Clinical Dermatology Notice
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
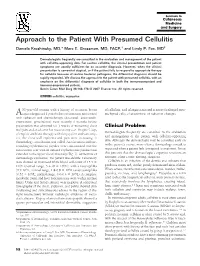
Approach to the Patient with Presumed Cellulitis Daniela Kroshinsky, MD,* Marc E
Approach to the Patient With Presumed Cellulitis Daniela Kroshinsky, MD,* Marc E. Grossman, MD, FACP,† and Lindy P. Fox, MD‡ Dermatologists frequently are consulted in the evaluation and management of the patient with cellulitic-appearing skin. For routine cellulitis, the clinical presentation and patient symptoms are usually sufficient for an accurate diagnosis. However, when the clinical presentation is somewhat atypical, or if the patient fails to respond to appropriate therapy for cellulitis because of routine bacterial pathogens, the differential diagnosis should be rapidly expanded. We discuss the approach to the patient with presumed cellulitis, with an emphasis on the differential diagnosis of cellulitis in both the immunocompetent and immunucompromised patient. Semin Cutan Med Surg 26:168-178 © 2007 Elsevier Inc. All rights reserved. KEYWORDS cellulitis, erysipelas 53-year-old woman with a history of recurrent breast of cellulitis, and telangiectasia and scattered enlarged mes- Acancer diagnosed 2 years before presentation and treated enchymal cells, characteristic of radiation changes. with radiation and chemotherapy (docetaxel, anastrozole, exemestane, gemcitabine) most recently 6 months before presentation was admitted for 3 weeks of worsening chest Clinical Problem wall pain and a rash over her mastectomy scar. Despite 5 days Dermatologists frequently are consulted in the evaluation of empiric antibiotic therapy with doxycycline and vancomy- and management of the patient with cellulitic-appearing cin, the chest wall erythema and pain were increasing. A dermatology consultation was called. An ulceration and sur- skin. Although the dermatologist may be consulted early on rounding erythematous papules were concentrated over the in the patient’s course, more often a dermatology consult is mastectomy scar with ill-defined erythematous patches that requested when a patient fails to respond to treatment. -

Bacterial Infections and Infectious Dermatologic Emergencies.Pdf
Learning Objectives Common Bacterial Infections recognition treatment complications Infectious Dermatologic Emergencies Necrotizing Fasciitis Toxic Shock Syndromes Normal Skin Flora Major function is to prevent skin infections Provides ecological competition for pathogens Hydrolyzes the lipids in sebum into free fatty acids which are toxic to many bacteria- linoleic and linolenic acid are more inhibitory of Staph Aureus Antimicrobial Peptides from lamellar bodies, Cathelicidins, and Defensins function to control overgrowth of pathogens Normal Skin Flora Aerobic Cocci Staphylococcus epidermidis Most common coccus on human skin All body sites, especially intertriginous areas Staphylococcus aureus More common in Atopic Dermatitis, Diabetes Mellitus, Hemodialysis, IVDU, Liver Disease, and HIV resident or contaminant? anterior nares- 20-35% perineum- 20% axillae and toe webs- 5-10% Normal Skin Flora Aerobic Coryneform Bacteria Corynebacterium minutissimum- intertriginous sites Erythrasma Anaerobic Coryneform Bacteria Propionibacterium acnes- sebaceous glands, hair follicles Acne vulgaris Gram Negative Bacteria Acinetobacter species- axillae, perineum, antecubital fossae - Requires moisture and maceration which increases pH and CO2 levels Yeast Pityrosporum ovale/Malassezia furfur- sebaceous sites Tinea Versicolor Introduction Strep and Staph cause the majority of skin infections in immunocompetent patients Immunodeficiency and underlying systemic disease result in severe infections which tend to be refractory to -

