Anatomy Module 3. Muscles. Materials for Colloquium Preparation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

7-Khyati Santram
J. Anat. Sciences, 24(2): Dec. 2016, 33-35 Case Report ANATOMICAL VARIATION OF THE TRAPEZIUS MUSCLE- A CASE REPORT Khayati Sant Ram*, Anjali Aggarwal*,Tulika Gupta *,Amandeep kaur*,Jyoti Rajput*, Daisy Sahni* *Department of Anatomy, Post Graduate Institute of Medical Education and Research, Chandigarh, ABSTRACT During routine cadaveric dissection for undergraduate teaching variation in the course and insertion of fibers left trapezius muscle was noticed in two embalmed male cadavers. Some of the occipital fibers while descending towards clavicle got separated from rest of the muscle, inclined medially and inserted on the 1cm area of middle third of superior surface of clavicle. The remaining occipital fibers got inserted after a gap of on 1.5cm on the superior surface of lateral part of clavicle. Detached portion of trapezius muscles was tendinous in insertion. Two structures namely external jugular vein and supraclavicular nerves were seen passing through the gap in one cadaver (Case 1) whereas in other cadaver (Case 2) only external jugular vein was passing through the gap. Knowledge of this variation is clinically important in surgical exploration of posterior triangle.supraclavicular nerve entrapment syndrome and in various approaches involving external jugular vein. Key words: - trapezius muscle, cleidoccipital, supraclavicular nerves INTRODUCTION insertion of clavicular fibers left trapezius muscle of Trapezius muscle(TM) is a flat triangular muscle left side was noticed in two adult male cadavers. which extends over back of the neck and upper Case 1- In 78- years-old male cadaver trapezius thorax. On either side the muscle is attached to muscle of left side took usual origin from the medial medial third of superior nuchal line, external occipital portion of superior nuchal line, external occipital protuberance, ligamentum nuchae and apices of the protuberance, ligamentum nuchae and apices of the spinous processes and their supraspinous ligament spinous processes of thoracic vertebrae. -

Neck Dissection Using the Fascial Planes Technique
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY NECK DISSECTION USING THE FASCIAL PLANE TECHNIQUE Patrick J Bradley & Javier Gavilán The importance of identifying the presence larised in the English world in the mid-20th of metastatic neck disease with head and century by Etore Bocca, an Italian otola- neck cancer is recognised as a prominent ryngologist, and his colleagues 5. factor determining patients’ prognosis. The current available techniques to identify Fascial compartments allow the removal disease in the neck all have limitations in of cervical lymphatic tissue by separating terms of accuracy; thus, elective neck dis- and removing the fascial walls of these section is the usual choice for management “containers” along with their contents of the clinically N0 neck (cN0) when the from the underlying vascular, glandular, risk of harbouring occult regional metasta- neural, and muscular structures. sis is significant (≥20%) 1. Methods availa- ble to identify the N+ (cN+) neck include Anatomical basis imaging (CT, MRI, PET), ultrasound- guided fine needle aspiration cytology The basic understanding of fascial planes (USGFNAC), and sentinel node biopsy, in the neck is that there are two distinct and are used depending on resource fascial layers, the superficial cervical fas- availability, for the patient as well as the cia, and the deep cervical fascia (Figures local health service. In many countries, 1A-C). certainly in Africa and Asia, these facilities are not available or affordable. In such Superficial cervical fascia circumstances patients with head and neck cancer whose primary disease is being The superficial cervical fascia is a connec- treated surgically should also have the tive tissue layer lying just below the der- neck treated surgically. -

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -
Anatomical Snuffbox
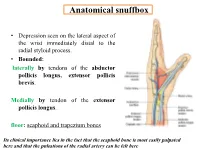
Anatomical snuffbox • Depression seen on the lateral aspect of the wrist immediately distal to the radial styloid process. • Bounded: laterally by tendons of the abductor pollicis longus, extensor pollicis brevis. Medially by tendon of the extensor pollicis longus. floor: scaphoid and trapezium bones Its clinical importance lies in the fact that the scaphoid bone is most easily palpated here and that the pulsations of the radial artery can be felt here Anatomical snuffbox Anatomical snuffbox • Contents: 2) Origin of the 1) The radial artery cephalic vein pass subcutaneously over the snuffbox. 3) Superficial branch of the radial nerve pass subcutaneously over the snuffbox. Blood supply of the hand Anastomoses occur between the radial and ulnar arteries via the superficial and deep palmar arches The Deep palmar arch is formed mainly by the radial artery while the superficial palmar arch is formed mainly by the ulnar artery 3-On entering the palm, it curves laterally behind (deep) the palmar 4-The arch is aponeurosis and in front completed on (superficial) of the long flexor the lateral side tendons forming by the the superficial palmar arch superficial branch of the radial artery. 2-Then it gives off its deep branch of which runs in front of the FR , and joins the radial artery to complete the deep palmar arch 1-Enters the hand anterior (superficial) to the Superficial flexor retinaculum palmar branch of radial artery through Guyon’s canal Radial artery 5-The superficial palmar arch gives off digital arteries from its convexity which pass to the fingers and supply them Superficial palmar arch Deep palmar branch of ulnar artery Superficial palmar branch of radial artery Ulnar artery Radial artery Radial Artery first dorsal interosseous muscle 1-From the floor of the anatomical snuff-box the radial artery leaves the dorsum of the hand by turning forward between the two heads of the first dorsal interosseous muscle. -

Level Diagnosis of Cervical Compressive Myelopathy: Signs, Symptoms, and Lesions Levels
Elmer Press Original Article J Neurol Res • 2013;3(5):135-141 Level Diagnosis of Cervical Compressive Myelopathy: Signs, Symptoms, and Lesions Levels Naoki Kasahata ficult to accurately localize the lesion before radiographic Abstract diagnosis. However, neurological level diagnosis of spinal cord is important for accurate lesion-specific level diagnosis, Background: To elucidate signs and symptoms corresponding to patients’ treatment, avoiding diagnostic error, differential di- each vertebral level for level-specific diagnoses. agnosis, and especially for accurate level diagnosis of other nonsurgical myelopathies. Moreover, level diagnosis should Methods: We studied 106 patients with cervical compressive my- be considered from multiple viewpoints. Therefore, we in- elopathy. Patients who showed a single compressive site on mag- tend to make level diagnosis of myelopathy more accurate. netic resonance imaging (MRI) were selected, and signs, symp- Previously, lesion-specific level diagnoses by determin- toms, and the levels of the MRI lesions were studied. ing a sensory disturbance area or location of numbness in Results: Five of 12 patients (41.7%) with C4-5 intervertebral level the hands had the highest accuracy [1, 2]. Previous stud- lesions showed decreased or absent biceps and brachioradialis re- ies reported that C3-4 intervertebral level lesions showed flexes, while 4 of these patients (33.3%) showed generalized hyper- increased or decreased biceps reflexes, deltoid weakness, reflexia. In comparison, 5 of 24 patients (20.8%) with C5-6 inter- and sensory disturbance of arms or forearms [1, 3, 4], while vertebral level lesions showed decreased or absent triceps reflexes; C4-5 intervertebral level lesions showed decreased biceps however, 9 of these patients (37.5%) showed decreased or absent reflexes, biceps weakness, and sensory disturbance of hands biceps and brachioradialis reflexes. -

Variant Origins of Arteries in the Carotid Triangle - a Case Report
Case Report 281 Variant Origins of Arteries in the Carotid Triangle - A Case Report B. V. Murlimanju, MD; Latha V. Prabhu, MS; Mangala M. Pai, MD; Dhanya Jayaprakash, MBBS; Vasudha V. Saralaya, MS The left superior laryngeal artery was observed arising from the external carotid artery instead of the superior thyroid artery in the cadaver of an approximately 70 year-old Asian man. In addition, on the same side, the superior thyroid artery arose from the common carotid artery 2 cm before the bifurcation instead of its usual origin from the external carotid artery. From the external carotid artery, the lingual and facial arteries arose from the com- mon linguofacial trunk. The nerves in the carotid triangle were normal in course. No varia- tions were observed on the right side carotid system. The multiple variations in this case have not been previously described. The embryogenesis of this combination of variations is not clear, but the anatomic consequences may have important clinical implications. As angiography has gained popularity in diagnostic approaches in recent years, it is essential to be aware of these variations so that they are not overlooked in differential diagnoses. (Chang Gung Med J 2012;35:281-4) Key words: artery, superior laryngeal, superior thyroid, common carotid, external carotid, vari- ant origin natomical variations in the carotid triangle in the STA from the left CCA is reported here. In the Athe neck are important, especially during surgi- literature, a few variations in origin have been cal and radiological intervention in the region. reported for both arteries,(1-3) but the combination of Normally, the superior laryngeal artery (SLA) is a variations reported in this case has not been previ- branch of the superior thyroid artery (STA). -

Morphology of Extensor Indicis Proprius Muscle in the North Indian Region: an Anatomy Section Anatomic Study with Ontogenic and Phylogenetic Perspective
DOI: 10.7860/IJARS/2019/41047:2477 Original Article Morphology of Extensor Indicis Proprius Muscle in the North Indian Region: An Anatomy Section Anatomic Study with Ontogenic and Phylogenetic Perspective MEENAKSHI KHULLAR1, SHERRY SHARMA2 ABSTRACT to the index finger were noted and appropriate photographs Introduction: Variants on muscles and tendons of the forearm were taken. or hand occur frequently in human beings. They are often Results: In two limbs, the EIP muscle was altogether absent. discovered during routine educational cadaveric dissections In all the remaining 58 limbs, the origin of EIP was from the and surgical procedures. posterior surface of the distal third of the ulnar shaft. Out of Aim: To observe any variation of Extensor Indicis Proprius (EIP) these 58 limbs, this muscle had a single tendon of insertion in 52 muscle and to document any accessory muscles or tendons limbs, whereas in the remaining six limbs it had two tendinous related to the index finger. slips with different insertions. Materials and Methods: The EIP muscle was dissected in 60 Conclusion: Knowledge of the various normal as well as upper limb specimens. After reflection of the skin and superficial anomalous tendons on the dorsal aspect of the hand is fascia from the back of the forearm and hand, the extensor necessary for evaluating an injured or diseased hand and also at retinaculum was divided longitudinally and the dorsum of the the time of tendon repair or transfer. Awareness of such variants hand was diligently dissected. The extensor tendons were becomes significant in surgeries in order to avoid damage to the delineated and followed to their insertions. -

Unusual Organization of the Ansa Cervicalis: a Case Report
CASE REPORT ISSN- 0102-9010 UNUSUAL ORGANIZATION OF THE ANSA CERVICALIS: A CASE REPORT Ranjana Verma1, Srijit Das2 and Rajesh Suri3 Department of Anatomy, Maulana Azad Medical College, New Delhi-110002, India. ABSTRACT The superior root of the ansa cervicalis is formed by C1 fibers carried by the hypoglossal nerve, whereas the inferior root is contributed by C2 and C3 nerves. We report a rare finding in a 40-year-old male cadaver in which the vagus nerve fused with the hypoglossal nerve immediately after its exit from the skull on the left side. The vagus nerve supplied branches to the sternohyoid, sternothyroid and superior belly of the omohyoid muscles and also contributed to the formation of the superior root of the ansa cervicalis. In this arrangement, paralysis of the infrahyoid muscles may result following lesion of the vagus nerve anywhere in the neck. The cervical location of the vagus nerve was anterior to the common carotid artery within the carotid sheath. This case report may be of clinical interest to surgeons who perform laryngeal reinnervation and neurologists who diagnose nerve disorders. Key words: Ansa cervicalis, hypoglossal nerve, vagus nerve, variations INTRODUCTION cadaver. The right side was normal. The neck region The ansa cervicalis is a nerve loop formed was dissected and the neural structures in the carotid by the union of superior and inferior roots. The and muscular triangle regions were exposed, with superior root is a branch of the hypoglossal nerve particular attention given to the organization of the containing C1 fibers, whereas the inferior root is ansa cervicalis. -

The Branching and Innervation Pattern of the Radial Nerve in the Forearm: Clarifying the Literature and Understanding Variations and Their Clinical Implications
diagnostics Article The Branching and Innervation Pattern of the Radial Nerve in the Forearm: Clarifying the Literature and Understanding Variations and Their Clinical Implications F. Kip Sawyer 1,2,* , Joshua J. Stefanik 3 and Rebecca S. Lufler 1 1 Department of Medical Education, Tufts University School of Medicine, Boston, MA 02111, USA; rebecca.lufl[email protected] 2 Department of Anesthesiology, Stanford University School of Medicine, Stanford, CA 94305, USA 3 Department of Physical Therapy, Movement and Rehabilitation Science, Bouve College of Health Sciences, Northeastern University, Boston, MA 02115, USA; [email protected] * Correspondence: [email protected] Received: 20 May 2020; Accepted: 29 May 2020; Published: 2 June 2020 Abstract: Background: This study attempted to clarify the innervation pattern of the muscles of the distal arm and posterior forearm through cadaveric dissection. Methods: Thirty-five cadavers were dissected to expose the radial nerve in the forearm. Each muscular branch of the nerve was identified and their length and distance along the nerve were recorded. These values were used to determine the typical branching and motor entry orders. Results: The typical branching order was brachialis, brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, supinator, extensor digitorum, extensor carpi ulnaris, abductor pollicis longus, extensor digiti minimi, extensor pollicis brevis, extensor pollicis longus and extensor indicis. Notably, the radial nerve often innervated brachialis (60%), and its superficial branch often innervated extensor carpi radialis brevis (25.7%). Conclusions: The radial nerve exhibits significant variability in the posterior forearm. However, there is enough consistency to identify an archetypal pattern and order of innervation. These findings may also need to be considered when planning surgical approaches to the distal arm, elbow and proximal forearm to prevent an undue loss of motor function. -

Distal Radial Approach Through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention
Korean Circ J. 2018 Dec;48(12):1131-1134 https://doi.org/10.4070/kcj.2018.0293 pISSN 1738-5520·eISSN 1738-5555 Editorial Distal Radial Approach through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention Jae-Hyung Roh, MD, PhD, and Jae-Hwan Lee , MD, PhD Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea ► See the article “Feasibility of Coronary Angiography and Percutaneous Coronary Intervention via Left Snuffbox Approach” in volume 48 on page 1120. Received: Aug 27, 2018 The anatomical snuffbox, also known as the radial fossa, is a triangular-shaped depression Accepted: Sep 17, 2018 on the radial, dorsal aspect of the hand at the level of the carpal bones. It is clearly observed Figure 1 1)2) Correspondence to when the thumb is extended ( ). The bottom of the snuffbox is supported by carpal Jae-Hwan Lee, MD, PhD bones composed of the scaphoid and trapezium. The medial and lateral borders are bounded Division of Cardiology, Department of Internal by tendons of the extensor pollicis longus and the extensor pollicis brevis, respectively. The Medicine, Chungnam National University proximal border is formed by the styloid process of the radius. Within this narrow triangular Hospital, Chungnam National University space, various structures are located, including the distal radial artery (RA), a branch of the School of Medicine, 282, Munhwa-ro, Jung-gu, radial nerve, and the cephalic vein. Daejeon 35015, Korea. E-mail: [email protected] The anatomy of the hand arteries is illustrated in Figure 2. -

Variation of the Infrahyoid Muscle: Duplicated Omohyoid and Appearance of the Levator Glandulae Thyroideae Muscles
DOI 10.3349/ymj.2010.51.6.984 Case Report pISSN: 0513-5796, eISSN: 1976-2437 Yonsei Med J 51(6):984-986, 2010 Variation of the Infrahyoid Muscle: Duplicated Omohyoid and Appearance of the Levator Glandulae Thyroideae Muscles Deog-Im Kim,1 Ho-Jeong Kim,2 Jae-Young Park,2 and Kyu-Seok Lee2 1Department of Anatomy, Catholic Institution for Applied Anatomy, College of Medicine, The Catholic University of Korea, Seoul; 2Department of Anatomy, Kwandong University College of Medicine, Gangneung, Korea. Received: November 21, 2008 The embryologic origin of the omohyoid muscle is different from that of the other Revised: March 23, 2009 neck muscles. A number of variations such as the absence of muscle, variable sites Accepted: March 27, 2009 of origin and insertion, and multiple bellies have been reported. However, varia- Corresponding author: Dr. Kyu-Seok Lee, tions in the inferior belly of the omohyoid muscle are rare. There have been no Department of Anatomy, Kwandong University reports of the combined occurrence of the omohyoid muscle variation with the College of Medicine, 522 Naegok-dong, appearance of the levator glandulase thyroideae muscle. Routine dissection of a 51- Gangneung 210-701, Korea. year-old female cadaver revealed a duplicated omohyoid muscle and the appea- Tel: 82-33-649-7473, Fax: 82-33-641-1074 rance of the levator glandulae thyroideae muscle. In this case, the two inferior E-mail: [email protected] bellies of the omohyoid muscle were found to originate inferiorly from the superior border of the scapula. One of the inferior bellies generally continued to the superior ∙The authors have no financial conflicts of belly with the tendinous intersection. -

An Anomalous Digastric Muscle in the Carotid Sheath: a Case Report with Its
Short Communication 2020 iMedPub Journals Journal of Stem Cell Biology and Transplantation http://journals.imedpub.com Vol. 4 ISS. 4 : sc 37 ISSN : 2575-7725 DOI : 10.21767/2575-7725.4.4.37 8th Edition of International Conference on Clinical and Medical Case Reports - An anomalous digastric muscle in the carotid sheath: a case report with its embryological perspective and clinical relevance Srinivasa Rao Sirasanagandla Sultan Qaboos University, Oman Abstract Key words: Although infrahyoid muscles show considerable variations in Anterior belly, Posterior belly, Variation, Stylohyoid muscle, My- their development, existence of an anomalous digastric muscle lohyoid muscle, Hyoid bone in the neck was seldom reported. During dissection of trian- Anatomy gles of the neck for medical undergraduate students, we came across an anomalous digastric muscle in the carotid sheath of There is a pair of digastric muscles in the neck, and each digas- left side of neck. It was observed in a middle-aged cadaver at tric muscle has the anterior belly and the posterior belly. The College of Medicine and Health Sciences, Sultan Qaboos Uni- anterior belly is attached to the digastric fossa on the base of versity, Muscat, Oman. Digastric muscle was located within the the mandible close to the midline and runs toward the hyoid carotid sheath between the common and internal carotid arter- bone. The posterior belly is attached to the notch of the mas- ies and internal jugular vein. It had two bellies; cranial belly and toid process of the temporal bone and also runs toward the caudal belly which were connected by an intermediate tendon.