JAMES MACKENZIE LECTURE 1979 the Happiness Pill? CLIFFORD R
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Role of Synthetic and Natural Inhibitors
Biochimica et Biophysica Acta 1845 (2014) 136–154 Contents lists available at ScienceDirect Biochimica et Biophysica Acta journal homepage: www.elsevier.com/locate/bbacan Review Targeting the STAT3 signaling pathway in cancer: Role of synthetic and natural inhibitors Kodappully Sivaraman Siveen a,1, Sakshi Sikka a,b,1,RohitSuranaa,b, Xiaoyun Dai a, Jingwen Zhang a, Alan Prem Kumar a,b,c,d, Benny K.H. Tan a, Gautam Sethi a,b,⁎, Anupam Bishayee e,⁎⁎ a Department of Pharmacology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore b Cancer Science Institute of Singapore, National University of Singapore, Centre for Translational Medicine, Singapore c School of Biomedical Sciences, Faculty of Health Sciences, Curtin University, Western Australia, Australia d Department of Biological Sciences, University of North Texas, Denton, TX, USA e Department of Pharmaceutical Sciences, School of Pharmacy, American University of Health Sciences, Signal Hill, CA, USA article info abstract Article history: Signal transducers and activators of transcription (STATs) comprise a family of cytoplasmic transcription factors Received 15 August 2013 that mediate intracellular signaling that is usually generated at cell surface receptors and thereby transmit it to Received in revised form 24 December 2013 the nucleus. Numerous studies have demonstrated constitutive activation of STAT3 in a wide variety of human Accepted 27 December 2013 tumors, including hematological malignancies (leukemias, lymphomas, and multiple myeloma) as well as Available online 2 January 2014 diverse solid tumors (such as head and neck, breast, lung, gastric, hepatocellular, colorectal and prostate cancers). There is strong evidence to suggest that aberrant STAT3 signaling promotes initiation and progression of human Keywords: STAT3 cancers by either inhibiting apoptosis or inducing cell proliferation, angiogenesis, invasion, and metastasis. -

El Origen De Syntex, Una Enseñanza Hist¶Orica En La Ciencia Mexicana
El origen de Syntex, una ensen~anza hist¶orica en la ciencia mexicana M. e n C. Fe lip e L e ¶o n Oliva r e s . E s c u e la N a c io n a l P r e p a r a t o r ia P la n t e l \ Ga b in o B a r r e d a " . A v. D e la s To r r e s . S / N . y P r o lo n g a c i¶o n A ld a m a programa de becas. As¶³ fue, que el qu¶³mico Rus- I. Re s u me n . La pre se nte inv e stig a c i¶o n tra ta de la e mpre sa fa r- sell E. Marker de la Universidad Estatal de Pennsyl- ma c ¶e utic a Sy nte x funda da e n M ¶e x ic o , q ue re a - vania, inici¶o sus estudios sobre las hormonas esteroi- liz ¶o una v e rda de ra re v o luc i¶o n mundia l e n e l c a m- des (Lehmann et al., 1973:196). po de la s¶³nte sis o rg ¶a nic a de la s ho rmo na s e ste ro i- Marker plante¶o que el punto clave en la industria de s, a l se r la prime ra e n lo g ra r la s¶³nte sis de pro - g e ste ro na , c o rtiso na y la ba se de l prime r a ntic o n- de las hormonas esteroides estaba en la materia pri- c e ptiv o , utiliz a ndo pa ra e llo la dio sg e nina o bte ni- ma, con esta hip¶otesis, prest¶o atenci¶on a las plan- da de la \ c a be z a de ne g ro " , (Dios corea mex icana) y , lue - tas como fuente barata y abundante de hormonas. -
Gateway to the West Regional Sunday
Sunday July 14-19 Hi 92°F Low 75°F Daily Bulletin Gateway to the West Regional All St. Louis Regional Results: for coming to St. Louis and we’d like www.acbl.org & www.unit143.org, to see you right back here again next Unit 143 includes links to the week’s Daily Bulletins. year. We appreciate that you chose to attend our Regional ’coz we do it all for you! to our Caddies, We appreciate your fine work this week! Jackson Florea Anna Garcia Jenna Percich Lauren Percich Clara Riggio Frank Riggio Katie Seibert Kate Vontz Our Date Back to August 15-21, 2016 Come back and join us next August. Please put us on your Regional tournament calendar today. Charity Pairs Series Raises $ BackStoppers will receive the $$$$ that you helped us raise in the Saturday morning Charity Open Pairs Game and will be added to what Last Chance for Registration Gift & was raised in the Wednesday evening Swiss event. We support this To Pick Up Your Section Top Awards organization to express our appreciation for lives given on behalf of Sunday, from 10:00 – 10:20 AM before the Swiss Team session others. Unit 143 will present the check at their October Sectional. begins, and 30 minutes after the sessions end, will be the last opportunity to pick up your convention card holder and section Thanks for playing in these events and showing your support! top awards. Daily Grin How can you tell if someone is a lousy bridge player? No Peeking, Lew! He has 5 smiling Kibitzers watching him play. -

Carl Djerassi: Chemist and Entrepreneur
Carl Djerassi: Chemist and entrepreneur Eugene Garfield 534 CHEMTECH SEPTEMBER 1983 Much has been said about the scientific entrepreneur. established a precedent for the widely used fragment coding Although the term ordinarily is applied to the person who system employed in the Index Chemicus Registry System has been successful in business—one thinks of Thomas (ICRS) and other systems. Edison or Edwin Land, among others—there also are At the end of the 1940s, much of the excitement centered scientific entrepreneurs in the academic community. It is on the discovery that cortisone could alleviate arthritis not often that one finds a scientist who can fit both symptoms. The chemical was derived from animal bile, but descriptions. To maintain a credible academic existence one initially in amounts too small for treating this chronic, needs enormous dedication and energy; to function in a widespread disease. Scientists around the world were racing scientifically oriented business these qualities as well as to find a more practical method of synthesis. In 1951, significant managerial competence are needed. That rare Djerassi and his team at Syntex won the race; they found a combination of qualities is found in my friend Carl relatively simple way to make cortisone using a readily Djerassi. available raw material, the Mexican yam (2). I recently had the honor of speaking informally at an That same year, Djerassi's team synthesized another unusual event. The numerous friends and collaborators of compound, which received much less attention at the time. Djerassi attended a party celebrating the publication of his They named it "norethisterone," and it was to become the thousandth paper. -

2000 Bridge Bulletin Index
2000 Bridge Bulletin Index ACBL BRIDGE HALL OF FAME. George Rosenkranz named Blackwood Award winner, Meyer Schleifer receives the von Zedtwitz Award C February. Hall of Fame inducts Lou Bluhm, Harry Fishbein, Charles Solomon, George Rosenkranz, Sidney Lazard, Meyer Schleifer and Ira Rubin C October. ACBL BOARD OF DIRECTORS. Highlights from the Boston Board meeting --- February. Election notice C March C May . Highlights of Cincinnati Board meeting C May. Highlights from the Anaheim meeting C October. Election results for 2000 Board C November. ACBL CHARITY FOUNDATION. 2000 Charity Committee appointees named --- February. ACBL CHARITY GAME. Winners C August. ACBL GOODWILL COMMITTEE. 2000 Appointees named --- February. ACBL HALL OF FAME. Rosenkranz wins Blackwood award; Meyer Schleifer is von Zedtwitz award winner C February. ACBL HONORARY MEMBER OF THE YEAR. Chip Martel named for 2000 --- February. ACBL INSTANT MATCHPOINT GAME. Promo C August, September. Results C December. ACBL INTERNATIONAL FUND GAME. Winners C July, November. ACBL PATRON MEMBER LIST. December. ACBL SENIOR GAME. Winners C May. ACE OF CLUBS. Winners of the 1999 contest --- April. AMERICAN BRIDGE ASSOCIATION. Schedule of upcoming national events --- monthly. ANAHEIM NABC. Promos C April --- July. Meltzer squad wins Spingold; Wei-Sender team takes Wagar; District 9 repeats win in GNT-A; District 19 wins GNT-B title; District 13 victorious in GNT-C contest; Zia, Rosenberg top LM Pairs field; Ping, Leung win Red Ribbon; Nugit squad wins Senior Swiss teams C October. Willenken, Silverstein win Fast Open Pairs; Bach and Burgess take IMP Pairs title; Mixed B-A-M winners; 199er Pairs winners; Five-way tie fir Fishbein Trophy; other NABC highlights C November. -