15. Dermatology Eponyms
Dermatology Eponyms DERMATOLOGY EPONYMS – PHENOMEN / SIGN – LEXICON (D) Brzeziński Piotr1, Wollina Uwe2, Poklękowska Katarzyna3, Khamesipour Ali4, Herrero Gonzalez Jose Eugenio5, Bimbi Cesar6, Di Lernia Vito7, Karwan Krzysztof 8 16th Military Support Unit, Ustka, Poland. [email protected] 2Department of Dermatology & Allergology, Hospital Dresden-Friedrichstadt, Academic Teaching Hospital of the Technical University of Dresden, Dresden, Germany [email protected] 3Mazowiecki Branch of the National Health Fund, Warsaw, Poland [email protected] 4Center for Research and Training in Skin Diseases and Leprosy, Tehran University of Medical Sciences, Tehran, Iran [email protected] 5Malalties Ampul.lars i Porfíries, Departament de Dermatologia, Hospital del Mar, Barcelona, Spain [email protected] 6Brazilian Society of Dermatology [email protected] 7Department of Dermatology, Arcispedale Santa Maria Nuova, Reggio Emilia, Italy [email protected] 8The Emergency Department, Military Institute of Medicine, Warsaw, Poland [email protected] N Dermatol Online. 2011; 2(3): 158-170 Date of submission: 08.04.2011 / acceptance: 29.05.2011 Conflicts of interest: None DANIELSSEN’S SIGN Anesthetic leprosy. A form of leprosy chiefly affecting the nerves, marked by hyperesthesia succeeded by anesthesia, and by paralysis, ulceration, and various trophic disturbances, terminating in gangrene and mutilation. In 1895 I presented to the Ohio State Medical Society two sisters, natives of Ohio, who manifested appearances of anesthetic leprosy. Synonyms: Danielssen disease, Danielssen-Boeck disease, dry leprosy, trophoneurotic leprosy. OBJAW DANIELSSENA Anesthetic leprosy. Postać trądu głównie wpływająca na nerwy, początkowo charakteryzuje się oznaczone przeczulicą, następcą znieczulicą i paraliŜem, owrzodzeniem i róŜnymi zaburzeniami troficznymi, kończąca się w gangreną i okaleczeniem. W 1895 roku przedstawiono w Ohio State Medical Society dwie siostry z Ohio, u których występowały objawy anesthetic Figure 1. -

Clinical Dermatology Notice
This page intentionally left blank Clinical Dermatology Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The editors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the editors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of such information contained in this work. Readers are encouraged to confirm the information contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. a LANGE medical book Clinical Dermatology Carol Soutor, MD Clinical Professor Department of Dermatology University of Minnesota Medical School Minneapolis, Minnesota Maria K. Hordinsky, MD Chair and Professor Department of Dermatology University of Minnesota Medical School Minneapolis, Minnesota New York Chicago San Francisco Lisbon London Madrid Mexico City Milan New Delhi San Juan Seoul Singapore Sydney Toronto Copyright © 2013 by McGraw-Hill Education, LLC. -

World Journal of Clinical Pediatrics
World Journal of W J C P Clinical Pediatrics Submit a Manuscript: http://www.f6publishing.com World J Clin Pediatr 2018 October 25; 7(4): 89-104 DOI: 10.5409/wjcp.v7.i4.89 ISSN 2219-2808 (online) REVIEW Perianal infectious dermatitis: An underdiagnosed, unremitting and stubborn condition Elena Daniela Serban Elena Daniela Serban, 2nd Department of Pediatrics, “Iuliu ficial inflammation of the perianal skin, which is of bac Hatieganu” University of Medicine and Pharmacy, Emergency terial origin (classically, group A betahemolytic strepto Hospital for Children, Cluj-Napoca 400177, Romania cocci). This narrative review aims to critically review and summarize the available scientific literature regarding ORCID number: Elena Daniela Serban (0000-0003-0906-1232). pediatric PID, being the first of its kind, to the best of Author contributions: Serban ED contributed to the paper’s the author’s knowledge. It also reports the first cases of conception and design, the data collection, extraction, analysis Romanian children with PID. Multiple databases were and evaluation, the interpretation of results, and the manuscript’s subjected to systematic literature search (from 1966 preparation, critical revision, editing and final submission. to April 30, 2018) to identify studies and case reports of children with PID. As such, this review provides up Conflict-of-interest statement: The author declares there are no dated information about essential aspects of PID (epi potential conflicts of interest relevant to this publication. demiology, etiology, pathogenesis, as well as clinical OpenAccess: This article is an open-access article which was features, required investigations and therapeutic options) selected by an in-house editor and fully peer-reviewed by external and of diagnostic pitfalls. -

