ANATOMY of VISION: the VISUAL PATHWAYS by Ph.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lacrimal Obstruction
Yung_edit_final_Layout 1 01/09/2009 15:19 Page 81 Lacrimal Obstruction Proximal Lacrimal Obstruction – A Review Carl Philpott1 and Matthew W Yung2 1. Rhinology and Anterior Skull Base Fellow, St Paul’s Sinus Centre, St Paul’s Hospital, Vancouver; 2. Department of Otolaryngology, Ipswich Hospital NHS Trust Abstract While less common than distal lacrimal obstruction, proximal obstruction causes many cases of epiphora. This article examines the aetiology of proximal lacrimal obstruction and considers current management strategies with reference to recent literature. The Lester Jones tube is the favoured method of dealing with most cases of severe proximal obstruction; other methods have been tried with less success. Keywords Proximal lacrimal obstruction, epiphora, canalicular blockage, Lester Jones tube Disclosure: The authors have no conflicts of interest to declare. Received: 31 March 2009 Accepted: 14 April 2009 DOI: 10.17925/EOR.2009.03.01.81 Correspondence: Matthew W Yung, The Ipswich Hospital, Heath Road, Ipswich, Suffolk, IP4 5PD, UK. E: [email protected] Obstruction of the lacrimal apparatus commonly causes sufferers to dominant fashion.3 Where absence of the punctum and papilla present with symptoms of epiphora, for which they are commonly (congenital punctal agenesis) occurs, it is likely that more distal parts referred to ophthalmology departments. In those units where of the lacrimal apparatus are obliterated. collaboration with otorhinolaryngology occurs, the distal site of obstruction is usually dealt with. -

(12) Patent Application Publication (10) Pub. No.: US 2013/0172829 A1 BADAW (43) Pub
US 2013 0172829A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0172829 A1 BADAW (43) Pub. Date: Jul. 4, 2013 (54) DRY EYE TREATMENT SYSTEMS (52) U.S. Cl. CPC .................................... A61F 9/0008 (2013.01) (71) Applicant: SIGHT SCIENCES, INC., San USPC .......................................................... 604/294 Francisco, CA (US) (72) Inventor: Paul BADAWI, San Francisco, CA (US) (57) ABSTRACT (73) Assignee: SIGHT SCIENCES, INC., San Dry eye treatment apparatus and methods are described Francisco, CA (US) herein which generally comprise a patch or strip affixed to the skin of the upper and/or lower eyelids to deliver heat or other (21) Appl. No.: 13/645,985 forms of energy, pressure, drugs, moisture, etc. (alone or in combination) to the one or more meibomianglands contained (22) Filed: Oct. 5, 2012 within the underlying skin. The treatment strip or strips include one or more strips configured to adhere to an under Related U.S. Application Data lying region of skin in proximity to one or both eyes of a (63) Continuation-in-part of application No. 13/343,407, subject such that the one or more strips allow for the subject filed on Jan. 4, 2012. to blink naturally without restriction from the one or more patches. Moreover, the one or more Strips may be configured Publication Classification to emit energy to the underlying region of skin and where the one or more strips are shaped to follow a location of one or 51) Int.nt. CC. more me1bOm1amibomiam gland S COnta1nedined W1thinwithin the underlyingunderW1n A6DF 9/00 (2006.01) region of skin. -
Eyelids (2 Lec.)
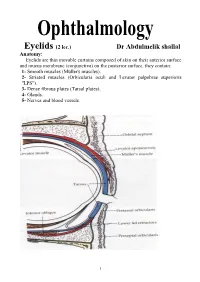
Eyelids (2 lec.) Dr Abdulmelik shallal Anatomy: Eyelids are thin movable curtains composed of skin on their anterior surface and mucus membrane (conjunctiva) on the posterior surface, they contain: 1- Smooth muscles (Müller's muscles). 2- Striated muscles (Orbicularis oculi and Levator palpebrae superioris "LPS"). 3- Dense fibrous plates (Tarsal plates). 4- Glands. 5- Nerves and blood vessels. 1 The contents of the lid are distributed as follows: the anterior surface is made of skin which has a round edge with the lid margin, the subcutaneous tissue, muscular layer, the submuscular (areolar tissue) layer, the orbital septum which end as a tarsal plate (that forms the architecture of lid) and finally the conjunctiva (palpebral) which is situated most posterior. The free margin of the eyelids contains: 1- The lashes (Cilia). 2- Grey line. 3- Orifices of Meibomian glands. 4- Mucocutaneous junction 5- Superior and inferior puncti of Naso-Lacrimal System (NLS). Muscles of the eyelids: 1- Orbicularis oculi muscle: It is a thin oval sheet of concentric striated muscle surrounding the palpebral fissure. It can be divided into: a- Peripheral (orbital) part: This is involved in forceful closure of lids. b- Central (palpebral) part: This is involved in involuntary blinking, voluntary nonforceful closure and participates in forceful closure with the orbital part. c- Muscle of Rioland's: this part is represented by the gray line of lid margin. d- lacrimalis muscle: that attached to the fundus of lacrimal sac. This part is involved in pumping action of lacrimal drainage system. Nerve supply: Sensory: Ophthalmic branch of trigeminal nerve Motor: Facial nerve. -

