Cervical Sono-Anatomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Unusual Morphology of the Superior Belly of Omohyoid Muscle
Case Report http://dx.doi.org/10.5115/acb.2014.47.4.271 pISSN 2093-3665 eISSN 2093-3673 Unusual morphology of the superior belly of omohyoid muscle Rajesh Thangarajan, Prakashchandra Shetty, Srinivasa Rao Sirasanagnadla, Melanie Rose D’souza Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Manipal, Karnataka, India Abstract: Though anomalies of the superior belly of the omohyoid have been described in medical literature, absence of superior belly of omohyoid is rarely reported. Herein, we report a rare case of unilateral absence of muscular part of superior belly of omohyoid. During laboratory dissections for medical undergraduate students, unusual morphology of the superior belly of the omohyoid muscle has been observed in formalin embalmed male cadaver of South Indian origin. The muscular part of the superior belly of the omohyoid was completely absent. The inferior belly originated normally from the upper border of scapula, and continued with a fibrous tendon which ran vertically lateral to sternohyoid muscle and finally attached to the lower border of the body of hyoid bone. The fibrous tendon was about 1 mm thick and received a nerve supply form the superior root of the ansa cervicalis. As omohyoid mucle is used to achieve the reconstruction of the laryngeal muscles and bowed vocal folds, the knowledge of the possible anomalies of the omohyoid muscle is important during neck surgeries. Key words: Superior belly, Fibrous tendon, Omohyoid, Neck surgery Received March 12, 2014; Revised April 3, 2014; Accepted April 28, 2014 Introduction bellies, absence and adhesion to sternohyoid are the reported anomalies of the superior belly of the OH [2]. -

Thoracic and Lumbar Spine Anatomy
ThoracicThoracic andand LumbarLumbar SpineSpine AnatomyAnatomy www.fisiokinesiterapia.biz ThoracicThoracic VertebraeVertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature – Costal Fovea T1 T2-T8 T9-12 ThoracicThoracic VertebraeVertebrae andand RibRib JunctionJunction FunctionsFunctions ofof ThoracicThoracic SpineSpine – Costovertebral Joint – Costotransverse Joint MotionsMotions – All available – Flexion and extension limited – T7-T12 LumbarLumbar SpineSpine BodiesBodies PediclesPedicles LaminaeLaminae TransverseTransverse ProcessProcess SpinousSpinous ProcessProcess ArticularArticular FacetsFacets LumbarLumbar SpineSpine ThoracolumbarThoracolumbar FasciaFascia LumbarLumbar SpineSpine IliolumbarIliolumbar LigamentsLigaments FunctionsFunctions ofof LumbarLumbar SpineSpine – Resistance of anterior translation – Resisting Rotation – Weight Support – Motion IntervertebralIntervertebral DisksDisks RatioRatio betweenbetween diskdisk thicknessthickness andand vertebralvertebral bodybody heightheight DiskDisk CompositionComposition – Nucleus pulposis – Annulus Fibrosis SpinalSpinal LigamentsLigaments AnteriorAnterior LongitudinalLongitudinal PosteriorPosterior LongitudinalLongitudinal LigamentumLigamentum FlavumFlavum InterspinousInterspinous LigamentsLigaments SupraspinousSupraspinous LigamentsLigaments IntertransverseIntertransverse LigamentsLigaments SpinalSpinal CurvesCurves PosteriorPosterior ViewView SagittalSagittal ViewView – Primary – Secondary -

Levator Claviculae Muscle: a Case Report Konstantinos Natsis*, Stylianos Apostolidis, Elisavet Nikolaidou, Georgios Noussios, Trifon Totlis and Nikolaos Lazaridis
Open Access Case report Levator claviculae muscle: a case report Konstantinos Natsis*, Stylianos Apostolidis, Elisavet Nikolaidou, Georgios Noussios, Trifon Totlis and Nikolaos Lazaridis Address: Department of Anatomy, Medical School, Aristotle University of Thessaloniki, P.O. Box: 300, 54124 Thessaloniki, Greece Email: KN* - [email protected]; SA - [email protected]; EN - [email protected]; GN - [email protected]; TT - [email protected]; NL - [email protected] * Corresponding author Published: 15 May 2009 Received: 12 February 2008 Accepted: 8 April 2009 Cases Journal 2009, 2:6712 doi: 10.1186/1757-1626-2-6712 This article is available from: http://casesjournal.com/casesjournal/article/view/6712 © 2009 Natsis et al; licensee Cases Network Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract In the current study a levator claviculae muscle, found in a 65-year old male cadaver, is presented. We describe the topography and morphology of this accessory muscle, which may be found in 1-3% of the population. Moreover, we discuss the embryologic origin of the muscle along with its clinical importance. Introduction In the current study we present a case of a levator Levator claviculae or cleidocervical muscle is a super- claviculae muscle found in a cadaver and we discuss the numerary muscle in humans, in contrast to anthropoids embryologic origin of the muscle along with its clinical and lower mammals where this muscle is found normally importance. -