A ABCD, 19, 142, 152 ABCDE, 19, 142 Abramowitz Sign, 3, 5
Index A Atopic dermatitis, 2, 18, 19, 20, 30, ABCD, 19, 142, 152 61, 81, 82, 84, 86, 99 ABCDE, 19, 142 Atrophie blanche, 173, 177 Abramowitz sign, 3, 5 Atrophy, crinkling, 143, 160 Acanthosis nigricans, 105, 106, 132 Atypical nevus, 144, 145, 163, 164 Addison disease (primary adrenal eclipse, 144, 164 insufficiency), 137 ugly duckling, 144, 163 Albright (McCune–Albright Auspitz sign, 3, 5, 6, 18, 104 syndrome), 83, 93 All in different stages, 33, 34, 40 All in same stage, 33, 34, 38 B Alopecia, 57, 77, 94, 105, 106, 111, Bamboo hair, 84, 99, 171, 172 117, 119, 127, 133, 171, 172, Basal cell carcinoma, 17, 104, 140, 182, 184 151, 162, 170 Alopecia areata, 105, 106, 127, 171 Bioterrorism, 33, 38 Amyloid, 107, 119 Black dot (tinea capitis), 37, 57 Angiofibroma, 89 Blue angel (see Tumors, painful) Angiokeratoma, 3, 79, 81, 85 Blue rubber bleb nevus, 144, Angiolipoma, 142, 155 154, 168 Angioma, spider, 107, 109, 134 angiolipioma, 142, 155 Angiomatosis, leptomeningeal, 90 neurilemmoma, 142, 156 Anticoagulant, lupus, 108, 121 glomus tumor, 142, 157 Antiphospholipid syndrome eccrine spiradenoma, 142, 158 (APLS), 19, 107, 108, 121 leiomyoma, 142, 159 Apocrine hidrocystoma, 144, Blue cyst (apocrine hidrocystoma), 166, 168 144, 166, 168 Apple jelly, 36, 37, 47 Blue nose (purpura fulminans), 19, Ash leaf macule (confetti macule), 108, 122 82, 89 Blue papule (blue nevus), 1, 144, Asymmetry, 19, 118, 136, 152 166, 167, 168 187 188 Index Blue rubber bleb nevus, 144, 154, 168 Coast of California, 82, 83, 91 Border Coast of Maine, 83, 93 irregular, 83, -

Reading List 2012.Indd
General Reading iGAS Guidelines - Published January 2012 CLICK HERE Educational Interim UK guidelines for management of close community contacts of invasive group A streptococcal disease. Health Protection Agency, Workshops 2012 Group A Streptococcus Working Group. Communicable Disease and Public Health 2004; 7(4):354-361. CLICK HERE Keynote Presentation: Diagnosis and Complicated infections of skin and skin structures: when the infection is more than skin deep. DiNubile MJ, Lipsky, B. Journal of treatment Antimicrobial Chemotherapy, 2004, 53, Suppl. S2, ii37-ii50 of skin and soft CLICK HERE Practice guidelines for the diagnosis and management of skin and tissue infections soft tissue infections. Stevens DL et al. Clinical Infectious Disease 2005; 41:1373–1406 CLICK HERE Infections of skin and soft tissue: Outcomes of a classifi cation scheme. Eron J. Clinical Infectious Diseases 2000;31:287(A432). CLICK HERE Occurrence and antimicrobial susceptibility patterns of pathogens isolated from skin and soft tissue infections: report from the SENTRY READING Antimicrobial Surveillance Program (United States and Canada, 2000). Rennie RP et al. Diagn Microbiol Infect Dis. 2003 Apr; 45(4):287-293. LIST CLICK HERE Comparison of community and health care associated methicillin resistant Staphylococcus aureus infection. Naimi TS, et al. JAMA 2003; 290: 2976-2984 CLICK HERE Methicillin resistant S. aureus infections amoung patients in the emergency department. Moran GJ et al. The New England Journal of Medicine 2006 CLICK HERE HPR 2011;5(7): News CLICK HERE Polyclonal multiply antiobiotic-resistant methicillin-resistant Staphylococcus aureus with Panton-Valentine leucocidin in England. JAC 2009; doi: 10.1093/jac/dkp386; CLICK HERE Eff ect of antibiotics on Staphylococcus aureus producing panton- valentine leukocidin. -
Evidence-Based Management of Skin and Soft-Tissue Infections In
VISIT US AT BOOTH # 203 AT THE ACEP PEDIATRIC ASSEMBLY IN NEW YORK, NY, MARCH 24-25, 2015 February 2015 Evidence-Based Management Volume 12, Number 2 Authors Of Skin And Soft-Tissue Jennifer E. Sanders, MD Pediatric Emergency Medicine Fellow, Department of Emergency Medicine, Icahn School of Medicine at Mount Sinai, Infections In Pediatric Patients New York, NY Sylvia E. Garcia, MD Assistant Professor of Pediatrics and Pediatric Emergency In The Emergency Department Medicine, Icahn School of Medicine at Mount Sinai, New York, NY Abstract Peer Reviewers Jeffrey Bullard-Berent, MD, FAAP, FACEP Skin and soft-tissue infections are among the most common condi- Health Sciences Professor, Emergency Medicine and Pediatrics, University of California – San Francisco, Benioff tions seen in children in the emergency department. Emergency de- Children’s Hospital, San Francisco, CA partment visits for these infections more than doubled between 1993 Carla Laos, MD, FAAP and 2005, and they currently account for approximately 2% of all Pediatric Emergency Medicine Physician, Dell Children’s Hospital, Austin, TX emergency department visits in the United States. This rapid increase CME Objectives in patient visits can be attributed largely to the pervasiveness of community-acquired methicillin-resistant Staphylococcus aureus. The Upon completion of this article, you should be able to: 1. Describe the pathophysiology of community-acquired emergence of this disease entity has created a great deal of controver- methicillin-resistant Staphylococcus aureus. sy regarding treatment regimens for skin and soft-tissue infections. 2. Differentiate the clinical presentation of common skin and soft-tissue infections. This issue of Pediatric Emergency Medicine Practice will focus on the 3. -