Procedural Article
Procedural Article The occasional eyelid lesion Mitchell Crozier, INTRODUCTION ANATOMY/ETIOLOGY BHK1, Sarah M. Giles, BSc, Physicians in the primary and External hordeola originate from an MD2 urgent care settings frequently acute staphylococcal infection of the 1School of Medicine, Faculty encounter patients presenting with sebaceous glands (Glands of Zeiss) or of Medicine, acute inflammatory eyelid nodules modified apocrine glands (Glands of University of Ottawa, and eyelid swelling. The external Moll) found along the margin of the Ottawa, ON, Canada, hordeolum, which is a painful infection upper and lower eyelid.3,4 Together, 2Department of Family Medicine, Faculty of involving the eyelid and referred the Glands of Zeiss and Moll produce Medicine, University of to as a ‘stye’ in clinical practice, is secretions with antibacterial and Ottawa, Ottawa, ON, one of the most common eye/eyelid immune defence properties.1,4,8 The Canada conditions reported by the general Glands of Zeis secrete into a duct at 1‑3 Correspondence to: population. There are no known the base of the eyelash hair follicle, Sarah M. Giles, age, sex or demographic differences while the Glands of Moll secrete [email protected] in the prevalence of external hordeola directly to the eyelid surface next to but patients with chronic conditions the base of the eyelashes and anterior This article has been peer 8 reviewed such as diabetes, dyslipidaemia and to the meibomian glands. When the seborrheic dermatitis may be at an glands become blocked, or if stasis increased risk.4,5 occurs, bacterial proliferation and Patients with an external infection can occur. As the infection hordeolum present with an acute‑onset results in a localised inflammatory red, painful and swollen abscess along response, a purulent and palpable the margin of the eyelid. -

Biomarkers in Sebaceous Gland Carcinomas
3/24/2017 Biomarkers in Sebaceous Gland Carcinomas Sander R. Dubovy, MD Professor of Ophthalmology and Pathology Victor T. Curtin Chair in Ophthalmology Florida Lions Ocular Pathology Laboratory Bascom Palmer Eye Institute University of Miami Miller School of Medicine Biomarkers in Sebaceous Gland Carcinomas Disclosure of Relevant Disclosure of Relevant Financial Relationships Financial Relationships USCAP requires that all planners (Education Committee) in a position to Dr. Sander R. Dubovy declares he has no conflict(s) of interest influence or control the content of CME disclose any relevant financial to disclose. relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner have, or have had, within the past 12 months, which relates to the content of this educational activity and creates a conflict of interest. Biomarkers in Sebaceous Gland Carcinomas Outline Introduction • Sebaceous carcinoma (SC) is a malignant neoplasm that arises from • Introduction to sebaceous cell carcinoma the sebaceous glands, most commonly in the periocular areas. • Incidence, demographics, risk factors • Clinical manifestations are often mistaken for benign conditions and • Ocular origins thus proper diagnosis and management is delayed. • Gross pathology • Metastases to regional lymph nodes and other sites are common. • Microscopic pathology • Immunohistochemistry • Management • Cases Biomarkers in Sebaceous Gland Carcinomas Biomarkers in Sebaceous Gland Carcinomas 1 3/24/2017 Introduction Sebaceous Gland • Pathologists should be aware of the -