Comparing the Injectate Spread and Nerve
Journal name: Journal of Pain Research Article Designation: Original Research Year: 2018 Volume: 11 Journal of Pain Research Dovepress Running head verso: Baek et al Running head recto: Ultrasound-guided GON block open access to scientific and medical research DOI: http://dx.doi.org/10.2147/JPR.S17269 Open Access Full Text Article ORIGINAL RESEARCH Comparing the injectate spread and nerve involvement between different injectate volumes for ultrasound-guided greater occipital nerve block at the C2 level: a cadaveric evaluation In Chan Baek1 Purpose: The spread patterns between different injectate volumes have not yet been investigated Kyungeun Park1 in ultrasound-guided greater occipital nerve (GON) block at the C2 level. This cadaveric study Tae Lim Kim1 was undertaken to compare the spread pattern and nerve involvements of different volumes of Jehoon O2 dye using this technique. Hun-Mu Yang2,* Materials and methods: After randomization, ultrasound-guided GON blocks with 1 or 5 mL dye solution were performed at the C2 level on the right or left side of five fresh cadavers. The Shin Hyung Kim1,* suboccipital regions were dissected, and nerve involvement was investigated. 1 Department of Anesthesiology and Results: Ten injections were successfully completed. In all cases of 5 mL dye, we observed the Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University deeply stained posterior neck muscles, including the suboccipital triangle space. The suboccipital College of Medicine, Seoul, Republic and third occipital nerves, in addition to GONs, were consistently stained when 5-mL dye was 2 of Korea; Department of Anatomy, used in all injections (100%). Although all GONs were successfully stained in the 1-mL dye Yonsei University College of Medicine, Seoul, Republic of Korea cases, three of five injections (60%) concomitantly stained the third occipital nerves. -

Unusual Organization of the Ansa Cervicalis: a Case Report
CASE REPORT ISSN- 0102-9010 UNUSUAL ORGANIZATION OF THE ANSA CERVICALIS: A CASE REPORT Ranjana Verma1, Srijit Das2 and Rajesh Suri3 Department of Anatomy, Maulana Azad Medical College, New Delhi-110002, India. ABSTRACT The superior root of the ansa cervicalis is formed by C1 fibers carried by the hypoglossal nerve, whereas the inferior root is contributed by C2 and C3 nerves. We report a rare finding in a 40-year-old male cadaver in which the vagus nerve fused with the hypoglossal nerve immediately after its exit from the skull on the left side. The vagus nerve supplied branches to the sternohyoid, sternothyroid and superior belly of the omohyoid muscles and also contributed to the formation of the superior root of the ansa cervicalis. In this arrangement, paralysis of the infrahyoid muscles may result following lesion of the vagus nerve anywhere in the neck. The cervical location of the vagus nerve was anterior to the common carotid artery within the carotid sheath. This case report may be of clinical interest to surgeons who perform laryngeal reinnervation and neurologists who diagnose nerve disorders. Key words: Ansa cervicalis, hypoglossal nerve, vagus nerve, variations INTRODUCTION cadaver. The right side was normal. The neck region The ansa cervicalis is a nerve loop formed was dissected and the neural structures in the carotid by the union of superior and inferior roots. The and muscular triangle regions were exposed, with superior root is a branch of the hypoglossal nerve particular attention given to the organization of the containing C1 fibers, whereas the inferior root is ansa cervicalis. -