Fingernails and Toenails Are There for Two Reasons
ingernails and toenails are there for two reasons: Fadornment and function. The desire to dress up nails dates back to the dawn of time, and it also seems to start very early in life. For instance, my daughter first demon strated a strong interest in her nails at the age of three. She would corral her mother and any available baby-sitter into painting her nails, and the more shocking the color, the more gleeful she became. Nonetheless, these hard and durable parts of our hands actually serve other needs as well. For one thing, they assist in dexterity. One day, my five-year-old son decided he didn't need his nails anymore. To prove him wrong, we put small pieces of modeling clay under his fin gertips, so it was as though he had no nails. My challenge to him: if he could pick up a dime with his fingers altered in this way, he could keep the dime. He failed several times, finally understanding how important nails are to everyday life. Nails serve another important purpose, at least to doc tors: they are a kind of external warning system because often it's there that the outward signs of internal disease may develop. Finally, in the world of dermatology, we are especially aware of the greatest importance of nails: scratching that pesky itch. © Copyright 2000, David J. Leffell. MD. All rights reserved. 166 L 0 0 kYo u r Be st Nails are actually an integral part of the skin. The nail itself is made of keratin, the same material hair is composed of. -

Update on Lichen Planus and Its Clinical Variants☆
International Journal of Women's Dermatology xxx (2015) xxx–xxx Contents lists available at ScienceDirect International Journal of Women's Dermatology Update on lichen planus and its clinical variants☆ Gillian Weston, MSIII a,⁎, Michael Payette, MD, MBA b a University of Connecticut School of Medicine, Farmington, CT b Department of Dermatology, University of Connecticut Health Center, Farmington, CT article info abstract Article history: Lichen planus (LP) is an inflammatory skin condition with characteristic clinical and histopathological findings. Received 8 December 2014 Classic LP typically presents as pruritic, polygonal, violaceous flat-topped papules and plaques; many variants Received in revised form 2 April 2015 in morphology and location also exist, including oral, nail, linear, annular, atrophic, hypertrophic, inverse, erup- Accepted 6 April 2015 tive, bullous, ulcerative, lichen planus pigmentosus, lichen planopilaris, vulvovaginal, actinic, lichen planus-lupus Available online xxxx erythematosus overlap syndrome, and lichen planus pemphigoides. Clinical presentation of the rarer variant le- fi Keywords: sions may be largely dissimilar to classic LP and therefore dif cult to diagnose based solely on clinical examina- lichen tion. However, histopathological examination of LP and LP-variant lesions reveal similar features, aiding in the planus proper diagnosis of the disease. Management of LP and LP variants aims to control symptoms and to decrease lichenoid time from onset to resolution; it often involves topical corticosteroids, but varies depending on the severity LP and location of the lesion. The literature contains an array of reports on the variations in presentation and suc- planopilaris cessful management of LP and its variants. A familiarity with LP and its variants is important in achieving timely variants recognition and management of the disease. -

