................................................... Emerg Med J 2005;22:590–591. doi: 10.1136/emj.2003.009951 ardiac arrests in children are fortunately rare and the patients. However a review by Young et al2 found that the presenting cardiac rhythm is often asystole. However, survival to hospital discharge in infants and children Cventricular fibrillation (VF) can occur and may respond presenting with VF/VT was of the order of 30%, compared favourably to defibrillation. with only 5% of patients whose initial presenting rhythm was asystole. VF has also been demonstrated to be relatively more CASE REPORT common in infants than any other paediatric age group A 7 month old girl was sitting in her high chair when she was (p,0.006).1 One study of over 500 000 children presenting to witnessed by her parents to collapse suddenly at 1707 hours. an ED over a period of 5 years found VF to be the third most They attempted cardiopulmonary resuscitation (CPR) and the common presenting cardiac arrhythmia of any origin in ambulance crew arrived 7 minutes later, the cardiac monitor infants below the age of 1 year.1 It has been suggested that a displaying VF. No defibrillation or medications were admi- subgroup of patients (those ,1 year old) that would benefit nistered and she was rapidly transferred to her nearest from early defibrillation can be identified.2 emergency department (ED), arriving at 1723. -
Automated Classification of Medical Percussion Signals for the Diagnosis of Pulmonary Injuries Bhuiyan Md Moinuddin Universty of Windsor
University of Windsor Scholarship at UWindsor Electronic Theses and Dissertations 2013 Automated Classification of Medical Percussion Signals for the Diagnosis of Pulmonary Injuries Bhuiyan Md Moinuddin Universty of Windsor Follow this and additional works at: http://scholar.uwindsor.ca/etd Recommended Citation Md Moinuddin, Bhuiyan, "Automated Classification of Medical Percussion Signals for the Diagnosis of Pulmonary Injuries" (2013). Electronic Theses and Dissertations. Paper 4941. This online database contains the full-text of PhD dissertations and Masters’ theses of University of Windsor students from 1954 forward. These documents are made available for personal study and research purposes only, in accordance with the Canadian Copyright Act and the Creative Commons license—CC BY-NC-ND (Attribution, Non-Commercial, No Derivative Works). Under this license, works must always be attributed to the copyright holder (original author), cannot be used for any commercial purposes, and may not be altered. Any other use would require the permission of the copyright holder. Students may inquire about withdrawing their dissertation and/or thesis from this database. For additional inquiries, please contact the repository administrator via email ([email protected]) or by telephone at 519-253-3000ext. 3208. Automated Classification of Medical Percussion Signals for the Diagnosis of Pulmonary Injuries By Md Moinuddin Bhuiyan A Dissertation Submitted to the Faculty of Graduate Studies through the Department of Electrical and Computer Engineering in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy at the University of Windsor Windsor, Ontario, Canada 2013 © 2013, Md Moinuddin Bhuiyan All Rights Reserved. No part of this document may be reproduced, stored or otherwise retained in a retrieval system or transmitted in any form, on any medium by any means without prior written permission of the author. -

Practical Cardiac Auscultation
LWW/CCNQ LWWJ306-08 March 7, 2007 23:32 Char Count= Crit Care Nurs Q Vol. 30, No. 2, pp. 166–180 Copyright c 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins Practical Cardiac Auscultation Daniel M. Shindler, MD, FACC This article focuses on the practical use of the stethoscope. The art of the cardiac physical exam- ination includes skillful auscultation. The article provides the author’s personal approach to the patient for the purpose of best hearing, recognizing, and interpreting heart sounds and murmurs. It should be used as a brief introduction to the art of auscultation. This article also attempts to illustrate heart sounds and murmurs by using words and letters to phonate the sounds, and by presenting practical clinical examples where auscultation clearly influences cardiac diagnosis and treatment. The clinical sections attempt to go beyond what is available in standard textbooks by providing information and stethoscope techniques that are valuable and useful at the bedside. Key words: auscultation, murmur, stethoscope HIS article focuses on the practical use mastered at the bedside. This article also at- T of the stethoscope. The art of the cardiac tempts to illustrate heart sounds and mur- physical examination includes skillful auscul- murs by using words and letters to phonate tation. Even in an era of advanced easily avail- the sounds, and by presenting practical clin- able technological bedside diagnostic tech- ical examples where auscultation clearly in- niques such as echocardiography, there is still fluences cardiac diagnosis and treatment. We an important role for the hands-on approach begin by discussing proper stethoscope selec- to the patient for the purpose of evaluat- tion and use. -
Pleurisy Dry and Exudative: Symptoms and Syndromes Based on Clinical-Instrumental and Laboratory Methods of Study
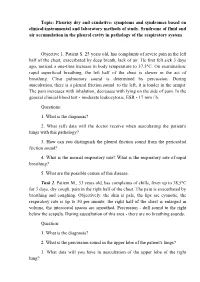
Topic: Pleurisy dry and exudative: symptoms and syndromes based on clinical-instrumental and laboratory methods of study. Syndrome of fluid and air accumulation in the pleural cavity in pathology of the respiratory system Objective 1. Patient S. 25 years old, has complaints of severe pain in the left half of the chest, exacerbated by deep breath, lack of air. He first felt sick 3 days ago, noticed a one-time increase in body temperature to 37,5°C. On examination: rapid superficial breathing, the left half of the chest is slower in the act of breathing. Clear pulmonary sound is determined by percussion. During auscultation, there is a pleural friction sound to the left, it is louder in the armpit. The pain increases with inhalation, decreases with lying on the side of pain. In the general clinical blood test - moderate leukocytosis, ESR - 17 mm / h. Questions: 1. What is the diagnosis? 2. What (all) data will the doctor receive when auscultating the patient's lungs with this pathology? 3. How can you distinguish the pleural friction sound from the pericardial friction sound? 4. What is the normal respiratory rate? What is the respiratory rate of rapid breathing? 5. What are the possible causes of this disease. Task 2. Patient M., 33 years old, has complaints of chills, fever up to 38,5°C for 3 days, dry cough, pain in the right half of the chest. The pain is exacerbated by breathing and coughing. Objectively: the skin is pale, the lips are cyanotic, the respiratory rate is up to 30 per minute, the right half of the chest is enlarged in volume, the intercostal spaces are smoothed. -

Review of Systems
code: GF004 REVIEW OF SYSTEMS First Name Middle Name / MI Last Name Check the box if you are currently experiencing any of the following : General Skin Respiratory Arthritis/Rheumatism Abnormal Pigmentation Any Lung Troubles Back Pain (recurrent) Boils Asthma or Wheezing Bone Fracture Brittle Nails Bronchitis Cancer Dry Skin Chronic or Frequent Cough Diabetes Eczema Difficulty Breathing Foot Pain Frequent infections Pleurisy or Pneumonia Gout Hair/Nail changes Spitting up Blood Headaches/Migraines Hives Trouble Breathing Joint Injury Itching URI (Cold) Now Memory Loss Jaundice None Muscle Weakness Psoriasis Numbness/Tingling Rash Obesity Skin Disease Osteoporosis None Rheumatic Fever Weight Gain/Loss None Cardiovascular Gastrointestinal Eyes - Ears - Nose - Throat/Mouth Awakening in the night smothering Abdominal Pain Blurring Chest Pain or Angina Appetite Changes Double Vision Congestive Heart Failure Black Stools Eye Disease or Injury Cyanosis (blue skin) Bleeding with Bowel Movements Eye Pain/Discharge Difficulty walking two blocks Blood in Vomit Glasses Edema/Swelling of Hands, Feet or Ankles Chrohn’s Disease/Colitis Glaucoma Heart Attacks Constipation Itchy Eyes Heart Murmur Cramping or pain in the Abdomen Vision changes Heart Trouble Difficulty Swallowing Ear Disease High Blood Pressure Diverticulosis Ear Infections Irregular Heartbeat Frequent Diarrhea Ears ringing Pain in legs Gallbladder Disease Hearing problems Palpitations Gas/Bloating Impaired Hearing Poor Circulation Heartburn or Indigestion Chronic Sinus Trouble Shortness -

Review of Systems – Return Visit Have You Had Any Problems Related to the Following Symptoms in the Past Month? Circle Yes Or No
REVIEW OF SYSTEMS – RETURN VISIT HAVE YOU HAD ANY PROBLEMS RELATED TO THE FOLLOWING SYMPTOMS IN THE PAST MONTH? CIRCLE YES OR NO Today’s Date: ______________ Name: _______________________________ Date of Birth: __________________ GENERAL GENITOURINARY Fatigue Y N Blood in Urine Y N Fever / Chills Y N Menstrual Irregularity Y N Night Sweats Y N Painful Menstrual Cycle Y N Weight Gain Y N Vaginal Discharge Y N Weight Loss Y N Vaginal Dryness Y N EYES Vaginal Itching Y N Vision Changes Y N Painful Sex Y N EAR, NOSE, & THROAT SKIN Hearing Loss Y N Hair Loss Y N Runny Nose Y N New Skin Lesions Y N Ringing in Ears Y N Rash Y N Sinus Problem Y N Pigmentation Change Y N Sore Throat Y N NEUROLOGIC BREAST Headache Y N Breast Lump Y N Muscular Weakness Y N Tenderness Y N Tingling or Numbness Y N Nipple Discharge Y N Memory Difficulties Y N CARDIOVASCULAR MUSCULOSKELETAL Chest Pain Y N Back Pain Y N Swelling in Legs Y N Limitation of Motion Y N Palpitations Y N Joint Pain Y N Fainting Y N Muscle Pain Y N Irregular Heart Beat Y N ENDOCRINE RESPIRATORY Cold Intolerance Y N Cough Y N Heat Intolerance Y N Shortness of Breath Y N Excessive Thirst Y N Post Nasal Drip Y N Excessive Amount of Urine Y N Wheezing Y N PSYCHOLOGY GASTROINTESTINAL Difficulty Sleeping Y N Abdominal Pain Y N Depression Y N Constipation Y N Anxiety Y N Diarrhea Y N Suicidal Thoughts Y N Hemorrhoids Y N HEMATOLOGIC / LYMPHATIC Nausea Y N Easy Bruising Y N Vomiting Y N Easy Bleeding Y N GENITOURINARY Swollen Lymph Glands Y N Burning with Urination Y N ALLERGY / IMMUNOLOGY Urinary -

Auscultation of Abdominal Arterial Murmurs
Auscultation of abdominal arterial murmurs C. ARTHUR MYERS, D.O.,° Flint, Michigan publications. Goldblatt's4 work on renal hyperten- sion has stimulated examiners to begin performing The current interest in the diagnostic value of ab- auscultation for renal artery bruits in their hyper- dominal arterial bruits is evidenced by the number tensive patients. of papers and references to the subject appearing in Stenosis, either congenital or acquired, and aneu- the recent literature. When Vaughan and Thoreki rysms are responsible for the vast majority of audi- published an excellent paper on abdominal auscul- ble renal artery bruits (Fig. 2). One should be tation in 1939, the only reference they made to highly suspicious of a renal artery defect in a hy- arterial murmurs was that of the bruit of abdominal pertensive patient with an epigastric murmur. Moser aortic aneurysm. In more recent literature, however, and Caldwell5 have produced the most comprehen- there is evidence of increased interest in auscultat- sive work to date on auscultation of the abdomen ing the abdomen for murmurs arising in the celiac, in renal artery disease. In their highly selective superior mesenteric, splenic, and renal arteries. series of 50 cases of abdominal murmurs in which The purpose of this paper is to review some of aortography was performed, renal artery disease the literature referable to the subject of abdominal was diagnosed in 66 per cent of cases. Their con- murmurs, to present some cases, and to stimulate clusions were that when an abdominal murmur of interest in performing auscultation for abdominal high pitch is found in a patient with hypertension, bruits as a part of all physical examinations. -

How to Do Chest Physical Therapy (CPT): Children, Adolescents and Adults
How to Do Chest Physical Therapy (CPT) Children, Adolescents, and Adults ©(2001, 2003, 2009) The Emily Center, Phoenix Children’s Hospital 1 2 ©(2001, 2003, 2009) The Emily Center, Phoenix Children’s Hospital Name of Child: Date:____________________ How to Do Chest Physical Therapy (CPT) Children, Adolescents, and Adults Your child needs a treatment called Chest Physical Therapy or CPT. CPT is also called Percussion and Postural Drainage (P & PD). Read this booklet to learn what CPT is and how to use it to help your child. What is CPT? Chest Physical Therapy (CPT) is something you can do to help your child breathe better. Sometimes there is too much mucus, or it is too thick. It blocks the air from moving in and out of your child’s lungs. Mucus makes it hard for your child to breathe. Mucus that sits too long in the lungs can also grow germs that can make your child sick. CPT helps to loosen your child’s mucus, so your child can cough it up. Think about how you would take Jell-O out of a mold. You tilt the mold over, then shake it and tap it to loosen the Jell-O . Mucus is like that Jell-O , and CPT helps to get it out. ©(2001, 2003, 2009) The Emily Center, Phoenix Children’s Hospital 3 Words to Learn Airways Air moves through these and into your lungs. The airways of the nose and throat lead to the big airways in the chest. The big airways branch off into smaller airways in the lungs. -

Bronchospasm &
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum of asthma severities & describe stepwise asthma management Describe COPD management & how it might differ from that of asthma List the signs of anaphylaxis, concerning features and key steps in management B on ABCDE assessment RR Oxygen saturations Respiratory distress Use of respiratory muscles Tachypnoea Speaking in sentences Cyanosis Tripod position Drooling Stridor Wheeze Respiratory examination Inspection Signs of respiratory distress Pallor Cyanosis Finger clubbing Tremor Chest wall shape Palpation Trachea position Cervical lymphadenopathy Chest expansion Tactile vocal fremitis Respiratory examination Percussion Dullness Hyperresonance Auscultation Breath sounds Vocal resonance 2 zones anteriorly 3 zones posteriorly Axilla Compare right with left Remember to always examine the back! Bronchospasm Constriction of bronchi & bronchioles Caused by: a spasm in the smooth muscles of bronchi and bronchioles an inflammation of the airways excessive production of mucous due to: an allergic reaction irritation caused by mechanical friction of air, overcooling or drying of airways Symptoms Difficulty breathing Wheezing Coughing Dyspnoea Case 1 24 year old female presents by ambulance with a 3 day history of a cough productive of green sputum, coryza, intermittent temperatures and difficulty breathing. -

Intra-Operative Auscultation of Heart and Lungs Sounds: the Importance of Sound Transmission
Intra-Operative Auscultation of more readily when stethoscopes are used. Loeb Heart and Lungs Sounds: (2) has reported that the response time to detect an abnormal value on an intraoperative The Importance of Sound monitor display and it was 61 seconds with 16% Transmission of the abnormal values not being recognized in 5 minutes. Whereas, Copper et al, (3) found the Anthony V. Beran, PhD* meantime between an event and detection with a stethoscope was 34 seconds. This Introduction suggests that changes in cardio-pulmonary function may be detected more readily with a Sometimes we put so much emphasis on stethoscope (1). Auscultation of heart and lung electronic monitoring devices we forget that sounds during perioperative period is useful our own senses often detect things before a only if the Esophageal Stethoscope provides machine can. Seeing condensation in airway strong, clear transmission of the sounds to the device or clear mask can serve to indicate the anesthesia provider. This study evaluates the presence of ventilation before the signal has sound transmission properties of several even reached the equipment. Sometimes the Esophageal Stethoscopes currently available in sense of smell can be the first thing to aid in the the market. detection of a disconnected airway device or circuit. Similarly, in some situations listening for Methods the presence of abnormal heart or airway sounds can help detect the onset of critical To evaluate the sound transmission properties incidents quicker than electronic monitors. But of the Esophageal Stethoscopes in vitro study in recent years the art of listening has changed was performed. A system that simulates the in the practice of Anesthesia. -
Documenting History at a Glance
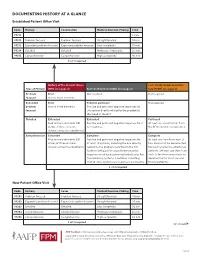
DOCUMENTING HISTORY AT A GLANCE Established Patient Office Visit Code History Examination Medical Decision-Making Time 99211 — — — 5 min. 99212 Problem focused Problem focused Straightforward 10 min. 99213 Expanded problem focused Expanded problem focused Low complexity 15 min. 99214 Detailed Detailed Moderate complexity 25 min. 99215 Comprehensive Comprehensive High complexity 40 min. 2 of 3 required History of the Present Illness Past, Family and/or Social His- Type of History (HPI) (see page 2) Review of Systems (ROS) (see page 2) tory (PFSH) (see page 2) Problem Brief Not required Not required focused One to three elements Expanded Brief Problem pertinent Not required problem One to three elements Positive and pertinent negative responses for focused the system directly related to the problem(s) identified in the HPI. Detailed Extended Extended Pertinent Four or more elements (OR Positive and pertinent negative responses for 2 At least one specific item from status of three or more to 9 systems. the PFSH must be documented. chronic or inactive conditions) Comprehensive Extended Complete Complete Four or more elements (OR Positive and pertinent negative responses for At least one item from each of status of three or more at least 10 systems, including the one directly two areas must be documented chronic or inactive conditions) related to the problem identified in the HPI. for most services to established Systems with positive or pertinent negative patients. (At least one item from responses must be documented individually. For each of the three areas must be the remaining systems, a notation indicating documented for most services that all other systems are negative is permissible.