EDS Awareness in the TMJ Patient
EDS Awareness in the TMJ Patient TMJ and CCI with the EDS Patient “The 50/50” Myofascial Pain Syndrome EDNF, Baltimore, MD August 14,15, 2015 Generation, Diagnosis and Treatment of Head Pain of Musculoskeletal Origin Head pain generated by: • Temporomandibular joint dysfunction • Cervicocranial Instability • Mandibular deviation • Deflection of the Pharyngeal Constrictor Structures Parameters & Observations . The Myofascial Pain Syndrome (MPS) is a description of pain tracking in 200 Ehlers-Danlos patients. Of the 200 patients, 195 were afflicted with this pain referral syndrome pattern. The MPS is in direct association and correlation to Temporomandibular Joint dysfunction and Cervico- Cranial Instability syndromes. Both syndromes are virtually and always correlated. Evaluation of this syndrome was completed after testing was done to rule out complex or life threatening conditions. The Temporomandibular Joint TMJ Dysfunction Symptoms: Deceptively Simple, with Complex Origins 1) Mouth opening, closing with deviation of mandibular condyles. -Menisci that maybe subluxated causing mandibular elevation. -Jaw locking “open” or “closed”. -Inability to “chew”. 2) “Headaches”/”Muscles spasms” (due to decreased vertical height)generated in the temporalis muscle, cheeks areas, under the angle of the jaw. 3) Osseous distortion Pain can be generated in the cheeks, floor of the orbits and/or sinuses due to osseous distortion associated with “bruxism”. TMJ dysfunction cont. (Any of the following motions may produce pain) Pain With: . Limited opening(closed lock): . Less than 33 mm of rotation in either or both joints . Translation- or lack of . Deviations – motion of the mandible to the affected side or none when both joints are affected . Over joint pain with or without motion around or . -

Shoulder Anatomy & Clinical Exam
MSK Ultrasound - Spine - Incheon Terminal Orthopedic Private Clinic Yong-Hyun, Yoon C,T-spine Basic Advanced • Medial branch block • C-spine transforaminal block • Facet joint block • Thoracic paravertebral block • C-spine intra-discal injection • Superficial cervical plexus block • Vagus nerve block • Greater occipital nerve block(GON) • Third occipital nerve block(TON) • Hydrodissection • Brachial plexus(1st rib level) • Suboccipital nerve • Stellate ganglion block(SGB) • C1, C2 nerve root, C2 nerve • Brachial plexus block(interscalene) • Recurrent laryngeal nerve • Serratus anterior plane • Cervical nerve root Cervical facet joint Anatomy Diagnosis Cervical facet joint injection C-arm Ultrasound Cervical medial branch Anatomy Nerve innervation • Medial branch • Same level facet joint • Inferior level facet joint • Facet joint • Dual nerve innervation Cervical medial branch C-arm Ultrasound Cervical nerve root Anatomy Diagnosis • Motor • Sensory • Dermatome, myotome, fasciatome Cervical nerve root block C-arm Ultrasound Stallete ganglion block Anatomy Injection Vagus nerve Anatomy Injection L,S-spine Basic Advanced • Medial branch block • Lumbar sympathetic block • Facet joint block • Lumbar plexus block • Superior, inferior hypogastric nerve block • Caudal block • Transverse abdominal plane(TAP) block • Sacral plexus block • Epidural block • Hydrodissection • Interlaminal • Pudendal nerve • Transforaminal injection • Genitofemoral nerve • Superior, inferior cluneal nerve • Rectus abdominal sheath • Erector spinae plane Lumbar facet -

