An Overview of the Food Consumption and Nutrition Situation in Mali
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
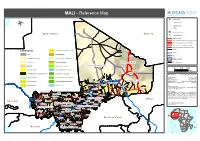
MALI - Reference Map
MALI - Reference Map !^ Capital of State !. Capital of region ® !( Capital of cercle ! Village o International airport M a u r ii t a n ii a A ll g e r ii a p Secondary airport Asphalted road Modern ground road, permanent practicability Vehicle track, permanent practicability Vehicle track, seasonal practicability Improved track, permanent practicability Tracks Landcover Open grassland with sparse shrubs Railway Cities Closed grassland Tesalit River (! Sandy desert and dunes Deciduous shrubland with sparse trees Region boundary Stony desert Deciduous woodland Region of Kidal State Boundary ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Bare rock ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Mosaic Forest / Savanna ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Region of Tombouctou ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 0 100 200 Croplands (>50%) Swamp bushland and grassland !. Kidal Km Croplands with open woody vegetation Mosaic Forest / Croplands Map Doc Name: OCHA_RefMap_Draft_v9_111012 Irrigated croplands Submontane forest (900 -1500 m) Creation Date: 12 October 2011 Updated: -

Evaluation Hydrologique De L'afrique Sub-Saharienne. Pays De L
Banque Mondiale Programme des Nations Unies pour le Développement Banque Africaine de Développement Ministère Français de la Coopération Evaluation Hydrologique de l'Afrique Sub-Saharienne Pays de l'Afrique de l'Ouest Rapport de pays: MALI Juillet 1992 Mott MacDonald BCEOM SOGREAH ORSTOM International Montpellier Grenoble Montpellier Cambridge,UK France France France PREAMBULE Celte étude constitue la troisième tranche de l'évaluation hydrologique régionale de l'Afrique Sub-Saharienne financée par le PNUD (Projet RAF/87/030), la Banque Africaine de Développement, et le Fonds d'Aide et de Coopération de la République Française. L'Etude a porté sur 23 pays de l'Afrique de l'Ouest et a débuté en Septembre 1990. Les pays furent visités par les membres de l'équipe d'étude entre Novembre 1990 et Novembre 1991. Le temps global consacré à chaque pays a été de six semaines en moyenne, dont la moitié au bureau des consultants. Dans 17 pays, ces derniers ont été introduits par le CIEH. L'étude a été organisée de manière à ce que les évaluations soient réalisées par le personnel de MOIT MacDonald International, du BCEOM, de SOGREAH, de l'ORSTOM et de plusieurs consultants nationaux. Dès le début, une attention particulière a été portée à la cohérence de l'approche et à l'homogénéité de l'évaluation. Le projet consistait à évaluer l'état des systèmes de collecte de données hydrologiques existants, et à formuler des recommandations nécessaires à leur amélioration, de manière à assister les pays dans l'établissement ou l'amélioration de bases de données hydrologiques fiables en vue de leur permettre une meilleure planification des programmes et projets de d'aménagement des ressources en eaux superficielles et souterraines. -

340102-Fre.Pdf (433.2Kb)
r 1 RAPPORT DE MISSION [-a mission que nous venons de terminer avait pour but de mener une enquête dans quelques localités du Mali pour avoir une idée sur la vente éventuelle de I'ivermectine au Mali et le suivi de la distribution du médicament par les acteurs sur le terrain. En effet sur ordre de mission No 26/OCPlZone Ouest du3l/01196 avec le véhicule NU 61 40874 nous avons debuté un périple dans les régions de Koulikoro, Ségou et Sikasso et le district de Bamako, en vue de vérifier la vente de l'ivermectine dans les pharmacies, les dépôts de médicament ou avec les marchands ambulants de médicaments. Durant notre périple, nous avons visité : 3 Régions : Koulikoro, Ségou, Sikasso 1 District : Bamako 17 Cercles Koulikoro (06 Cercles), Ségou (05 Cercles), Sikasso (06 Cercles). 1. Koulikoro l. Baraouli 1. Koutiala 2. Kati 2. Ségou 2. Sikasso 3. Kolokani 3. Macina 3. Kadiolo 4. Banamba 4. Niono 4. Bougouni 5. Kangaba 5. Bla 5. Yanfolila 6. Dioila 6. Kolondiéba avec environ Il4 pharmacies et dépôts de médicaments, sans compter les marchands ambulants se trouvant à travers les 40 marchés que nous avons eu à visiter (voir détails en annexe). Malgré notre fouille, nous n'avons pas trouvé un seul comprimé de mectizan en vente ni dans les pharmacies, ni dans les dépôts de produits pharmaceutiques ni avec les marchands ambulants qui ne connaissent d'ailleurs pas le produit. Dans les centres de santé où nous avons cherché à acheter, on nous a fait savoir que ce médicament n'est jamais vendu et qu'il se donne gratuitement à la population. -

FINAL REPORT Quantitative Instrument to Measure Commune
FINAL REPORT Quantitative Instrument to Measure Commune Effectiveness Prepared for United States Agency for International Development (USAID) Mali Mission, Democracy and Governance (DG) Team Prepared by Dr. Lynette Wood, Team Leader Leslie Fox, Senior Democracy and Governance Specialist ARD, Inc. 159 Bank Street, Third Floor Burlington, VT 05401 USA Telephone: (802) 658-3890 FAX: (802) 658-4247 in cooperation with Bakary Doumbia, Survey and Data Management Specialist InfoStat, Bamako, Mali under the USAID Broadening Access and Strengthening Input Market Systems (BASIS) indefinite quantity contract November 2000 Table of Contents ACRONYMS AND ABBREVIATIONS.......................................................................... i EXECUTIVE SUMMARY............................................................................................... ii 1 INDICATORS OF AN EFFECTIVE COMMUNE............................................... 1 1.1 THE DEMOCRATIC GOVERNANCE STRATEGIC OBJECTIVE..............................................1 1.2 THE EFFECTIVE COMMUNE: A DEVELOPMENT HYPOTHESIS..........................................2 1.2.1 The Development Problem: The Sound of One Hand Clapping ............................ 3 1.3 THE STRATEGIC GOAL – THE COMMUNE AS AN EFFECTIVE ARENA OF DEMOCRATIC LOCAL GOVERNANCE ............................................................................4 1.3.1 The Logic Underlying the Strategic Goal........................................................... 4 1.3.2 Illustrative Indicators: Measuring Performance at the -

Policies for Sustainable Mobility and Accessibility in Cities of Mali
Page 1 Policies for sustainable mobility and accessibility in cities of Mali Page 2 ¾ SSATP – Mali - Policies for Sustainable Mobility and Accessibility in Urban Areas – October 2019 Page 3 ¾ SSATP – Mali - Policies for Sustainable Mobility and Accessibility in Urban Areas – October 2019 Policies for sustainable mobility and accessibility in urban areas of Mali An international partnership supported by: Page 4 ¾ SSATP – Mali - Policies for Sustainable Mobility and Accessibility in Urban Areas – October 2019 The SSATP is an international partnership to facilitate policy development and related capacity building in the transport sector in Africa. Sound policies lead to safe, reliable, and cost-effective transport, freeing people to lift themselves out of poverty and helping countries to compete internationally. * * * * * * * The SSATP is a partnership of 42 African countries: Angola, Benin, Burkina Faso, Burundi, Cameroon, Cape Verde, Central African Republic, Chad, Comoros, Congo, Democratic Republic of the Congo, Côte d'Ivoire, Djibouti, Eswatini, Ethiopia, Gabon, The Gambia, Ghana, Guinea, Guinea-Bissau, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritania, Morocco, Mozambique, Namibia, Niger, Nigeria, Rwanda, Senegal, Sierra Leone, South Sudan, Tanzania, Togo, Tunisia, Uganda, Zambia, Zimbabwe; 8 Regional Economic Communities (RECs); 2 African institutions: African Union Commission (AUC) and United Nations Economic Commission for Africa (UNECA); Financing partners for the Third Development Plan: European Commission (main donor), -

Country Travel Risk Summaries
COUNTRY RISK SUMMARIES Powered by FocusPoint International, Inc. Report for Week Ending September 19, 2021 Latest Updates: Afghanistan, Burkina Faso, Cameroon, India, Israel, Mali, Mexico, Myanmar, Nigeria, Pakistan, Philippines, Russia, Saudi Arabia, Somalia, South Sudan, Sudan, Syria, Turkey, Ukraine and Yemen. ▪ Afghanistan: On September 14, thousands held a protest in Kandahar during afternoon hours local time to denounce a Taliban decision to evict residents in Firqa area. No further details were immediately available. ▪ Burkina Faso: On September 13, at least four people were killed and several others ijured after suspected Islamist militants ambushed a gendarme patrol escorting mining workers between Sakoani and Matiacoali in Est Region. Several gendarmes were missing following the attack. ▪ Cameroon: On September 14, at least seven soldiers were killed in clashes with separatist fighters in kikaikelaki, Northwest region. Another two soldiers were killed in an ambush in Chounghi on September 11. ▪ India: On September 16, at least six people were killed, including one each in Kendrapara and Subarnapur districts, and around 20,522 others evacuated, while 7,500 houses were damaged across Odisha state over the last three days, due to floods triggered by heavy rainfall. Disaster teams were sent to Balasore, Bhadrak and Kendrapara districts. Further floods were expected along the Mahanadi River and its tributaries. ▪ Israel: On September 13, at least two people were injured after being stabbed near Jerusalem Central Bus Station during afternoon hours local time. No further details were immediately available, but the assailant was shot dead by security forces. ▪ Mali: On September 13, at least five government soldiers and three Islamist militants were killed in clashes near Manidje in Kolongo commune, Macina cercle, Segou region, during morning hours local time. -

Annuaire Statistique 2015 Du Secteur Développement Rural
MINISTERE DE L’AGRICULTURE REPUBLIQUE DU MALI ----------------- Un Peuple - Un But – Une Foi SECRETARIAT GENERAL ----------------- ----------------- CELLULE DE PLANIFICATION ET DE STATISTIQUE / SECTEUR DEVELOPPEMENT RURAL Annuaire Statistique 2015 du Secteur Développement Rural Juin 2016 1 LISTE DES TABLEAUX Tableau 1 : Répartition de la population par région selon le genre en 2015 ............................................................ 10 Tableau 2 : Population agricole par région selon le genre en 2015 ........................................................................ 10 Tableau 3 : Répartition de la Population agricole selon la situation de résidence par région en 2015 .............. 10 Tableau 4 : Répartition de la population agricole par tranche d'âge et par sexe en 2015 ................................. 11 Tableau 5 : Répartition de la population agricole par tranche d'âge et par Région en 2015 ...................................... 11 Tableau 6 : Population agricole par tranche d'âge et selon la situation de résidence en 2015 ............. 12 Tableau 7 : Pluviométrie décadaire enregistrée par station et par mois en 2015 ..................................................... 15 Tableau 8 : Pluviométrie décadaire enregistrée par station et par mois en 2015 (suite) ................................... 16 Tableau 9 : Pluviométrie enregistrée par mois 2015 ........................................................................................ 17 Tableau 10 : Pluviométrie enregistrée par station en 2015 et sa comparaison à -