Ophthalmology
LECTURE NOTES For Health Science Students Ophthalmology Dereje Negussie, Yared Assefa, Atotibebu Kassa, Azanaw Melese University of Gondar In collaboration with the Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education 2004 Funded under USAID Cooperative Agreement No. 663-A-00-00-0358-00. Produced in collaboration with the Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education. Important Guidelines for Printing and Photocopying Limited permission is granted free of charge to print or photocopy all pages of this publication for educational, not-for-profit use by health care workers, students or faculty. All copies must retain all author credits and copyright notices included in the original document. Under no circumstances is it permissible to sell or distribute on a commercial basis, or to claim authorship of, copies of material reproduced from this publication. ©2004 by Dereje Negussie, Yared Assefa, Atotibebu Kassa, Azanaw Melese All rights reserved. Except as expressly provided above, no part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without written permission of the author or authors. This material is intended for educational use only by practicing health care workers or students and faculty in a health care field. PREFACE This lecture note will serve as a practical guideline for the hard-pressed mid-level health workers. We hope that it will be a good introduction to eye diseases for health science students working in Ethiopia. -
A Unification Theory for Dry Eye and Blepharitis Open Access to Scientific and Medical Research DOI
Journal name: Clinical Ophthalmology Article Designation: Hypothesis Year: 2016 Volume: 10 Clinical Ophthalmology Dovepress Running head verso: Rynerson and Perry Running head recto: DEBS – a unification theory for dry eye and blepharitis open access to scientific and medical research DOI: http://dx.doi.org/10.2147/OPTH.S114674 Open Access Full Text Article HYPOTHESIS DEBS – a unification theory for dry eye and blepharitis James M Rynerson1 Abstract: For many years, blepharitis and dry eye disease have been thought to be two distinct Henry D Perry2 diseases, and evaporative dry eye distinct from aqueous insufficiency. In this treatise, we propose a new way of looking at dry eye, both evaporative and insufficiency, as the natural sequelae of 1BlephEx, LLC, Alvaton, KY, 2Department of Ophthalmology, decades of chronic blepharitis. Dry eye is simply the late form and late manifestation of one Nassau University Medical Center, disease, blepharitis. We suggest the use of a new term in describing this one chronic disease, Hofstra University School of Medicine, East Meadow, NY, USA namely dry eye blepharitis syndrome (DEBS). Bacteria colonize the lid margin within a structure known as a biofilm. The biofilm allows for population densities that initiate quorum-sensing gene activation. These newly activated gene products consist of inflammatory virulence factors, such as exotoxins, cytolytic toxins, and super-antigens, which are then present for the rest of the patient’s life. The biofilm never goes away; it only thickens with age, producing increasing quantities of bacterial virulence factors, and thus, increasing inflammation. These virulence For personal use only. factors are likely the culprits that first cause follicular inflammation, then meibomian gland dysfunction, aqueous insufficiency, and finally, after many decades, lid destruction. -

5 Cases, 1 Cause of Irritated Eyes
PHOTO ROUNDS Kimia Ziahosseini, MD 5 cases, 1 cause Stockport Eye Centre, Stepping Hill Hospital, Stockport, Cheshire, of irritated eyes United Kingdom rritated and watery eyes. Mild ery- of his left eye that had been bothering him [email protected] thema of the nasal bulbar conjunc- for the last 2 weeks. He had been treated Thabit A. Mustafa Odat, tiva. Photophobia. Blurred vision. with a topical antibiotic, but showed no MBBS, FRCS, JBO I Oculoplastic and Orbital These were just some of the signs and improvement. Surgeon, King Hussein Medical symptoms that prompted the following CASE 4 A 15-year-old girl came in com- Centre, Amman, Jordan 5 patients to seek treatment. Though plaining of irritation of the left eye over f E a TU r E E d ITO r the specifics of their cases varied, their the last month. She was seen by an oph- Richard P. Usatine, MD diagnosis was the same. thalmologist, who attributed her symp- University of Texas Health CASE 1 A 35-year-old man presented toms to exposure keratopathy due to lag- Science Center at San Antonio with a foreign-body sensation and tear®- Dowdenophthalmos—inability Health to close,Media or poor ing of his right eye that had lasted for a closure of, the eyelids (FIGURE). He treated few days. The eye showed mild erythema her with different lubricants and antibiot- of the nasal bulbar conjunctivaCopyright andFor linear personalics, without improvement. use only corneal abrasions. CASE 5 A 15-year-old boy came in com- CASE 2 A 23-year-old woman came in plaining of blurred vision in his right eye. -

Differential Incidence of Eyelid Margin Cysts in ASU Outpatients
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (6), Page 4761-4764 Differential Incidence of Eyelid Margin Cysts in ASU Outpatients Mayar Mohammad Salaheldin Faheem, Sherif Elwan, Azza Mohamed Ahmed Said, Ossama Tarek Nada Department of Ophthalmology, Faculty of Medicine, Ain Shams University Corresponding author: Mayar Mohammad Salaheldin Faheem, E-Mail: [email protected], Mobile: +2 01097316366 ABSTRACT Background: Wide varieties of lesions affecting the eyelid are encountered within routine Ophthalmology practice. These lesions are numerous due to the unique anatomical features of the eyelid as the whole skin structures, appendages, muscle, modified glands, and conjunctival mucous membrane are represented in the eyelid. The eyelid comprises different types of glands that clinically correlate with the development of eyelid cysts; Sebaceous glands (Meibomian glands and glands of Zeis), aporcine glands (glands of Moll) and eccrine sweat glands. Objectives: To report the incidence of the different etiologies of eyelid margin cysts in Ain Shams University (ASU) Hospital, General Ophthalmology Outpatients Clinic. Patients and Methods: It included all patients who presented to the General Ophthalmology Outpatient Clinic, 6 days per week for one month (November 2017) complaining of eyelid margin lesions, found cystic on slit lamp examination, of all ages. Results: The total number of patients recorded was 45 patients presenting with eyelid margin cysts, out of 1920 patients visiting the General Ophthalmology Outpatient Clinic during the month of November 2017 with an incidence of 2.34%. Seven types of cysts were found namely; External Hordeolum (8.9%), Internal Hordeolum (15.6%), Chalazion (28.9%), Sebaceous Cyst (11.1%), Cyst of Zeis Gland (13.3%), Apocrine Hidrocystoma (11.1%) and Eccrine Hidrocystoma (11.1%). -

Benign Eye Lid Lesions Arnab Biswas1
Review Article Benign eye lid lesions Arnab Biswas1 (Excerpts from Eyelid Tumor Clinical Evaluation and Reconstruction Techniques Authors: Biswas, Springer; 2014 edition) ny Eyelid mass or ulcer could be a benign or a Seboric Keratosis malignant lesion. An accurate diagnosis can be A Introduction: Seborrheic keratosis( Basal cell reached based on history and clinical examination. If in papilloma,seborrheic warts) are common benign lesions doubt surgical biopsy followed by histo pathological on the face and abdomen. It can also present on the lids evaluation can clinch the diagnosis. In this review article of aging individuals. we look at some of the more common eyelid lesions that an ophthalmologist may encounter in a general practice. Clinical Features: They are well circumscribed, waxy, friable and appear stuck on to the skin. Some lesions are covered BENIGN TUMORS OF EPIDERMIS by an adherent greasy-appearing scale and are raised Squamous Papilloma above the surface of the skin. They can feel soft and greasy. Introduction: It is one of the most common benign eye lid The shape is round to oval, and multiple lesions may be lesion. It is not a specific clino-pathological entity. aligned in the direction of skin folds.The lesion is very superficial and may be pigmented from slight discolouration to deep brown in colour. Prognosis: They are usually assymptomatic, but can sometimes cause pruritis and irritation. Treatment Options: Treatment involves surgical excision or laser ablation Inverted Folicular Keratosis Introduction: It is a benign cutaneous lesion almost similar in character to seborrheic keratosis. The term Inverted A large pailomatous growth from lateral aspect of lower lid follicular karatosis is a misnomer, as it was thought that Age of Presentation: It is a group of condition that usually presents in middle or elderly age. -

Malignant Lymphoma of the Lacrimal Canaliculi: a Rare Case Report
Malignant Lymphoma of The Lacrimal Canaliculi: A Rare Case Report Banu Aji Dibyasakti1,2, Yunia Irawati3,4, Hernawita Soeharko4, Darmayanti Siswoyo4 1Division of Reconstructive Surgery, Oculoplasty, and Oncology, Department of Ophthalmology, Dr. Sardjito General Hospital, Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada, Yogyakarta, Indonesia 2Fellow at JEC Eye Hospitals and Clinics, Jakarta, Indonesia 3Division of Plastic and Reconstructive Surgery, Department of Ophthalmology, Faculty of Medicine Universitas Indonesia, dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia 4JEC Eye Hospitals and Clinics, Jakarta, Indonesia Background: Malignant lymphoma in the lacrimal system is a rare case of ocular malignancy. It is often caused by immunosuppressive conditions or associated with older age. We aim to conduct a careful examination of canaliculi mass especially a suspect for malignant to be completed with histopathology and discuss the diagnosis and management of malignant lymphoma in the lacrimal canaliculus. Results: A woman, 60 years old, presented with a swollen left upper eyelid, red eye, and eye discharge. She had been assessed as blepharoconjunctivitis and received adequate antibiotics for the last four months. However, her complaints persisted. She had ocular pain, itchiness, yellowish thick eye discharge. History of previous tumor was denied. Physical examination revealed a swollen lacrimal punctum on the left upper eyelid, depicted a ‘fish mouth appearance’ with volume 3.0 x 3.0 x 3.0 mm. Irrigation test showed a negative result with a positive regurgitation discharge. Punctum incision and curettage were performed using local anesthesia. The curettage procedure revealed a dacryolith on the upper side and a purplish-red mass on the lower side. -

Jemds.Com Original Research Article
Jemds.com Original Research Article ANALYSIS OF 34 CASES OF ENDONASAL ENDOSCOPIC DACRYOCYSTORHINOSTOMY- SURGICAL SUCCESS AND PATIENT SATISFACTION, A CASE SERIES, OUR EXPERIENCE N. Gopinathan Pillai1, Binu Babu2, Anjana Mary Reynolds3, Subadhra S4 1Associate Professor, Department of Otorhinolaryngology, PIMSRC, Thiruvalla. 2Assistant Professor, Department of Otorhinolaryngology, PIMSRC, Thiruvalla. 3Assistant Professor, Department of Otorhinolaryngology, PIMSRC, Thiruvalla. 4Junior Resident, Department of Otorhinolaryngology, PIMSRC, Thiruvalla. ABSTRACT BACKGROUND The conventional treatment of dacryocystitis is external dacryocystorhinostomy. Its success rate varies from 80 - 98%.1-4 But patient’s satisfaction was poor due to facial scar, disruption of medial canthus anatomy and dysfunction of lacrimal pump mechanism. Endoscopic DCR has neither facial scar nor any postoperative distortion of lacrimal pump mechanism and medial canthal anatomy. The objective of this study is to assess the surgical success rate and patient’s satisfaction after endonasal endoscopic Dacryocystorhinostomy (DCR). Study Design- This study was done at Pushpagiri Institute of Medical Sciences and Research Centre, Thiruvalla, between January 2012 and August 2016. There were 34 patients included in this study. Females are more commonly affected than males. Unilateral cases are more than bilateral cases. Their age ranges from 13 - 83 years. Mean age is 35 years. MATERIALS AND METHODS Patients presented with epiphora or swelling below the medial canthus of eye with or without pain, mucopurulent regurgitation from the lacrimal sac into the eye on pressing the swelling. Five patients had concomitant deviated nasal septum, for which septoplasty was done along with DCR. The patency of nasolacrimal duct was assessed by syringing and diagnostic nasal endoscopy. RESULTS The success rate is comparable to other studies of endonasal DCR.