The Anomalous Human Levator Claviculae Muscle: a Case Report
Central Annals of Vascular Medicine & Research Case Report *Corresponding author Kunwar P Bhatnagar, Department of Anatomical Sciences and Neurobiology, University of Louisville, 7000 Creekton, USA, Tel: 150-2456-4779; Email: bhatnagar@ The Anomalous Human Levator louisville.edu Submitted: 08 February 2021 Claviculae Muscle: A Case Accepted: 20 February 2021 Published: 24 February 2021 ISSN: 2378-9344 Report Copyright © 2021 Bhatnagar KP, et al. Kunwar P Bhatnagar1* and Timothy D Smith2 OPEN ACCESS 1Department of Anatomical Sciences and Neurobiology, University of Louisville, USA 2School of Physical Therapy, Slippery Rock University, USA Keywords • Anomalous muscle • Levator claviculae Abstract • omo-trachelien • Omocervicalis This case report describes the observation of a unilaterally present anomalous levator claviculae muscle in a 66 -year-old human male. The observations were made during routine laboratory dissections. In our 80- • Sternomastoideus some years of cumulative human dissection education prior to this detection, this was the first observation (with about 45 cadavers dissected yearly) of this muscle. The levator claviculae muscle was observed with intact nerve supply from the ventral ramus of C3, indicating its functional status. The muscle was lambda (λ)-shaped with its stem oriented cranially, attaching to the fascia of the longus capitis muscle at the level of the transverse process of the fourth cervical vertebra. More inferiorly, the stem splits into a pars medialis and pars lateralis each with fascial attachments to the clavicle within the middle third of the bone. Both parts had fascial attachments to the clavicle within the middle third of the bone, and the lateral part passed medial to the external jugular vein. -

A Comprehensive Review of Anatomy and Regional Anesthesia Techniques of Clavicle Surgeries
vv ISSN: 2641-3116 DOI: https://dx.doi.org/10.17352/ojor CLINICAL GROUP Received: 31 March, 2021 Research Article Accepted: 07 April, 2021 Published: 10 April, 2021 *Corresponding author: Dr. Kartik Sonawane, Uncovering secrets of the Junior Consultant, Department of Anesthesiol- ogy, Ganga Medical Centre & Hospitals, Pvt. Ltd. Coimbatore, Tamil Nadu, India, E-mail: beauty bone: A comprehensive Keywords: Clavicle fractures; Floating shoulder sur- gery; Clavicle surgery; Clavicle anesthesia; Procedure review of anatomy and specific anesthesia; Clavicular block regional anesthesia techniques https://www.peertechzpublications.com of clavicle surgeries Kartik Sonawane1*, Hrudini Dixit2, J.Balavenkatasubramanian3 and Palanichamy Gurumoorthi4 1Junior Consultant, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India 2Fellow in Regional Anesthesia, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India 3Senior Consultant, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India 4Consultant, Department of Anesthesiology, Ganga Medical Centre & Hospitals, Pvt. Ltd., Coimbatore, Tamil Nadu, India Abstract The clavicle is the most frequently fractured bone in humans. General anesthesia with or without Regional Anesthesia (RA) is most frequently used for clavicle surgeries due to its complex innervation. Many RA techniques, alone or in combination, have been used for clavicle surgeries. These include interscalene block, cervical plexus (superficial and deep) blocks, SCUT (supraclavicular nerve + selective upper trunk) block, and pectoral nerve blocks (PEC I and PEC II). The clavipectoral fascial plane block is also a safe and simple option and replaces most other RA techniques due to its lack of side effects like phrenic nerve palsy or motor block of the upper limb. -

Omohyoid Muscle Syndrome
International Journal of Research in Medical Sciences Maengkom FA et al. Int J Res Med Sci. 2020 Mar;8(3):1127-1129 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20200497 Case Report Omohyoid muscle syndrome Fika Amanda Maengkom, Putu Anda Tusta Adiputra* Department of General Surgery, Sanglah General Hospital, Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia Received: 30 December 2019 Accepted: 15 January 2020 *Correspondence: Dr. Putu Anda Tusta Adiputra, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Omohyoid muscle syndrome is a rare cause of a bulging lateral neck mass that occurs on swallowing that often a worrisome observation because of the concern of malignancy and cosmetic deformity. The first case has been documented on 1969. A 12 years old male came to Surgical Oncology Outpatient Clinic with chief complaint a protruding right lateral neck mass during swallowing. He noticed this complaint since three months prior. He had no previous history of medical illness. He had history of multiple chokehold trauma when playing with his friend 6 months ago. He had no symptoms besides the mass occurring on his right neck. The patient went through the cervical radiograph and neck ultrasonography examination. There were inconclusive results. The patient was informed that the implication of these findings was strictly cosmetic and did not pose any risk of long-term consequence. -
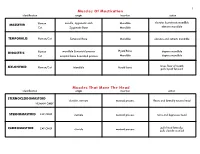
Muscles of Mastication Muscles That Move the Head
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts,