Resident / Humanitarian Coordinator Report on the Use of CERF Funds
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Côte D'ivoire
CÔTE D’IVOIRE COI Compilation August 2017 United Nations High Commissioner for Refugees Regional Representation for West Africa - RSD Unit UNHCR Côte d’Ivoire UNHCR Regional Representation for West Africa - RSD Unit UNHCR Côte d’Ivoire Côte d’Ivoire COI Compilation August 2017 This report collates country of origin information (COI) on Côte d’Ivoire up to 15 August 2017 on issues of relevance in refugee status determination for Ivorian nationals. The report is based on publicly available information, studies and commentaries. It is illustrative, but is neither exhaustive of information available in the public domain nor intended to be a general report on human-rights conditions. The report is not conclusive as to the merits of any individual refugee claim. All sources are cited and fully referenced. Users should refer to the full text of documents cited and assess the credibility, relevance and timeliness of source material with reference to the specific research concerns arising from individual applications. UNHCR Regional Representation for West Africa Immeuble FAALO Almadies, Route du King Fahd Palace Dakar, Senegal - BP 3125 Phone: +221 33 867 62 07 Kora.unhcr.org - www.unhcr.org Table of Contents List of Abbreviations .............................................................................................................. 4 1 General Information ....................................................................................................... 5 1.1 Historical background ............................................................................................ -

Militarized Youths in Western Côte D'ivoire
Militarized youths in Western Côte d’Ivoire - Local processes of mobilization, demobilization, and related humanitarian interventions (2002-2007) Magali Chelpi-den Hamer To cite this version: Magali Chelpi-den Hamer. Militarized youths in Western Côte d’Ivoire - Local processes of mobiliza- tion, demobilization, and related humanitarian interventions (2002-2007). African Studies Centre, 36, 2011, African Studies Collection. hal-01649241 HAL Id: hal-01649241 https://hal-amu.archives-ouvertes.fr/hal-01649241 Submitted on 27 Nov 2017 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. African Studies Centre African Studies Collection, Vol. 36 Militarized youths in Western Côte d’Ivoire Local processes of mobilization, demobilization, and related humanitarian interventions (2002-2007) Magali Chelpi-den Hamer Published by: African Studies Centre P.O. Box 9555 2300 RB Leiden The Netherlands [email protected] www.ascleiden.nl Cover design: Heike Slingerland Cover photo: ‘Market scene, Man’ (December 2007) Photographs: Magali Chelpi-den Hamer Printed by Ipskamp -
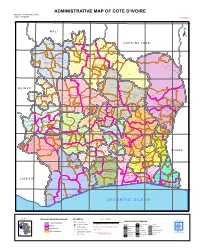
ADMINISTRATIVE MAP of COTE D'ivoire Map Nº: 01-000-June-2005 COTE D'ivoire 2Nd Edition
ADMINISTRATIVE MAP OF COTE D'IVOIRE Map Nº: 01-000-June-2005 COTE D'IVOIRE 2nd Edition 8°0'0"W 7°0'0"W 6°0'0"W 5°0'0"W 4°0'0"W 3°0'0"W 11°0'0"N 11°0'0"N M A L I Papara Débété ! !. Zanasso ! Diamankani ! TENGRELA [! ± San Koronani Kimbirila-Nord ! Toumoukoro Kanakono ! ! ! ! ! !. Ouelli Lomara Ouamélhoro Bolona ! ! Mahandiana-Sokourani Tienko ! ! B U R K I N A F A S O !. Kouban Bougou ! Blésségué ! Sokoro ! Niéllé Tahara Tiogo !. ! ! Katogo Mahalé ! ! ! Solognougo Ouara Diawala Tienny ! Tiorotiérié ! ! !. Kaouara Sananférédougou ! ! Sanhala Sandrégué Nambingué Goulia ! ! ! 10°0'0"N Tindara Minigan !. ! Kaloa !. ! M'Bengué N'dénou !. ! Ouangolodougou 10°0'0"N !. ! Tounvré Baya Fengolo ! ! Poungbé !. Kouto ! Samantiguila Kaniasso Monogo Nakélé ! ! Mamougoula ! !. !. ! Manadoun Kouroumba !.Gbon !.Kasséré Katiali ! ! ! !. Banankoro ! Landiougou Pitiengomon Doropo Dabadougou-Mafélé !. Kolia ! Tougbo Gogo ! Kimbirila Sud Nambonkaha ! ! ! ! Dembasso ! Tiasso DENGUELE REGION ! Samango ! SAVANES REGION ! ! Danoa Ngoloblasso Fononvogo ! Siansoba Taoura ! SODEFEL Varalé ! Nganon ! ! ! Madiani Niofouin Niofouin Gbéléban !. !. Village A Nyamoin !. Dabadougou Sinémentiali ! FERKESSEDOUGOU Téhini ! ! Koni ! Lafokpokaha !. Angai Tiémé ! ! [! Ouango-Fitini ! Lataha !. Village B ! !. Bodonon ! ! Seydougou ODIENNE BOUNDIALI Ponondougou Nangakaha ! ! Sokoro 1 Kokoun [! ! ! M'bengué-Bougou !. ! Séguétiélé ! Nangoukaha Balékaha /" Siempurgo ! ! Village C !. ! ! Koumbala Lingoho ! Bouko Koumbolokoro Nazinékaha Kounzié ! ! KORHOGO Nongotiénékaha Togoniéré ! Sirana -

