Variation in the Course and Termination of the Cephalic Vein in the Deltopectoral Triangle
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -
Anatomical Snuffbox
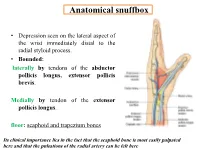
Anatomical snuffbox • Depression seen on the lateral aspect of the wrist immediately distal to the radial styloid process. • Bounded: laterally by tendons of the abductor pollicis longus, extensor pollicis brevis. Medially by tendon of the extensor pollicis longus. floor: scaphoid and trapezium bones Its clinical importance lies in the fact that the scaphoid bone is most easily palpated here and that the pulsations of the radial artery can be felt here Anatomical snuffbox Anatomical snuffbox • Contents: 2) Origin of the 1) The radial artery cephalic vein pass subcutaneously over the snuffbox. 3) Superficial branch of the radial nerve pass subcutaneously over the snuffbox. Blood supply of the hand Anastomoses occur between the radial and ulnar arteries via the superficial and deep palmar arches The Deep palmar arch is formed mainly by the radial artery while the superficial palmar arch is formed mainly by the ulnar artery 3-On entering the palm, it curves laterally behind (deep) the palmar 4-The arch is aponeurosis and in front completed on (superficial) of the long flexor the lateral side tendons forming by the the superficial palmar arch superficial branch of the radial artery. 2-Then it gives off its deep branch of which runs in front of the FR , and joins the radial artery to complete the deep palmar arch 1-Enters the hand anterior (superficial) to the Superficial flexor retinaculum palmar branch of radial artery through Guyon’s canal Radial artery 5-The superficial palmar arch gives off digital arteries from its convexity which pass to the fingers and supply them Superficial palmar arch Deep palmar branch of ulnar artery Superficial palmar branch of radial artery Ulnar artery Radial artery Radial Artery first dorsal interosseous muscle 1-From the floor of the anatomical snuff-box the radial artery leaves the dorsum of the hand by turning forward between the two heads of the first dorsal interosseous muscle. -

Anatomical Variants in the Termination of the Cephalic Vein Stoyan Novakov1*, Elena Krasteva2
Institute of Experimental Morphology, Pathology and Anthropology with Museum Bulgarian Anatomical Society Acta morphologica et anthropologica, 25 (3-4) Sofia • 2018 Anatomical Variants in the Termination of the Cephalic Vein Stoyan Novakov1*, Elena Krasteva2 1 Department of Anatomy, Histology and Embryology, 2Department of Propaedeutics of Surgical Di- seases, Medical Faculty, Medical University of Plovdiv * Corresponding author e-mail: [email protected] Jugulocephalic vein is atavistic structure which is very rare. The low incidence of the variations of the cephalic vein in deltopectoral triangle and its position on the anterior surface of the clavicle and the neck doesn’t make it less important for the clinical practice. Phylo- and ontogenesis explain the formation of the above mentioned variations. We followed the pattern of the cephalic vein in its proximal part and termination to describe possible variations. In this long term study on 140 upper limbs of 70 cadavers, 4 or 2,9% of the cephalic veins were variable. The direct empting of the cephalic vein into internal jugular is an exception with few descriptions at the moment. The rareness of this anatomical variation doesn’t make it less important for clinical practice. It is described as a possible obstacle in catheter implantation, clavicle fractures and creation of arteriovenous fistula in patients on hemodialysis. Key words:cadavers, human anatomy variation, cephalic vein, external jugular vein, jugulocephalic vein Introduction Cephalic vein (CV) belongs to the group of superficial veins of the upper limb. It usually forms over the anatomical snuff-box on the radial side of the wrist from the radial end of the dorsal venous plexus. -

Pectoral Muscles 1. Remove the Superficial Fascia Overlying the Pectoralis Major Muscle (Fig
BREAST, PECTORAL REGION, AND AXILLA LAB (Grant's Dissector (16th Ed.) pp. 28-38) TODAY’S GOALS: 1. Identify the major structural and tissue components of the female breast, including its blood supply. 2. Identify examples of axillary lymph nodes and understand the lymphatic drainage of the breast. 3. Identify the pectoralis major, pectoralis minor, and serratus anterior muscles. Demonstrate their bony attachments, nerve supply, and actions. 4. Identify the walls and associated muscles of the axilla. 5. Identify the axillary sheath, axillary vein, and the 6 major branches of the axillary artery. 6. Identify and trace the cords of the brachial plexus and their branches. DISSECTION NOTES: The donor should be in the supine position. Breast 1. The breast or mammary gland is a modified sweat gland embedded in the superficial fascia overlying the anterior chest wall. Refer to Fig. 2.5A for incisions for reflecting skin of the pectoral region to the mid-arm. Do this bilaterally. Within the superficial fascia in front of the shoulder and along the lateral and lower medial portions of the arm locate the cephalic and basilic veins and preserve these for now. Observe the course of the cephalic vein from the arm into the deltopectoral groove between the deltoid and pectoralis major muscles. 2. For those who have a female donor, mobilize the breast by inserting your fingers behind it within the retromammary space and separate it from the underlying deep fascia of the pectoralis major (see Fig. 2.7). An extension of breast tissue (axillary tail) from the superolateral (upper outer) quadrant often extends around the lateral border of the pectoralis major muscle into the axilla. -

Distal Radial Approach Through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention
Korean Circ J. 2018 Dec;48(12):1131-1134 https://doi.org/10.4070/kcj.2018.0293 pISSN 1738-5520·eISSN 1738-5555 Editorial Distal Radial Approach through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention Jae-Hyung Roh, MD, PhD, and Jae-Hwan Lee , MD, PhD Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea ► See the article “Feasibility of Coronary Angiography and Percutaneous Coronary Intervention via Left Snuffbox Approach” in volume 48 on page 1120. Received: Aug 27, 2018 The anatomical snuffbox, also known as the radial fossa, is a triangular-shaped depression Accepted: Sep 17, 2018 on the radial, dorsal aspect of the hand at the level of the carpal bones. It is clearly observed Figure 1 1)2) Correspondence to when the thumb is extended ( ). The bottom of the snuffbox is supported by carpal Jae-Hwan Lee, MD, PhD bones composed of the scaphoid and trapezium. The medial and lateral borders are bounded Division of Cardiology, Department of Internal by tendons of the extensor pollicis longus and the extensor pollicis brevis, respectively. The Medicine, Chungnam National University proximal border is formed by the styloid process of the radius. Within this narrow triangular Hospital, Chungnam National University space, various structures are located, including the distal radial artery (RA), a branch of the School of Medicine, 282, Munhwa-ro, Jung-gu, radial nerve, and the cephalic vein. Daejeon 35015, Korea. E-mail: [email protected] The anatomy of the hand arteries is illustrated in Figure 2. -

Ultrasound-Guided Access of the Distal Radial Artery at the Anatomical Snuffbox for Catheter-Based Vascular Interventions: a Technical Guide
Title: Ultrasound-guided access of the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: A technical guide. Authors: Anastasia Hadjivassiliou, MBBS, BSc; Ferdinand Kiemeneij, M.D, PhD; Sandeep Nathan, M.D, MSc; Darren Klass, M.D, PhD DOI: 10.4244/EIJ-D-19-00555 Citation: Hadjivassiliou A, Kiemeneij F, Nathan S, Klass D. Ultrasound-guided access of the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: A technical guide. EuroIntervention 2019; Jaa-625 2019, doi: 10.4244/EIJ-D-19-00555 Manuscript submission date: 10 June 2019 Revisions received: 24 July 2019 Accepted date: 01 August 2019 Online publication date: 06 August 2019 Disclaimer: This is a PDF file of a "Just accepted article". This PDF has been published online early without copy editing/typesetting as a service to the Journal's readership (having early access to this data). Copy editing/typesetting will commence shortly. Unforeseen errors may arise during the proofing process and as such Europa Digital & Publishing exercise their legal rights concerning these potential circumstances. Ultrasound-guided access of the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: A technical guide Anastasia Hadjivassiliou, MBBS, BSc1; Ferdinand Kiemeneij, MD, PhD2; Sandeep Nathan, MD, MSc3; Darren Klass, MD, PhD1 1. Department of Interventional Radiology, Vancouver General Hospital, University of British Columbia, Canada 2. Department of Cardiology, Tergooi Hospital, Blaricum, the Netherlands 3. University of Chicago Medicine, Chicago, IL, USA Short title: Ultrasound guided distal radial artery access at the anatomical snuffbox Corresponding author: Dr Darren Klass Department of Radiology, Vancouver General Hospital 899 West 12th Avenue, V5Z 1M9, Vancouver, BC, Canada Email address: [email protected] Disclaimer : As a public service to our readership, this article -- peer reviewed by the Editors of EuroIntervention - has been published immediately upon acceptance as it was received. -

The Clinical Anatomy of the Cephalic Vein in the Deltopectoral Triangle
Folia Morphol. Vol. 67, No. 1, pp. 72–77 Copyright © 2008 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl The clinical anatomy of the cephalic vein in the deltopectoral triangle M. Loukas1, 2, C.S. Myers1, Ch.T. Wartmann1, R.S. Tubbs3, T. Judge1, B. Curry1, R. Jordan1 1Department of Anatomical Sciences, St. George’s University, School of Medicine, Grenada, West Indies 2Department of Education and Development, Harvard Medical School, Boston MA, USA 3Department of Cell Biology and Pediatric Neurosurgery, University of Alabama at Brimingham, AL, USA [Received 19 June 2007; Revised 3 January 2008; Accepted 7 January 2008] Identification and recognition of the cephalic vein in the deltopectoral triangle is of critical importance when considering emergency catheterization proce- dures. The aim of our study was to conduct a cadaveric study to access data regarding the topography and the distribution patterns of the cephalic vein as it relates to the deltopectoral triangle. One hundred formalin fixed cadavers were examined. The cephalic vein was found in 95% (190 right and left) spec- imens, while in the remaining 5% (10) the cephalic vein was absent. In 80% (152) of cases the cephalic vein was found emerging superficially in the lateral portion of the deltopectoral triangle. In 30% (52) of these 152 cases the ceph- alic vein received one tributary within the deltopectoral triangle, while in 70% (100) of the specimens it received two. In the remaining 20% (38) of cases the cephalic vein was located deep to the deltopectoral fascia and fat and did not emerge through the deltopectoral triangle but was identified medially to the coracobrachialis and inferior to the medial border of the deltoid. -

Carpal Box and Open Cup Radiography
.............................................................................................................. ON THE JOB Carpal Box and Open Cup Radiography Dan L. Hobbs, M.S.R.S., Scaphoid fractures of the wrist are will include a discussion of the blood R.T.(R)(CT)(MR), is an asso- common and account for 71% of all car- supply to this bone. Next, there will be ciate professor in the depart- pal bone fractures. In the United States, a brief discussion of the mechanism of ment of radiographic science approximately 345 000 new scaphoid frac- injury, and the article will conclude with at Idaho State University in tures occur each year.1 Additionally, sta- a review of 3 positioning techniques that Pocatello. tistics have shown that scaphoid fractures can be employed to help diagnose scaph- account for 2% to 7% of all orthopedic oid fractures. Acknowledgement: Joshua fractures; they are the most commonly Howard , a student in the undiagnosed fracture.2 If an undiag- Anatomy radiographic science program nosed fracture is left without proper The scaphoid is located on the radial at Idaho State University, con- immobilization, a portion of the scaphoid side of the wrist in the anatomical snuff tributed valuable research to may die; therefore, it is imperative that box, which is located between the extensor this article. proper diagnosis, radiographic evalua- pollicis brevis and extensor pollicis longus tion and therapeutic treatment begin as tendons. (See Fig. 1.) It is the largest bone soon as possible. in the proximal row of carpals and can be The purpose of this article is to described as being complex because of its acquaint the radiographer with a few non- twisted shape; some describe it as being traditional methods used to image this boat-shaped.3 It articulates with the radius, fracture. -
Abdominal Wall Anterior 98-108 Posterior 109-11 Abductor Digiti
Index Cambridge University Press 978-0-521-72809-6 - Atlas of Musculoskeletal Ultrasound Anatomy: Second Edition Dr Mike Bradley and Dr Paul O’Donnell Index More information Index abdominal wall brachialis 42 echogenicity xi anterior 98–108 – – brachioradialis 49 elbow 49 64 posterior 109 11 anterior 53–8 calcaneo-fibular – abductor digiti minimi 70, 87 ligament 193 lateral 49 52 abductor pollicis brevis 87 medial 60 calf 178–86 posterior 62–4 abductor pollicis longus 79 antero-lateral compartment – extensor carpi radialis brevis acromioclavicular joint 26–7 179 80 lateral compartment 181–2 49, 79 adductor brevis 134 posterior compartment extensor carpi radialis longus – adductor canal 151 183 6 49, 79 adductor longus 134 capsule echogenicity xi extensor carpi ulnaris 79 – adductor magnus 134, 137 carpal tunnel 70 3 extensor digiti minimi 79 air echogenicity xi cartilage echogenicity extensor digitorum 79 costal cartilage xi – extensor digitorum longus 178 anatomical snuffbox 76 7 fibrocartilage xi anisotropy ix hyaline cartilage xi extensor hallucis longus 178, 205, 218–19 ankle 187–205 chest wall 13–21 anterior 202–5 anterior 13 extensor indicis 79 – lateral 193–6 costal cartilages 13 16 extensor pollicis brevis 79 medial 197–201 lateral 17 posterior 187–92 posterior 18–21 extensor pollicis longus 79 ribs 13–16 annular ligament 52 extensor retinaculum 202 collateral ligament anterior cruciate ligament fascia echogenicity xi lateral 167 (ACL) 153–7 fat echogenicity xi medial 165 antero-lateral pelvis 127–30 ulnar (UCL) 61 femoral neck -

Hand Surgery: a Guide for Medical Students
Hand Surgery: A Guide for Medical Students Trevor Carroll and Margaret Jain MD Table of Contents Trigger Finger 3 Carpal Tunnel Syndrome 13 Basal Joint Arthritis 23 Ganglion Cyst 36 Scaphoid Fracture 43 Cubital Tunnel Syndrome 54 Low Ulnar Nerve Injury 64 Trigger Finger (stenosing tenosynovitis) • Anatomy and Mechanism of Injury • Risk Factors • Symptoms • Physical Exam • Classification • Treatments Trigger Finger: Anatomy and MOI (Thompson and Netter, p191) • The flexor tendons run within the synovial tendinous sheath in the finger • During flexion, the tendons contract, running underneath the pulley system • Overtime, the flexor tendons and/or the A1 pulley can get inflamed during finger flexion. • Occassionally, the flexor tendons and/or the A1 pulley abnormally thicken. This decreases the normal space between these structures necessary for the tendon to smoothly glide • In more severe cases, patients can have their fingers momentarily or permanently locked in flexion usually at the PIP joint (Trigger Finger‐OrthoInfo ) Trigger Finger: Risk Factors • Age: 40‐60 • Female > Male • Repetitive tasks may be related – Computers, machinery • Gout • Rheumatoid arthritis • Diabetes (poor prognostic sign) • Carpal tunnel syndrome (often concurrently) Trigger Finger: Subjective • C/O focal distal palm pain • Pain can radiate proximally in the palm and distally in finger • C/O finger locking, clicking, sticking—often worse during sleep or in the early morning • Sometimes “snapping” during flexion • Can improve throughout the day Trigger Finger: -

Radial Medial Head Triceps Branch Transfer to Axillary Nerve by Axillary Approach Acesso Ao Nervo Axilar Por Via Axilar Anterior
THIEME 134 Review Article | Artigo de Revisão Radial Medial Head Triceps Branch Transfer to Axillary Nerve by Axillary Approach Acesso ao nervo axilar por via axilar anterior José Marcos Pondé 1 Lazaro Santos 2 João Pedro Magalhaes 2 Ana Flavia D ’Álmeida 2 1 Department of Neurosciences and Mental Health, Universidade Address for correspondence José Marcos Pondé, MD, PhD, Av. Paulo Federal da Bahia (UFBA), Salvador, Bahia, Brazil VI, 111, Pituba, Salvador, BA, Brazil 41810-000 2 Bahian School of Medicine and Public Health, Salvador, Bahia, Brazil (e-mail: [email protected]). Arq Bras Neurocir 2015;34:134 –138. - Abstract Objective To describe axillary approach for axillary nerve transfer with radial nerve branch in brachial plexus lesions. Methods Six patients aged 24 to 54 (mean 30) years with traumatic superior trunk brachial plexus injury underwent axillary approach between October 2011 and April 2012. On physical examination prior to surgery, they could not perform shoulder abduction, external rotation, or elbow flexion. Surgical approach was made through axillary pathway without any muscular section. The transfer was done with the radial branch to the medial head of triceps. In addition to transfer to axillary nerve, each Keywords patient had spinal accessory nerve transferred to suprascapular nerve and ulnar nerve ► axillary nerve fascicle transferred to musculocutaneous nerve. ► brachial plexus Conclusion Theaxillary approach allowseasyaccesstoaxillarynerveand, therefore, is ► transfer a feasible pathway to transferences involving this nerve. Resumo Objetivo Apresentar via axilar por transferência de nervo axilar com ramo de nervo radial em lesões do plexus braquial. Métodos Seis pacientes com idade entre 24 e 54 anos (média de 30) com lesão braquial traumática do plexus no tronco superior submetidos a via axilar entre outubro de 2011 e abril de 2012. -

Causes and Assessment of Subacute and Chronic Wrist Pain
Singapore Med J 2013; 54(10): 592-598 P ictorial E ssay doi:10.11622/smedj.2013205 CMEARTICLE Causes and assessment of subacute and chronic wrist pain Janice Chin-Yi Liao1, MBBS, MRCS, Alphonsus Khin Sze Chong1,2, MBBS, FAMS, David Meng Kiat Tan1 , MBBS, MMed ABSTRACT Wrist pain is a common presentation to the general practitioner and emergency department. Most cases are simple to treat, and pain frequently resolves with conservative treatment. However, there are certain conditions, such as scaphoid nonunion and Kienböck’s disease, where delayed diagnosis and treatment can result in long-term deformity or disability. This article covers the various causes of wrist pain, recommendations on how wrist pain should be assessed, as well as details some of the common conditions that warrant specialist referral. Keywords: chronic wrist pain, physical examination, wrist injuries, wrist pain INTRODUCTION in the scapholunate interval or ulnar fossa may indicate Wrist pain is a common clinical problem.(1) Many acute cases scapholunate ligament injuries or triangular fibrocartilage are sprains or contusions following a minor injury, or tendinitis complex (TFCC) injuries, respectively. The wrist should following an episode of overuse. These problems generally then be assessed through passive and active range of motion resolve within weeks with rest, temporary immobilisation and exercises. Special tests (e.g. Finkelstein’s and Watson’s tests) symptomatic pain relief. to differentiate specific wrist conditions are described in Wrist pain that does not resolve after six weeks to three later sections. Ideally, patients with persistent swelling and months is a frequent diagnostic challenge to primary care tenderness, or a recent or remote history of trauma, should physicians.