Mannen Och Rotknölen Som Gav Idén Till P-Pillret
n kultur Redaktör: Gabor Hont 08-790 34 80 [email protected] Foto:TropicalsTop ROTKNÖL Rotknölen av mexikansk sköldpaddsjams är oumbärlig för Mannen och rotknölen produktion av halvsyntetiskt som gav idén till p-pillret progesteron. etenskapens historia rymmer ett galleri började den 12 mars 1902 då han föddes på en gård av udda och egensinniga personer som utanför Hagerstown i Maryland. Som 16-åring be- kompromisslöst går sina egna vägar stämde han sig för att bli vetenskapsman, och vid 21 övertygade om sina idéers hållbarhet års ålder tog han en kandidatexamen i organisk kemi om de så har hela världen – eller njugga vid Marylands universitet och året därpå en magis- Vuniversitet och industrier – emot sig. I det här fallet terexamen i fysikalisk kemi. [1]. På väg mot sin dok- handlar det om Russell Earl Marker och hans ban- torsexamen vägrade han att gå några obligatoriska brytande framställning av halvsyntetiskt progeste- kurser i fysikalisk kemi eftersom han inte ville slösa ron som med tiden resulterade i en kaskad av nya lä- bort tid på något han ansåg sig redan kunna. Det blev kemedel mot till exempel astma, reumatism, ämnes- FORSKARE en schism; universitetet vägrade att specialanpassa omsättningssjukdomar, brännskador, allergier, can- Russell Earl hans studier och han varnades för att i evig tid få sit- cer och allvarliga infektioner. Markers arbete lade Marker, som ta och analysera urin om han inte följde regelverket. också grunden för lanseringen av p-piller på 1960-ta- han såg ut un- Marker lyssnade inte på det örat – i stället lämnade let och infriade den mångtusenåriga önskan om der sina år vid han universitetet utan att avlägga någon doktors- barnbegränsning. -

The 2011 Grand National Champs
Monday, July 25, 2011 Volume 83, Number 4 Daily Bulletin 83rd North American Bridge Championships Editors: Brent Manley and Paul Linxwiler The 2011 Grand National Champs Morehead Championship Flight Trailing by 16 IMPs with three boards to go, the District 9 team captained by Warren Spector outscored their District 6 opponents 28-0 on two boards Per-Olla Cullin and Peter Bertheau. to pull out a 140-128 win in the Grand National Teams Swedes rally to win Championship Flight. von Zedtwitz LM Even after picking up an Per-Olla Cullin and Peter Bertheau, both 11-IMP swing on board 62 of members of Sweden’s Bermuda Bowl team, posted 64, the Spector team still trailed Winners of the GNT Championship Flight: Gary Cohler, Michael a 60% game in the second final session of the von by 5 IMPs, but the next-to-last Becker, Warren Spector, Jeff Meckstroth, Eric Rodwell and David Zedtwitz Life Master Pairs to win the event by less continued on page 5 Berkowitz. than a board. continued on page 5 Goldman Flight A The District 14 team captained by Kurt Schaeffer jumped out to an early lead and maintained it throughout to win a relatively close match and the championship in the Goldman Flight A of the Grand National Teams. The runners-up are the District 24 team captained by Igor Savchenko. The final score was 109-93. The winners, all from Minnesota, are Schaeffer, a medical review Bruce LM winners Howard Engle and Mark specialist; his partner, Kerry Weisman Holloway, who is in pharmaceutical Winners of the Goldman Flight A of the Grand National sales; Bjorgvin Kristinsson, a “full- Chicago duo wins Teams: Kerry Holloway, Kurt Schaeffer, Keith Connolly and Bjorgvin Kristinsson continued on page 5 Bruce LM Howard Engle and Mark Weisman of the Sheinwold Chicago area came to the Toronto NABC to Flight B represent District 13 in the Grand National Teams Flight A. -

