The 21St Century Panglong Conference Kun Tang1* and Yingxi Zhao2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
U.S. Relations with Burma: Key Issues in 2019
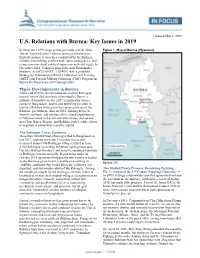
Updated May 8, 2019 U.S. Relations with Burma: Key Issues in 2019 In 2018, the 115th Congress was generally critical of the Figure 1. Map of Burma (Myanmar) Trump Administration’s Burma policy, particularly its limited response to atrocities committed by the Burmese military, intensifying conflict with ethnic insurgencies, and rising concerns about political repression and civil rights. In December 2018, Congress passed the Asia Reassurance Initiative Act of 2018 (P.L. 115-409), which prohibits funding for International Military Education and Training (IMET) and Foreign Military Financing (FMF) Program in Burma for fiscal years 2019 through 2023. Major Developments in Burma At the end of 2018, an estimated one million Rohingya, most of whom fled atrocities committed by Burma’s military (Tatmadaw) in late 2017, remained in refugee camps in Bangladesh, unable and unwilling to return to Burma’s Rakhine State given the current policies of the Burmese government. Also in 2018, fighting between Burma’s military and various ethnic armed organizations (EAOs) escalated in Kachin and Shan States, and spread into Chin, Karen (Kayin), and Rakhine States, while efforts to negotiate a nationwide ceasefire stalled. The Rohingya Crises Continue More than 700,000 Sunni Rohingya fled to Bangladesh in late 2017, seeking to escape Tatmadaw forces that destroyed almost 400 Rohingya villages, killed at least 6,700 Rohingya (according to human rights groups and Doctors Without Borders), and sexually assaulted hundreds of Rohingya women and girls. Repatriation under an October 2018 agreement between the two nations is stalled as the Burmese government is unable or unwilling to Source: CRS establish conditions that would allow the voluntary, safe, dignified, and sustainable return of the Rohingya. -

The Situation in Karen State After the Elections PAPER No
EBO ANALYSIS The Situation in Karen State after the Elections PAPER No. 1 2011 THE SITUATION IN KAREN STATE AFTER THE ELECTIONS EBO Analysis Paper No. 1/2011 For over sixty years the Karens have been fighting the longest civil war in recent history. The struggle, which has seen demands for an autonomous state changed to equal recognition within a federal union, has been bloody and characterized by a number of splits within the movement. While all splinter groups ostensibly split to further ethnic Karen aspirations; recent decisions by some to join the Burmese government’s Border Guard Force (BGF) is seen as an end to such aspirations. Although a number of Karen political parties were formed to contest the November elections, the likelihood of such parties seriously securing appropriate ethnic representation without regime capitulation is doubtful. While some have argued, perhaps correctly, that the only legitimate option was to contest the elections, the closeness of some Karen representatives to the current regime can only prolong the status quo. This papers examines the problems currently affecting Karen State after the 7 November elections. THE BORDER GUARD FORCE Despite original promises of being allowed to recruit a total of 9,000 troops, the actual number of the DKBA (Democratic Karen Buddhist Army) or Karen Border Guard Force has been reduced considerably. In fact, a number of the original offers made to the DKBA have been revoked. At a 7 May 2010 meeting held at Myaing Gyi Ngu, DKBA Chairman U Tha Htoo Kyaw stated that ‘According to the SE Commander, the BGF will retain the DKBA badge.’ In fact the DKBA were given uniforms with SPDC military patches and all Karen flags in DKBA areas were removed and replaced by the national flag. -

Women and the 21 Century Panglong Conference