B K B Ld I MD Brooke Baldwin, MD Private Practice, Lutz, Florida Chief
BBkrooke BBldialdwin, MD Private Practice, Lutz, Florida Chief of Dermatology James A Haley VA Hospital Adjunct Assistant Professor of Dermatology University of Florida What we are going to cover today Dermatologic Emergencies Common benign skin growths Malignant skin tumors Common Rashes Photoprotecti on and CiCosmetics Dermatologic Emergencies Erythroderma PlPustular psoriiiasis Pemphigus DRESS Syndrome SJS / TEN EEthdrythroderma Erythroderma Generalized redness and scaling of skin involving >90% BSA Systemic manifestations PihPeripheral edema & ffilacial edema Tachycardia Loss of fluids and proteins Disturbed thermoregulation Most common etiologies Atopic dermatitis, psoriasis, CTCL, drug reactions Despite intensive evaluation, the cause remains unknown in 25‐30% PPlustular psoriiiasis Pustular Psoriasis Generalized pustular psoriasis Unusual mani festation o f psoriasis Triggering factors Pregnancy (impetigo herpetiformis) Tapering of corticosteroids (Von Zumbusch reaction) HliHypocalcemia Infections Topical irritants Rarely treatment with TNF alpha blockers (palms and soles) Pemphigus Group of chronic autoimmune blistering diseases presenting with painful erosions IgG Autoantibodies are directed against the cell surface of keratinocytes Results in blistering in varying areas of the epidermis Diagnosi s is confirmed wihith direct iflimmunofluorescence on skin biopsy 3 ma jor forms P. vulgaris, P. foliaceus, paraneoplastic Do not confuse with Bullous pemphigoid which presents with tense bullae Pempgphigus -
56 AAVLD Diagnostic Pathology Slide Session
56th AAVLD Diagnostic Pathology Slide Session American Association of Veterinary Laboratory Diagnosticians San Diego, California Saturday, October 19, 2013 3:30-6:00 PM 56th AAVLD Diagnostic Pathology Slide Seminar 56thAAVLD Diagnostic Pathology Slide Session October 19, 2013 San Diego, California 2013 AAVLD Diagnostic Pathology Slide Seminar Presenters Case # Presenter Species Institution 1 Marcia R. S. Ilha Canine TVDIL-UGA 2 Alison Tucker Swine NCVDLS 3 Scott D. Fitzgerald Raccoon DCPAH-MSU 4 Bailey L. Wilberts Bovine ISU 5 Kelly Hughes Canine OSU-VDL 6 Dodd Sledge Chicken DCPAH-MSU 7 Tuddow Thaiwong Canine DCPAH-MSU 8 Kelli Almes Feline KSVDL-KSU 9 Chanran Ganta Swine KSVDL-KSU 10 Mahogany Caesar Equine NCVDLS 11 Panayiotis Loukopoulos Pacific gopher snake CAHFS-UCDavis 12 Andrew Brooks Canine AHL-UofG 13 Donal O’Toole Canine WSVL-UW 14 Sandra Scholes Bovine AHVLA 15 Leslie W. Woods Pacific fisher CAHFS-UCDavis 16 Francisco A. Uzal Bovine CAHFS-UCDavis 17 Jeffrey R. Hayes Swine Ohio ADDL 18 Tim Cushing Feline CVDC 2 56th AAVLD Diagnostic Pathology Slide Seminar 56thAAVLD Diagnostic Pathology Slide Session October 19, 2013 San Diego, California 2013 AAVLD Diagnostic Pathology Slide Seminar Diagnoses Case # Presenter Species Diagnosis Page # 1 Ilha Canine Extra-adrenal paraganglioma 4 2 Tucker Swine Idiopathic vesicular disease of swine 5 3 Fitzgerald Raccoon Canine distemper and infectious canine hepatitis 6 4 Wilberts Bovine Mannheimiosis and adenoviral infection 7 5 Hughes Canine Canine meningeal polyarteritis 8-9 6 Sledge Chicken