Cote D'ivoire Summary Full Resettlement Plan (Frp)
AFRICAN DEVELOPMENT BANK GROUP PROJECT : GRID REINFORCEMENT AND RURAL ELECTRIFICATION PROJECT COUNTRY : COTE D’IVOIRE SUMMARY FULL RESETTLEMENT PLAN (FRP) Project Team : Mr. R. KITANDALA, Electrical Engineer, ONEC.1 Mr. P. DJAIGBE, Principal Energy Officer ONEC.1/SNFO Mr. M.L. KINANE, Principal Environmental Specialist ONEC.3 Mr. S. BAIOD, Consulting Environmentalist, ONEC.3 Project Team Sector Director: Mr. A.RUGUMBA, Director, ONEC Regional Director: Mr. A. BERNOUSSI, Acting Director, ORWA Division Manager: Mr. Z. AMADOU, Division Manager, ONEC.1, 1 GRID REIFORCEMENT AND RURAL ELECTRIFICATION PROJECT Summary FRP Project Name : GRID REIFORCEMENT AND RURAL ELECTRIFICATION PROJECT Country : COTE D’IVOIRE Project Number : P-CI-FA0-014 Department : ONEC Division: ONEC 1 INTRODUCTION This document presents the summary Full Resettlement Plan (FRP) of the Grid Reinforcement and Rural Electrification Project. It defines the principles and terms of establishment of indemnification and compensation measures for project affected persons and draws up an estimated budget for its implementation. This plan has identified 543 assets that will be affected by the project, while indicating their socio- economic status, the value of the assets impacted, the terms of compensation, and the institutional responsibilities, with an indicative timetable for its implementation. This entails: (i) compensating owners of land and developed structures, carrying out agricultural or commercial activities, as well as bearing trees and graves, in the road right-of-way for loss of income, at the monetary value replacement cost; and (ii) encouraging, through public consultation, their participation in the plan’s planning and implementation. 1. PROJECT DESCRIPTION AND IMPACT AREA 1.1. Project Description and Rationale The Grid Reinforcement and Rural Electrification Project seeks to strengthen power transmission infrastructure with a view to completing the primary network, ensuring its sustainability and, at the same time, upgrading its available power and maintaining its balance. -

Full-Text (PDF)
Vol. 12(4), pp. 291-304, October-December 2020 DOI: 10.5897/IJBC2020.1430 Article Number: 3BC20E565083 ISSN 2141-243X Copyright © 2020 International Journal of Biodiversity and Author(s) retain the copyright of this article http://www.academicjournals.org/IJBC Conservation Full Length Research Paper Impact of cocoa cultivation in the forest-savannah transition zone of western Côte d'Ivoire Kadio Attey N. Koua*, Kouassi B. Kpangui and Yao Sadaiou S. Barima Laboratory of Biodiversity and Sustainable Management of Tropical Ecosystems, Université Jean Lorougnon Guédé, BP 150 Daloa, Côte d'Ivoire. Received 14 July, 2020 ; Accepted 30 September, 2020 The mountainous relief of Western Region of Côte d'Ivoire, as well as large savannas bordering the dense semi-deciduous forests, did not make this part of the country an area suitable for cocoa cultivation. However, in search of forest land for cocoa cultivation, a large influx of people has been observed in this area over the last decade. The objective of this study is to assess the impact of human pressure due to population migrations for cocoa cultivation on vegetation degradation in the western mountainous region. To achieve this, the methodology consisted of digital processing of a set of three Landsat satellite images from 1985, 2002 and 2018, and interviews with cocoa plantation owners in the study area. The results showed that between 2002 and 2018, the annual rates of forest and savannah loss were 8.6 and 0.7% respectively. This loss is to the benefit of new cocoa farms, which are increasing annually by 12.6%. Also, the period 2002 to 2018 corresponds to the period of strong migration of producers in the zone with a settlement rate of 85.5%. -

République De Cote D'ivoire
R é p u b l i q u e d e C o t e d ' I v o i r e REPUBLIQUE DE COTE D'IVOIRE C a r t e A d m i n i s t r a t i v e Carte N° ADM0001 AFRIQUE OCHA-CI 8°0'0"W 7°0'0"W 6°0'0"W 5°0'0"W 4°0'0"W 3°0'0"W Débété Papara MALI (! Zanasso Diamankani TENGRELA ! BURKINA FASO San Toumoukoro Koronani Kanakono Ouelli (! Kimbirila-Nord Lomara Ouamélhoro Bolona Mahandiana-Sokourani Tienko (! Bougou Sokoro Blésségu é Niéllé (! Tiogo Tahara Katogo Solo gnougo Mahalé Diawala Ouara (! Tiorotiérié Kaouara Tienn y Sandrégué Sanan férédougou Sanhala Nambingué Goulia N ! Tindara N " ( Kalo a " 0 0 ' M'Bengué ' Minigan ! 0 ( 0 ° (! ° 0 N'd énou 0 1 Ouangolodougou 1 SAVANES (! Fengolo Tounvré Baya Kouto Poungb é (! Nakélé Gbon Kasséré SamantiguilaKaniasso Mo nogo (! (! Mamo ugoula (! (! Banankoro Katiali Doropo Manadoun Kouroumba (! Landiougou Kolia (! