Serum N-Glycomics Stratifies Bacteremic Patients Infected With
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glycomics Meets Genomics, Epigenomics and Other High Throughput Omics for System Biology Studies
COCHBI-1014; NO. OF PAGES 7 Available online at www.sciencedirect.com Glycomics meets genomics, epigenomics and other high throughput omics for system biology studies 1 1 2,3 Vlatka Zoldosˇ , Tomislav Horvat and Gordan Lauc Majority of eukaryotic proteins are glycosylated and their Both inherited (genetic) and acquired (environmental) glycan moieties have numerous important structural, functional factors that modulate glycosylation affect numerous mol- and regulatory roles. Because of structural complexity of ecular processes, including interactions with specific glycans and technological limitations glycomics, and receptors or half-life of numerous membrane proteins particularly glycoproteomics was not able to follow rapid [3]. Both quantitative and qualitative changes in the progress in genomics and proteomics over last 30 years. repertoire of glycan structures have been found in many However, the field of glycan has been progressing rapidly and complex diseases and cancer [4]. However, due to the first large-scale studies of the glycome have been completed structural complexity of glycans and technological limita- recently. These studies have revealed significant differences in tions the knowledge of functional importance of glycans glycome composition between individuals, which may is significantly lagging behind the knowledge of DNA and contribute to the human phenotypic variability. The current proteins. state-of-the-art in high-throughput glycomics and its integration with genomics, epigenomics and lipidomics is The development of high-throughput reviewed in this article. quantitative glycomic analysis Addresses Until only a few years ago glycan analysis was extremely 1 University of Zagreb, Faculty of Science, Zagreb, Croatia 2 laborious and complex, hampering large-scale studies of University of Zagreb, Faculty of Pharmacy and Biochemistry, Zagreb, Croatia the glycome. -

Insights of New Tools in Glycomics Research Denong Wang1 * and Srinubabu Gedela2,3
Journal of Proteomics & Bioinformatics - Open Access Editorial JPB/Vol.1/November 2008 Insights of New Tools In Glycomics Research Denong Wang1 * and Srinubabu Gedela2,3 1Stanford Tumor Glycome Laboratory, Stanford University School of Medicine, Beckman Center, Rm B006, 279 Campus Drive, Stanford, CA 94305-5120, USA 2Center for Biotechnology & International Center for Bioinformatics, Andhra University College of Engineering, Visakhapatnam-530003, India. 3Institute of Glycoproteomics & Systems Biology, Andhra Pradesh, India *Corresponding authors: Denong Wang, Stanford Tumor Glycome Laboratory, Stanford University School of Medicine, Beckman Center, Rm B006, 279 Campus Drive, Stanford, CA 94305-5120, USA, E-mail: [email protected] Srinubabu Gedela: [email protected] Received November 01, 2008; Accepted November 04, 2008; Published November 05, 2008 Citation: Denong W, Srinubabu G (2008) Insights of New tools in Glycomics Research. J Proteomics Bioinform 1: 374-378. doi:10.4172/jpb.1000046 Copyright: © 2008 Denong W, Srinubabu G. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Since the origin of Journal of Proteomics & Bioinformatics the equivalence of papers published from different –omics disciplines is steadfast. The present editorial describes the new tools in glycomics research. -omics era Completion of the genome sequencing projects not only on the outer surfaces of the majority of viral, bacterial, pro- provides insight into the complex origin, history and related- tozoan and fungal pathogens. Many sugar structures are ness of the species, but also helps in understanding molecu- pathogen-specific, which makes them important molecular lar pathology of genetic diseases. -

1 Metabolomic and Glycomic Findings in Posttraumatic Stress Disorder Marcela Konjevoda, Lucija Tudora, Dubravka Svob Straca
CORE Metadata, citation and similar papers at core.ac.uk Metabolomic and glycomic findings in posttraumatic stress disorder Marcela Konjevoda, Lucija Tudora, Dubravka Svob Straca, Gordana Nedic Erjaveca,b, Coral Barbasb, Neven Zarkovica, Matea Nikolac Perkovica, Suzana Uzunc,d, Oliver Kozumplikc,d, Gordan Lauce, Nela Pivaca,* aRudjer Boskovic Institute, Division of Molecular Medicine, Bijenicka cesta 54, 10000 Zagreb, Croatia bThe Centre of Metabolomics and Bioanalysis (CEMBIO), University San Pablo CEU, Urbanización Montepríncipe, 28660 Boadilla del Monte, Madrid, Spain cClinic for Psychiatry Vrapce, Bolnicka cesta 32, 10000 Zagreb, Croatia dUniversity Josip Juraj Strossmayer Osijek, School of Medicine, Trg Svetog Trojstva 3, 31000 Osijek, Croatia eGENOS, Glycoscience Research Laboratory, Borongajska cesta 83, 10000 Zagreb, Croatia *Correspondence to: Professor Nela Pivac, PhD, Senior Scientist Division of Molecular Medicine Rudjer Boskovic Institute Bijenicka cesta 54, 10 000 Zagreb, Croatia Phone: + 385 1 457 1207; Fax: + 385 1 456 1010 E-mail: [email protected] 1 Abstract Posttraumatic stress disorder (PTSD) is a stressor-related disorder that develops in a subset of individuals exposed to a traumatic experience. Factors associated with vulnerability to PTSD are still not fully understood. PTSD is frequently comorbid with various psychiatric and somatic disorders, moderate response to treatment and remission rates. The term “theranostics” combines diagnosis, prognosis, and therapy and offers targeted therapy based on specific analyses. -
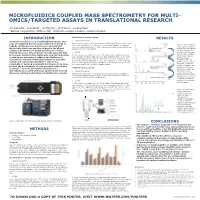
Microfluidics Coupled Mass Spectrometry for Multi- Omics/Targeted Assays in Translational Research
MICROFLUIDICS COUPLED MASS SPECTROMETRY FOR MULTI- OMICS/TARGETED ASSAYS IN TRANSLATIONAL RESEARCH PD Rainville1, G Astarita1, JP Murphy1, ID Wilson2, JI Langridge1 1Waters Corporation, Milford, MA; 2Imperial College, London, United Kingdom INTRODUCTION Lipidomics of human plasma RESULTS Translation medicine is an interdisciplinary science that Sample Preparation Human plasma samples were prepared by modified Bligh-Dyer extraction with aims at combining the information taken from bench to Figure 4. BPI of multiple- bedside. In this process molecules are isolated and chloroform : methanol (2:1) with a (4:1) with human plasma. The samples were then centrifuged at 13,000 RCF for 5 min, dried down, reconstituted and omics experiments from identified in discovery and then utilized in the clinical injected onto the LC-MS system. human urine and plasma setting as biomarkers of health and disease to better run consecutively. The develop therapies. It has become recently apparent that LC-MS profiling of biofluids was carried out in repetitive proteomics, metabolomics, lipidomics, and glycomics data A 1 µL injection was made onto the LC-MS system. The sample was eluted order of polar plasma under gradient conditions with aqueous formic acid/acetonitrile (40/60) and combined are necessary to address the challenge of profiling, plasma acetonitrile/isopropanol (10/90) at a flow rate of 3 µL/min. Separation was translational research which places strain on available lipidomics, and urine carried out on an iKey CSH C18 100 Å, 1.7µm, 150 µm x 100 mm controlled 1-4 profiling over a period of sample and instrument utilization . Due to the at 60 °C. -

Experimental Section
EXPERIMENTAL SECTION Detailed description of N-glycomics analysis. N-glycan release from plasma samples The N-glycan release of the discovery set was performed in microcentrifuge tubes, while the glycan release of the testing set was performed in 96-well plates. Both methods were shown to perform similarly (Supplementary Figure 3). The procedures are the same and similar to previously published methods (1, 2). Briefly, 25 μL of a 200mM ammonium bicarbonate (Sigma-Aldrich, St. Louis, MO) solution with 10 mM dithiothreitol (DTT, Promega, Madison, WI) was added to 25 μL of plasma. For the discovery set, this was performed in microcentrifuge tubes; for the testing set, this was performed in 96-well plates. Proteins in the samples were denatured using six cycles alternating between 100°C and room temperature (RT) for 10 seconds each. One µL of PNGaseF (New England Biolabs, Ipswich, MA, corresponding to 1000 NEB units or 15 IUB mU) was added to the samples, and enzymatic glycan release was performed for the discovery set in a CEM (Matthews, NC) microwave at 20W for 10 min. Enzymatic release was performed in batches of 23 samples and one standard serum, to allow quality control. For the testing set, glycan release was performed overnight (16h) at 37°C and a standard serum sample was included in the plate after every ten samples to allow quality control. Upon glycan release, deglycosylated proteins were precipitated using 200 µL of ice-cold ethanol, and the samples were chilled at -80°C for 1 hour. Upon centrifugation, the supernatant was transferred, and dried in vacuo. -

Semantics of Data for Life Sciences and Reproducible Research[Version 1
F1000Research 2020, 9:136 Last updated: 16 AUG 2021 OPINION ARTICLE BioHackathon 2015: Semantics of data for life sciences and reproducible research [version 1; peer review: 2 approved] Rutger A. Vos 1,2, Toshiaki Katayama 3, Hiroyuki Mishima4, Shin Kawano 3, Shuichi Kawashima3, Jin-Dong Kim3, Yuki Moriya3, Toshiaki Tokimatsu5, Atsuko Yamaguchi 3, Yasunori Yamamoto3, Hongyan Wu6, Peter Amstutz7, Erick Antezana 8, Nobuyuki P. Aoki9, Kazuharu Arakawa10, Jerven T. Bolleman 11, Evan Bolton12, Raoul J. P. Bonnal13, Hidemasa Bono 3, Kees Burger14, Hirokazu Chiba15, Kevin B. Cohen16,17, Eric W. Deutsch18, Jesualdo T. Fernández-Breis19, Gang Fu12, Takatomo Fujisawa20, Atsushi Fukushima 21, Alexander García22, Naohisa Goto23, Tudor Groza24,25, Colin Hercus26, Robert Hoehndorf27, Kotone Itaya10, Nick Juty28, Takeshi Kawashima20, Jee-Hyub Kim28, Akira R. Kinjo29, Masaaki Kotera30, Kouji Kozaki 31, Sadahiro Kumagai32, Tatsuya Kushida 33, Thomas Lütteke 34,35, Masaaki Matsubara 36, Joe Miyamoto37, Attayeb Mohsen 38, Hiroshi Mori39, Yuki Naito3, Takeru Nakazato3, Jeremy Nguyen-Xuan40, Kozo Nishida41, Naoki Nishida42, Hiroyo Nishide15, Soichi Ogishima43, Tazro Ohta3, Shujiro Okuda44, Benedict Paten45, Jean-Luc Perret46, Philip Prathipati38, Pjotr Prins47,48, Núria Queralt-Rosinach 49, Daisuke Shinmachi9, Shinya Suzuki 30, Tsuyosi Tabata50, Terue Takatsuki51, Kieron Taylor 28, Mark Thompson52, Ikuo Uchiyama 15, Bruno Vieira53, Chih-Hsuan Wei12, Mark Wilkinson 54, Issaku Yamada 36, Ryota Yamanaka55, Kazutoshi Yoshitake56, Akiyasu C. Yoshizawa50, Michel -

Glycomics Hits the Big Time
Leading Edge Essay Glycomics Hits the Big Time Gerald W. Hart1,* and Ronald J. Copeland1 1Department of Biological Chemistry, School of Medicine, Johns Hopkins University, 725 North Wolfe Street, Baltimore, MD 21205-2185, USA *Correspondence: [email protected] DOI 10.1016/j.cell.2010.11.008 Cells run on carbohydrates. Glycans, sequences of carbohydrates conjugated to proteins and lipids, are arguably the most abundant and structurally diverse class of molecules in nature. Recent advances in glycomics reveal the scope and scale of their functional roles and their impact on human disease. By analogy to the genome, transcriptome, O-GlcNAc (Hart et al., 2007). Even though Dynamic Structural Complexity or proteome, the ‘‘glycome’’ is the the generic term ‘‘glycosylation’’ is often Underlies Glycan Functions complete set of glycans and glycoconju- used to categorize and lump all glycan Glycoconjugates provide dynamic struc- gates that are made by a cell or organism modifications of proteins into one bin, tural diversity to proteins and lipids that under specific conditions. Therefore, side by side with other posttranslational is responsive to cellular phenotype, to ‘‘glycomics’’ refers to studies that attempt modifications such as phosphorylation, metabolic state, and to the developmental to define or quantify the glycome of a cell, acetylation, ubiquitination, or methylation, stage of cells. Complex glycans play crit- tissue, or organism (Bertozzi and Sasise- such a view is not only inaccurate, but ical roles in intercellular and intracellular kharan, 2009). In eukaryotes, protein also is completely misleading. If one only processes, which are fundamentally glycosylation generally involves the cova- considers the linkage of the first glycan important to the development of multicel- lent attachment of glycans to serine, to the polypeptide in both prokaryotic lularity (Figure 1). -

Researchers Apply Systems Biology and Glycomics to Study Human Inflammatory Diseases 28 October 2008
Researchers apply systems biology and glycomics to study human inflammatory diseases 28 October 2008 An innovative systems biology approach to complex biological functions and interactions understanding the carbohydrate structures in cells instead of studying individual units, such as a single is leading to new ways to understand how gene or protein, in isolation. inflammatory illnesses and cardiovascular disease develop in humans. The work was described in two "Systems biology is well-suited to this research recent publications by University at Buffalo because it helps us develop the mathematical chemical engineers. concepts to enable us to influence and enhance our understanding of how the glycome functions," said Supported by research grants from the National Neelamegham. "This then produces clues on how Institutes of Health, the ultimate goal of the project we might manipulate the adhesivity of white blood is to define novel strategies to perturb the glycome cells to the blood vessel wall." -- the complete set of an organism's carbohydrate structures in cells -- in ways that lead to the Glycans are carbohydrate molecules that mediate identification of new targets and molecular the microscopic interactions between white blood therapies to combat a broad range of inflammatory cells and blood vessel walls. These interactions diseases. play a major role in painful and debilitating inflammatory medical conditions such as asthma, The binding of white blood cells to blood vessels is psoriasis, Crohn's disease, reperfusion injury and a key step in the progression of inflammatory other cardiovascular ailments. diseases, explained Sriram Neelamegham, Ph.D., UB professor of chemical and biological In a recent paper in The FASEB Journal, the UB engineering in the School of Engineering and researchers describe one of the first studies to take Applied Sciences, and co-author of both papers. -

Regulation of Sialylated N-Glycans/ Integrin and Breast Cancer Brain Metastasis Wenjing Peng, Rui Zhu, Shiyue Zhou, Parvin Mirzaei & Yehia Mechref*
www.nature.com/scientificreports OPEN Integrated Transcriptomics, Proteomics, and Glycomics Reveals the Association between Up- regulation of Sialylated N-glycans/ Integrin and Breast Cancer Brain Metastasis Wenjing Peng, Rui zhu, Shiyue Zhou, Parvin Mirzaei & Yehia Mechref* Breast cancer brain metastasis has been recognized as one of the central issues in breast cancer research. The elucidation of the processes and pathways that mediate this step will provide important clues for a better understanding of breast cancer metastasis. Increasing evidence suggests that aberrant glycosylation patterns greatly contribute to cell invasion and cancer metastasis. Herein, we combined next-generation RNA sequencing with liquid chromatography-tandem mass spectrometry-based proteomic and N-glycomic analysis from fve breast cancer cell lines and one brain cancer cell line to investigate the possible mechanisms of breast cancer brain metastasis. The genes/proteins associated with cell movement were highlighted in breast cancer brain metastasis. The integrin signaling pathway and the up-regulation of α-integrin (ITGA2, ITGA3) were associated with the brain metastatic process. 12 glycogenes showed unique expression in 231BR, which could result in an increase of sialylation during brain metastasis. In agreement with the changes of glycogenes, 60 out of 63 N-glycans that were identifed exhibited diferential expression among cell lines. The correlation between glycogenes and glycans revealed the importance of sialylation and sialylated glycans in breast cancer brain metastasis. Highly sialylated N-glycans, which were up-regulated in brain-seeking cell line 231BR, likely play a role in brain metastasis. Breast cancer, the leading cause of cancer mortality and morbidity among females, represents the second highest frequency of brain metastasis1,2. -

Integrated Omics: Tools, Advances and Future Approaches
62 1 Journal of Molecular B B Misra et al. Approaches and tools in 62:1 R21–R45 Endocrinology integrated omics REVIEW Integrated omics: tools, advances and future approaches Biswapriya B Misra1, Carl Langefeld1,2, Michael Olivier1 and Laura A Cox1,3 1Center for Precision Medicine, Section on Molecular Medicine, Department of Internal Medicine, Wake Forest School of Medicine, Winston-Salem, North California, USA 2Department of Biostatistics, Wake Forest School of Medicine, Winston-Salem, North California, USA 3Southwest National Primate Research Center, Texas Biomedical Research Institute, San Antonio, Texas, USA Correspondence should be addressed to L A Cox: [email protected] Abstract With the rapid adoption of high-throughput omic approaches to analyze biological Key Words samples such as genomics, transcriptomics, proteomics and metabolomics, each f integrated analysis can generate tera- to peta-byte sized data files on a daily basis. These data file f omics sizes, together with differences in nomenclature among these data types, make the f genomics integration of these multi-dimensional omics data into biologically meaningful context f transcriptomics challenging. Variously named as integrated omics, multi-omics, poly-omics, trans-omics, f proteomics pan-omics or shortened to just ‘omics’, the challenges include differences in data f metabolomics cleaning, normalization, biomolecule identification, data dimensionality reduction, f network biological contextualization, statistical validation, data storage and handling, sharing and f statistics data archiving. The ultimate goal is toward the holistic realization of a ‘systems biology’ f Bayesian understanding of the biological question. Commonly used approaches are currently f machine learning limited by the 3 i’s – integration, interpretation and insights. -

1 an Introduction to Bioinformatics for Glycomics Research Kiyoko F. Aoki-Kinoshita, Ph.D. Dept. of Bioinformatics Faculty of En
An introduction to bioinformatics for glycomics research Kiyoko F. Aoki-Kinoshita, Ph.D. Dept. of Bioinformatics Faculty of Engineering, Soka University [email protected] Abstract: Carbohydrates are the third class of information-encoding biological macromolecules. The term ‘glycomics,’ the scientific attempt of characterizing and studying carbohydrates, is a rapidly emerging branch of science, for which informatics is just beginning. Glycomics requires sophisticated algorithmic approaches. The status of structural encoding, standardization, databases and applications will be presented. Goals • To introduce the role of carbohydrates as the third class of information-containing biological macromolecules to a broader audience of computational biologists. • To explain the fundamental characteristics of carbohydrate structures, which require specific encoding schemata as well as algorithmic developments. • To give an overview of available database resources, algorithms and techniques. • To outline a systems approach to discover the structure-function relationships of glycans. Schedule: • General Introduction: (60 minutes plus 15 minutes for discussion) • Biological role of carbohydrates as information containing molecules (15 minutes) • The role of informatics in glycomics research (15 minutes) • The challenges to connect glyco-related databases (30 minutes) • Glycome Informatics: (120 minutes plus 15 minutes for discussion) • Computer theoretic algorithms for tree structures (30 minutes) • Automated MS prediction algorithms (20 minutes) -

Introducing Glycomics Data Into the Semantic
Aoki-Kinoshita et al. Journal of Biomedical Semantics 2013, 4:39 http://www.jbiomedsem.com/content/4/1/39 JOURNAL OF BIOMEDICAL SEMANTICS SHORT REPORT Open Access Introducing glycomics data into the Semantic Web Kiyoko F Aoki-Kinoshita1, Jerven Bolleman2, Matthew P Campbell3, Shin Kawano4, Jin-Dong Kim4, Thomas Lütteke5, Masaaki Matsubara6, Shujiro Okuda7,8, Rene Ranzinger9, Hiromichi Sawaki10, Toshihide Shikanai10, Daisuke Shinmachi10, Yoshinori Suzuki10, Philip Toukach11, Issaku Yamada6, Nicolle H Packer3 and Hisashi Narimatsu10* Abstract Background: Glycoscience is a research field focusing on complex carbohydrates (otherwise known as glycans)a, which can, for example, serve as “switches” that toggle between different functions of a glycoprotein or glycolipid. Due to the advancement of glycomics technologies that are used to characterize glycan structures, many glycomics databases are now publicly available and provide useful information for glycoscience research. However, these databases have almost no link to other life science databases. Results: In order to implement support for the Semantic Web most efficiently for glycomics research, the developers of major glycomics databases agreed on a minimal standard for representing glycan structure and annotation information using RDF (Resource Description Framework). Moreover, all of the participants implemented this standard prototype and generated preliminary RDF versions of their data. To test the utility of the converted data, all of the data sets were uploaded into a Virtuoso triple store, and several SPARQL queries were tested as “proofs-of-concept” to illustrate the utility of the Semantic Web in querying across databases which were originally difficult to implement. Conclusions: We were able to successfully retrieve information by linking UniCarbKB, GlycomeDB and JCGGDB in a single SPARQL query to obtain our target information.