Women and the 21st Century Panglong Conference Dispatch by Hanney Lwin Oo, Yangon Office Today, 31st August 2016, the historic Panglong Conference started in Myanmar, aimed at reaching comprehensive peace in the conflict-torn country. The participants of the Conference include the government, political parties, ethnic armed groups, ethnic representatives, the Myanmar military, and some civil society actors. Participating Women’s Organizations include Women and Peace Action Network, Shan State Gender Equality Network, Women's League of Burma (WLB), Nyein Foundation Women's Organizations Network (Myanmar), Gender and Development Institute-Myanmar, and Alliance on Gender Inclusion in the Peace Process (AGIPP). UN Secretary General, Ban Ki-moon will deliver a speech at today’s 21st-century Panglong Conference, which he called a “promising first step” of the new administration’s attempt to solve Myanmar’s decades- long armed conflicts. Visiting the country for the fifth time, the UN chief said yesterday that the peace process will need further strengthening. But he congratulated the participants’ “patience, determination and spirit of compromise”. “The steps you have taken toward peace and national reconciliation will need to be further strengthened, broadened and consolidated. This is the real expectation of the international community,” he said. He added that the United Nations will continue to support the peace process, as it has done since the reign of the oppressive military regime. Mr Ban said the United Nations has consistently backed Myanmar’s journey toward democracy and human rights. “It has been a great honour to work with Daw Aung San Suu Kyi in particular,” he said, while standing alongside the state counsellor. -

Burma's Northern Shan State and Prospects for Peace
UNITED STATES INSTITUTE OF PEACE PEACEBRIEF234 United States Institute of Peace • www.usip.org • Tel. 202.457.1700 • @usip September 2017 DAVID SCOTT MATHIESON Burma’s Northern Shan State Email: [email protected] and Prospects for Peace Summary • Increased armed conflict between the Burmese Army and several ethnic armed organizations in northern Shan State threaten the nationwide peace process. • Thousands of civilians have been displaced, human rights violations have been perpetrated by all parties, and humanitarian assistance is being increasingly blocked by Burmese security forces. • Illicit economic activity—including extensive opium and heroin production as well as transport of amphetamine stimulants to China and to other parts of Burma—has helped fuel the conflict. • The role of China as interlocutor between the government, the military, and armed actors in the north has increased markedly in recent months. • Reconciliation will require diverse advocacy approaches on the part of international actors toward the civilian government, the Tatmadaw, ethnic armed groups, and civil society. To facili- tate a genuinely inclusive peace process, all parties need to be encouraged to expand dialogue and approach talks without precondition. Even as Burma has “transitioned from decades Introduction of civil war and military rule Even as Burma has transitioned—beginning in late 2010—from decades of civil war and military to greater democracy, long- rule to greater democracy, long-standing and widespread armed conflict has resumed between several ethnic armed organizations (EAOs) and the Burmese armed forces (Tatmadaw). Early in standing and widespread 2011, a 1994 ceasefire agreement broke down as relations deterioriated in the wake of the National armed conflict has resumed.” League for Democracy government’s refusal to permit Kachin political parties to participate in the elections that ended the era of military rule in the country. -

STATUS of HUMAN RIGHTS & SANCTIONS in MYANMAR JULY 2020 REPORT Summary. This Report Reviews the July 2020 Developments Rela
STATUS OF HUMAN RIGHTS & SANCTIONS IN MYANMAR JULY 2020 REPORT Summary. This report reviews the July 2020 developments relating to human rights in Myanmar. Relatedly, it addresses the interchange between Myanmar’s reform efforts and the responses of the international community. I. Political Developments......................................................................................................2 A. Rohingya Refugee Crisis................................................................................................2 B. Corruption.......................................................................................................................2 C. International Community / Sanctions...........................................................................3 II. Civil and Political Rights...................................................................................................3 A. Freedom of Speech, Assembly and Association............................................................3 B. Freedom of the Press and Censorship...........................................................................4 III. Economic Development.....................................................................................................4 A. Economic Development—Legal Framework, Foreign Investment............................4 B. Economic Development—Infrastructure, Major Projects..........................................5 C. Land Seizure....................................................................................................................5 -

Panglong Or the Three Kings? by Harn Yawnghwe
No.2/2016 EBO Briefing Paper August 2016 Panglong or the Three Kings? By Harn Yawnghwe Why is it important that the 21st Century Panglong Conference acknowledges the fact that the Republic of the Union of Myanmar was founded by the peoples of the Chin and Kachin Hills; the Federated Shan States; the independent Karenni States; and British Burma? This is because in the prevailing general public view, the Union of Myanmar is a continuation of the three Burman Empires founded by King Anawratha, Bayinnaung, and Alaungpaya. In this version of history, the Burman empire founded by these warrior kings was disrupted by the advent of British colonial power. It is claimed that the British divided up the nation into various components in order to divide and rule. So General Aung San re-united all the components of this great nation at Panglong. Giant statues of King Anawratha, Bayinnaung and Alaungpaya in Naypyitaw This viewpoint was actively propagated by the Tatmadaw under successive dictatorships. In some circles, the period after independence in 1948 is known as the 4th Burman Empire. Even the preamble of the 2008 Constitution advocates this view by stating that, We, the National people have been living in unity and oneness, setting up an independent sovereign State and standing tall with pride. Due to colonial intrusion, the Nation lost her sovereign power in 1885. This actually applies only to the majority Burman kingdom. The Mon Hanthawaddy kingdom lost its sovereignty to the Burman in 1757 and the Rakhine Mrauk-U kingdom in 1785. The Chin, Kachin, Karenni and the Shan were never totally subjugated but engaged in fluctuating relationships with successive Burman kingdoms. -

A Return to War: Militarized Conflicts in Northern Shan State
A Return to War: Militarized Conflicts in Northern Shan State ASIA PAPER July 2018 EUROPEAN UNION A Return to War: Militarized Conflicts in Northern Shan State © Institute for Security and Development Policy V. Finnbodavägen 2, Stockholm-Nacka, Sweden www.isdp.eu “A Return to War: Militarized Conflicts in Northern Shan State” is an Asia Paper published by the published by the Institute for Security and Development Policy. The Asia Paper Series is the Occasional Paper series of the Institute’s Asia Program, and addresses topical and timely subjects. The Institute is based in Stockholm, Sweden, and cooperates closely with research centers worldwide. The Institute serves a large and diverse community of analysts, scholars, policy-watchers, business leaders, and journalists. It is at the forefront of research on issues of conflict, security, and development. Through its applied research, publications, research cooperation, public lectures, and seminars, it functions as a focal point for academic, policy, and public discussion. This publication has been produced with funding by the European Union. The content of this publication does not reflect the official opinion of the European Union. Responsibility for the information and views expressed in the paper lies entirely with the authors. No third-party textual or artistic material is included in the publication without the copyright holder’s prior consent to further dissemination by other third parties. Reproduction is authorised provided the source is acknowledged. © European Union and ISDP, 2018 Printed in Lithuania ISBN: 978-91-88551-11-5 Cover photo: Patrick Brown patrickbrownphoto.com Distributed in Europe by: Institute for Security and Development Policy Västra Finnbodavägen 2, 131 30 Stockholm-Nacka, Sweden Tel. -

Karen Peace Support Network's Burma's Dead
Burma’s Dead-End Peace Negotiation Process: A Case Study of the Land Sector A new political dialogue framework must be established that can go beyond the 2008 Constitution, and only then can a genuine and inclusive nationwide political dialogue take place. ABOUT KPSN aren Peace Support Network (KPSN) is the largest network of Karen civil society Korganizations in Burma/Myanmar. KPSN member organizations have facilitated humanitarian support for vulnerable conflict-affected Karen communities, internally facilitatedisplaced persons advocacy (IDPs), for and a refugeessustainable for decades. and equitable KPSN works peace to empower in Karen local areasKaren ofcommunities, Burma. raise awareness of the peace process, document human rights issues, and For [email protected] information, please contact: Karen Peace Support Network July, 2018 Karen Peace Support Network Burma’s Dead-End Peace Negotiation Process: July 2018 Front page cartoon LaiLone Burma’s Dead-End Peace Negotiation Process: 1 A Case Study of the Land Sector Acronym AA - Arakan Army CSOs - Civil Society Organizations FPD - Framework for Political Dialogue IDPs - Internally Displaced Peoples JICM - Joint Implementation Coordination Meeting KPSN - Karen Peace Support Network JMC - Joint Ceasefire Monitoring Committee KNU - Karen National Union KNLA - Karen National Liberation Army KIO - Kachin Independence Organziation KIA - Kachin Independence Army LDU - Lahu Democratic Union MNDAA - Myanmar National Democratic Alliance Army NMSP - New Mon State Party NLD - National League of Democracy ND - National Dialogue NCA - Nationwide Ceasefire Agreement PPST - Peace Process Steering Team RCSS - Restoration Council of Shan State TNLA - Ta-an National Liberation Army TWC - Thematic Working Committee 21CPC - Union Peace Conference (21Century Panglong Conference) UPDJC - Union Peace Dialogue Joint Committee 2 Burma’s Dead-End Peace Negotiation Process: A Case Study of the Land Sector CONTENTS I. -
Negotiating Burmese Independence Lauriane Simony
The London Conference and Beyond: Negotiating Burmese Independence Lauriane Simony To cite this version: Lauriane Simony. The London Conference and Beyond: Negotiating Burmese Independence. Human- ities and Social Sciences. 2013. dumas-02184580 HAL Id: dumas-02184580 https://dumas.ccsd.cnrs.fr/dumas-02184580 Submitted on 16 Jul 2019 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. THE LONDON CONFERENCE AND BEYOND: NEGOTIATING BURMESE INDEPENDENCE Lauriane Simony M1 Etudes Anglophones – ENS de Lyon May 2013 Under the supervision of Mélanie Torrent TABLE OF CONTENTS INTRODUCTION 4 I. ACCELERATING THE PROCESS: “INDEPENDENCE WITHIN A YEAR” 14 1. PRELIMINARY DEMANDS: ESTABLISHING A POSITION OF STRENGTH 14 A. THE AFPFL’S STATEMENT ON THE 23RD OF DECEMBER 1946 14 B. PRESSURE AND THREATS 16 2. A NECESSARY REDEFINITION OF THE WHITE PAPER PROGRAMME 18 A. THE WHITE PAPER PROGRAMME 18 B. INTERIM GOVERNMENT 19 C. THE DATE OF INDEPENDENCE 20 3. THE INFLUENCE OF INDIA’S STRUGGLE FOR INDEPENDENCE 22 A. BURMA AND INDIA’S SHARED HISTORY 22 B. KEEPING PACE WITH INDIA 23 II. INDEPENDENCE, STATE AND NATION: DEBATING BURMESE IDENTITY 27 1. THE BIRTH OF A NEW STATE: STRUGGLING FOR SELF-DETERMINATION 27 A. -
Militias in Myanmar
Militias in Myanmar John Buchanan July 2016 Acknowledgement The author would like to acknowledge the many people who assisted in this project, particularly those who generously shared their thoughts and experiences about the many topics covered in this report. I would also like to thank my friends and colleagues who took the time to provide comments and feedback on earlier drafts of this report. These include Matthew Arnold, Patrick Barron, Kim Jolliffe, Paul Keenan, David Mathieson, Brian McCartan, Kim Ninh, Andrew Selth and Martin Smith. Finally, I would also like to express my appreciation to friends from Burma who assisted with translation and data collection. About the Author John Buchanan is a Ph.D. Candidate in the Department of Political Science at the University of Washington. His interest in Southeast Asia dates back over two decades. His most recent publication is Developing Disparity: Regional Investment in Burma’s Borderlands for the Transnational Institute. About The Asia Foundation The Asia Foundation is a nonprofit international development organization committed to improving lives across a dynamic and developing Asia. Informed by six decades of experience and deep local expertise, our programs address critical issues affecting Asia in the 21st century—governance and law, economic development, women's empowerment, environment, and regional cooperation. In addition, our Books for Asia and professional exchanges are among the ways we encourage Asia’s continued development as a peaceful, just, and thriving region of the world. Headquartered in San Francisco, The Asia Foundation works through a network of offices in 18 Asian countries and in Washington, DC. Working with public and private partners, the Foundation receives funding from a diverse group of bilateral and multilateral development agencies, foundations, corporations, and individuals. -