Drought and Livestock in Semi-Arid Africa and Southwest Asia
Working Paper 117 DROUGHT AND LIVESTOCK IN SEMI-ARID AFRICA AND SOUTHWEST ASIA Roger Blench Zoë Marriage March 1999 Overseas Development Institute Portland House Stag Place London SW1E 5DP Acknowledgements The first version of this paper and the annotated bibliography was prepared as a keynote document for the FAO-sponsored Electronic Conference ‘Drought and livestock in semi-arid Africa and the Near East’, which took place between July and September 1998. The papers from the conference can be accessed at http://www.fao.org/ag/aga/agap/lps/drought1.htm. The authors are grateful to all those who took part in the conference, and the revision of this document reflects both specific comments on the text and some of the general discussion that formed part of the conference. We would like to thank Andy Catley, Maryam Fuller and Simon Mack for their observations and additional references; we hope their concerns are reflected in this revised text. This working paper is distributed by the Overseas Development Institute (ODI), an independent, non-profit policy research institute, with financial support from the Food and Agriculture Organization of the United Nations (FAO) and the Natural Resources Institute (NRI) under funding from the Department for International Development. Opinions expressed do not necessarily reflect the views of ODI, FAO, NRI or the Department for International Development. Roger Blench ([email protected]) is a Research Fellow, and Zoë Marriage (z.marriage@ odi.org.uk) is a Research Assistant, at the Overseas Development Institute. Editing, index and layout by Paul Mundy, Weizenfeld 4, 51467 Bergisch Gladbach, Germany; [email protected], http://www.netcologne.de/~nc-mundypa ISBN 0 85003 416 7 © Overseas Development Institute 1999 All rights reserved. -

USAID/ Mali SIRA
USAID/ Mali SIRA Selective Integrated Reading Activity Quarterly Report April to June 2018 July 30, 2018 Submitted to USAID/Mali by Education Development Center, Inc. in accordance with Task Order No. AID-688-TO-16-00005 under IDIQC No. AID-OAA-I-14- 00053. This report is made possible by the support of the American People jointly through the United States Agency for International Development (USAID) and the Government of Mali. The contents of this report are the sole responsibility of Education Development Center, Inc. (EDC) and, its partners and do not necessarily reflect the views of USAID or the United States Government. Table of Contents ACRONYMS ...................................................................................................................................... 2 I. Executive Summary ................................................................................................................. 3 II. Key Activities and Results ....................................................................................................... 5 II.A. – Intermediate Result 1: Classroom Early Grade Reading Instruction Improved ........................ 5 II.A.1. Sub-Result 1.1: Student’s access to evidence-based, conflict and gender sensitive, early Grade reading material increased .................................................................................................. 5 II.A.2. Sub IR1.2: Inservice teacher training in evidence-based early Grade reading improved ..... 6 II.A.3. Sub-Result 1.3: Teacher coaching and supervision -

Uva-DARE (Digital Academic Repository)
UvA-DARE (Digital Academic Repository) That Desert is Our Country: Tuareg Rebellions and Competing Nationalisms in Comtemporary Mali (1946-1996) Lecocq, J.S. Publication date 2002 Link to publication Citation for published version (APA): Lecocq, J. S. (2002). That Desert is Our Country: Tuareg Rebellions and Competing Nationalisms in Comtemporary Mali (1946-1996). General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) Download date:27 Sep 2021 VII I al-Jebha al-Jebha Thee Tamasheq rebellion (1990-1993) ) Introduction n Onn 28 June 1990, a group of armed fighters attacked the army barracks andd the Arrondissement office in Tidaghmene, in the Cercle Menaka. Simultaneously,, another group of fighters ambushed a convoy of four cars belongingg to the American NGO World Vision. -

Mardi, Le 8 Décembre 2020
RÉUNION DE COORDINATION DU CLUSTER SÉCURITÉ ALIMENTAIRE DE GAO RÉUNION MENSUELLE DE NOVEMBRE 2020 Mardi, le 8 décembre 2020 TEAMS EN LIGNE NOVEMBRE 2020 QUELQUES RÈGLES AVANT DE COMMENCER o Désactivez votre micro en cliquant sur l'onglet correspondant. Une barre s'affichera dessus 1 pour le mettre en mode "mute". Cliquer dessus lorsque vous souhaitez intervenir. o Pour une meilleure performance réseau, désactivez votre caméra (l'onglet juste à côté du 2 micro). Une barre s'affichera dessus une fois désactivée. o En entrant dans la réunion, veuillez indiquer votre nom, organisation et position dans le chat. 3 Cela facilite l'édition de la liste de présence ainsi que la transparence dans les échanges. o Étant donné que nous sommes nombreux dans la discussion, demandez la parole en envoyant 4 un message dans le chat, ou posez vos questions dans le chat pour organiser les débats. o Le facilitateur guidera les discussions. 5 2 NOVEMBRE 2020 AGENDA 1. BILAN DE LA RÉPONSE EN OCTOBRE 2020 2. SITUATION DES MARCHÉS 3. PRÉSENTATION DES RÉSULTATS DU CADRE HARMONISÉ DE NOVEMBRE 2020 4. SUIVI DES MOUVEMENTS DES POPULATIONS ET DE LA RÉPONSE RRM 5. PIN ET CIBLE 2021 DU CLUSTER : MÉTHODOLOGIE ET DONNÉES 6. DIVERS 3 NOVEMBRE 2020 1. BILAN DE LA RÉPONSE EN OCTOBRE 2020 : ANALYSE DE LA 5W 4 NOVEMBRE 2020 1. BILAN DE LA RÉPONSE EN OCTOBRE 2020 – PARTENAIRES Organisations ACF-E, ACTED, ARCHE NOVA, AVSF, CARE Mali, CICR, CRS, FAO, 12 NRC, PAM, SCI et SOS Sahel Organisations par objectif du Cluster SA : ❑ OBJ1 – Assistance Alimentaire (7) : ACF-E, ACTED, CICR, CRS, NRC, PAM et SCI. -

2016 Country Review
Mali 2016 Country Review http://www.countrywatch.com Table of Contents Chapter 1 1 Country Overview 1 Country Overview 2 Key Data 5 Mali 6 Africa 7 Chapter 2 9 Political Overview 9 History 10 Political Conditions 12 Political Risk Index 66 Political Stability 81 Freedom Rankings 96 Human Rights 108 Government Functions 110 Government Structure 111 Principal Government Officials 121 Leader Biography 122 Leader Biography 122 Foreign Relations 131 National Security 143 Defense Forces 154 Chapter 3 156 Economic Overview 156 Economic Overview 157 Nominal GDP and Components 159 Population and GDP Per Capita 160 Real GDP and Inflation 161 Government Spending and Taxation 162 Money Supply, Interest Rates and Unemployment 163 Foreign Trade and the Exchange Rate 164 Data in US Dollars 165 Energy Consumption and Production Standard Units 166 Energy Consumption and Production QUADS 167 World Energy Price Summary 168 CO2 Emissions 169 Agriculture Consumption and Production 170 World Agriculture Pricing Summary 172 Metals Consumption and Production 173 World Metals Pricing Summary 175 Economic Performance Index 176 Chapter 4 188 Investment Overview 188 Foreign Investment Climate 189 Foreign Investment Index 193 Corruption Perceptions Index 206 Competitiveness Ranking 217 Taxation 226 Stock Market 227 Partner Links 227 Chapter 5 229 Social Overview 229 People 230 Human Development Index 232 Life Satisfaction Index 236 Happy Planet Index 247 Status of Women 256 Global Gender Gap Index 259 Culture and Arts 268 Etiquette 268 Travel Information 269 Diseases/Health Data 280 Chapter 6 287 Environmental Overview 287 Environmental Issues 288 Environmental Policy 288 Greenhouse Gas Ranking 290 Global Environmental Snapshot 301 Global Environmental Concepts 312 International Environmental Agreements and Associations 326 Appendices 350 Bibliography 351 Mali Chapter 1 Country Overview Mali Review 2016 Page 1 of 363 pages Mali Country Overview MALI Located in western Africa, the landlocked Mali is one of the poorest countries in the world.