Potential of Guggulsterone, a Farnesoid X Receptor Antagonist, In
Exploration of Targeted Anti-tumor Therapy Open Access Review Potential of guggulsterone, a farnesoid X receptor antagonist, in the prevention and treatment of cancer Sosmitha Girisa , Dey Parama , Choudhary Harsha , Kishore Banik , Ajaikumar B. Kunnumakkara* Cancer Biology Laboratory and DBT-AIST International Center for Translational and Environmental Research (DAICENTER), Department of Biosciences and Bioengineering, Indian Institute of Technology Guwahati, Guwahati, Assam 781039, India *Correspondence: Ajaikumar B. Kunnumakkara, Cancer Biology Laboratory and DBT-AIST International Center for Translational and Environmental Research (DAICENTER), Department of Biosciences and Bioengineering, Indian Institute of Technology Guwahati, Guwahati, Assam 781039, India. [email protected]; [email protected] Academic Editor: Gautam Sethi, National University of Singapore, Singapore Received: August 8, 2020 Accepted: September 14, 2020 Published: October 30, 2020 Cite this article: Girisa S, Parama D, Harsha C, Banik K, Kunnumakkara AB. Potential of guggulsterone, a farnesoid X receptor antagonist, in the prevention and treatment of cancer. Explor Target Antitumor Ther. 2020;1:313-42. https://doi.org/10.37349/ etat.2020.00019 Abstract Cancer is one of the most dreadful diseases in the world with a mortality of 9.6 million annually. Despite the advances in diagnosis and treatment during the last couple of decades, it still remains a serious concern due to the limitations associated with currently available cancer management strategies. Therefore, alternative strategies are highly required to overcome these glitches. The importance of medicinal plants as primary healthcare has been well-known from time immemorial against various human diseases, including cancer. Commiphora wightii that belongs to Burseraceae family is one such plant which has been used to cure various ailments in traditional systems of medicine. -

Progestin - Wikipedia, the Free Encyclopedia
Progestin - Wikipedia, the free encyclopedia http://en.wikipedia.org/wiki/Progestin From Wikipedia, the free encyclopedia A progestin is a synthetic[1] progestogen that has progestinic effects similar to progesterone. [2] The two most common uses of progestins are for hormonal contraception (either alone or with an estrogen), and to prevent endometrial hyperplasia from unopposed estrogen in hormone replacement therapy. Progestins are also used to treat secondary amenorrhea, dysfunctional uterine bleeding and endometriosis, and as palliative treatment of endometrial cancer, renal cell carcinoma, breast cancer, and prostate cancer. High-dose megestrol acetate is used to treat anorexia, cachexia, and AIDS-related wasting. Progesterone (or sometimes the progestin dydrogesterone or 17α-hydroxyprogesterone caproate) is used for luteal support in IVF protocols, questionably for treatment of recurrent pregnancy loss, and for prevention of preterm birth in pregnant women with a history of at least one spontaneous preterm birth.[3] They are also used in judicial chemical castration of sex offenders as well as a treatment options for those suffering from paraphilia. Co-inventor Luis E. Miramontes's signed laboratory notebook. October 15, 1951 1 History 2 Examples 3 Methods of progestin-based contraception 4 See also 5 References The recognition of progesterone's ability to suppress ovulation during pregnancy spawned a search for a similar hormone that could bypass the problems associated with administering progesterone (low bioavailability when administered -
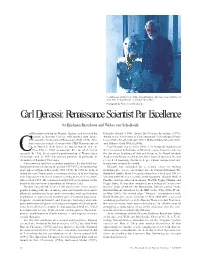
Carl Djerassi, Pictured Here with Artwork from His Collection
Carl Djerassi, pictured here with artwork from his collection. This sculpture, by artist Niki de Saint Phalle, is entitled “Wise Man.” Photograph by Walter van Schalkwijk. Carl Djerassi: Renaissance Scientist Par Excellence by Krishnan Rajeshwar and Walter van Schalkwijk arl Djerassi was born in Vienna, Austria, and received his Fritzsche Award (1960), Award for Creative Invention (1973), education at Kenyon College (AB summa cum laude, Award in the Chemistry of Contemporary Technological Prob- 1942) and the University of Wisconsin (PhD, 1945). After lems (1983), Priestley Medal (1992), Willard Gibbs Medal (1997), four years as research chemist with CIBA Pharmaceutical and Othmer Gold Medal (2000). Co. in Summit, New Jersey, he joined Syntex, S.A., in Carl Djerassi is a member of the U.S. National Academy of Mexico City in 1949 as associate director of chemical Sciences and of its Institute of Medicine, as well as a member of Cresearch. In 1952, he accepted a professorship at Wayne State the American Academy of Arts and Sciences, the Royal Swedish University, and in 1959 his current position as professor of Academy of Sciences, and many other learned societies. He has chemistry at Stanford University. received 18 honorary doctorate degrees from various academic Concurrently with his academic positions, he also held var- institutions around the world. ious posts at Syntex during the period 1957-1972, including that Djerassi has embarked on a second career in writing of president of Syntex Research (1968-1972). In 1968, he helped including five “science-in-fiction” novels: Cantor’s Dilemma; The found Zoecon Corporation, a company dedicated to developing Bourbaki Gambit; Marx, Deceased; Menachem’s Seed; and NO. -

International Historic Chemical Landmark Acclaims Success of Mexican Steroid Industry and a U.S
Journal of the Mexican Chemical Society ISSN: 1870-249X [email protected] Sociedad Química de México México Raber, Linda Steroid industry honored. International historic chemical landmark acclaims success of mexican steroid industry and a U.S. chemist who made it possible Journal of the Mexican Chemical Society, vol. 43, núm. 6, noviembre-diciembre, 1999, pp. 235-237 Sociedad Química de México Distrito Federal, México Available in: http://www.redalyc.org/articulo.oa?id=47543610 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Revista de la Sociedad Química de México, Vol. 43, Núm. 6 (1999) 235-237 Noticias Steroid Industry Honored† International Historic Chemical Landmark Acclaims Success of Mexican Steroid Industry and a U.S. Chemist Who Made it Possible Linda Raber American Chemical Society 1155-16th St., N.W, Washington, D.C. 20036. U.S.A. “There are more stories told about Russell Marker than any he founded in Mexico City with Emeric Somlo and Federico other chemist. Although perhaps many of these stories are A. Lehmann. apocryphal, they are so fascinating that most of us cannot bear “This low-cost progesterone eventually became the pre- to stop repeating them. This is the oral history of our profes- ferred precursor in the industrial preparation of the anti- sion that we pass to our colleagues and our students. They are inflammatory drug cortisone. In 1951, Syntex researchers syn- the campfire stories that bind our profession together” – thesized the first useful oral contraceptive from Marker’s start- Steven M. -

Cancer Risk an Unfortunate Truth
Breast Cancer May 2013 Issue 30 RO F ACTs, MYTHs, VI N Cancer Risk N M an E E CHOICEs N and T unfortunate(excerpts from truth P Anand et al, 2008) GENES diet is linked to cancer deaths in as many as 70% of colorectal cancer cases. How diet contributes to cancer is not fully understood. Most carcinogens that are ingested, such as nitrates, nitrosamines, pesticides, and dioxins, come from food or food additives or from cooking. INDEX Various phytochemicals have been identified in RESEARCH PARTNERS fruits, vegetables, spices, and grains that exhibit chemopreventive potential, and numerous studies Cancer risk.....................................1 have shown that a proper diet can help protect Addictive junk food......,..................7 against cancer. Although all cancers are a result of multiple COMMUNITY PARTNERS mutations, these mutations are due to interaction with the environment. Coffee Talks..................................8 Sunchokes.......................................9 Up to 10% of total cancer cases may be Crossword puzzle.........................10 induced by radiation, both ionizing and nonionizing, typically from radioactive substances and ultraviolet Nutrient Density............................12 (UV), pulsed electromagnetic fields. Yoga Pose......................................13 Junk food and brain activity......14 Heavy consumption of red meat is a risk factor Just 4 fun.......................................15 for colorectal, prostate, bladder, breast, gastric, pancreatic, and oral cancers. Contacts Inflammation may