The United Wa State Army and Burma's Peace Process
The United Wa State Army and Burma’s Peace Process By Bertil Lintner NO. 147 | APRIL 2019 Making Peace Possible NO. 147 | APRIL 2019 ABOUT THE REPORT Supported by USIP’s Asia Center to provide policymakers and the general public with a better understanding of Burma’s ethnic conflicts, this report examines the role of PEACE PROCESSES both the United Wa State Army and China in Burma’s peace process and suggests ways forward to break the present stalemate. ABOUT THE AUTHOR Bertil Lintner has covered Burma’s civil war and related issues such as narcotics trafficking for more than thirty-five years. Burma correspondent for the Far Eastern Economic Review from 1982 to 2004, he now writes for Asia Times and is the author of several books about Burma’s civil war and ethnic strife. Cover photo: United Wa State Army soldiers march during a media display in Panghsang, in the Wa Self-Administered Division of Shan State, Burma. (Photo by Soe Zeya Tun/Reuters) The views expressed in this report are those of the author alone. They do not necessarily reflect the views of the United States Institute of Peace. An online edition of this and related reports can be found on our website (www.usip.org), together with additional information on the subject. © 2019 by the United States Institute of Peace United States Institute of Peace 2301 Constitution Avenue NW Washington, DC 20037 Phone: 202.457.1700 Fax: 202.429.6063 E-mail: [email protected] Web: www.usip.org Peaceworks No. 147. First published 2019. ISBN: 978-1-60127-765-7 Making Peace Possible Contents 3 Introduction 4 Who Are the Wa? 6 Communism 10 Drug Trafficking 13 The UWSP, UWSA, and Their Allies 16 The UWSP and China’s Role in the Peace Process 22 Conclusion and Policy Recommendations USIP.ORG 1 Summary The United Wa State Army (UWSA), with its twenty-odd thousand men in arms, is the largest of Burma’s ethnic armed organizations (EAOs). -
Burma (Myanmar)
report Burma (Myanmar): The Time for Change By Martin Smith Acknowledgements Minority Rights Group International Minority Rights Group International (MRG) gratefully acknowl- Minority Rights Group International (MRG) is a non-govern- edges the support of all organizations and individuals who mental organization (NGO) working to secure the rights of gave financial and other assistance for this report ethnic, religious and linguistic minorities and indigenous peo- ples worldwide, and to promote cooperation and The Author understanding between communities. Our activities are Martin Smith is a writer and journalist specializing in Burmese focused on international advocacy, training, publishing and and ethnic minority affairs. He is author of Burma: Insurgency outreach. We are guided by the needs expressed by our and the Politics of Ethnicity, and he has reported for a variety worldwide partner network of organizations which represent of media, including the Guardian and the BBC. His television minority and indigenous peoples. work includes the documentaries, Dying for Democracy (UK Channel Four) and Forty Million Hostages (BBC). He has also MRG works with over 130 organizations in nearly 60 coun- written papers and reports for a number of academic institu- tries. Our governing Council, which meets twice a year, has tions and non-governmental organizations, including Article members from 10 different countries. MRG has consultative 19, World University Service, Tokyo University of Foreign Stud- status with the United Nations Economic and Social Council ies and Anti-Slavery International. Other publications include (ECOSOC), and is registered as a charity and a company Ethnic Groups in Burma: Development, Democracy and limited by guarantee under English law.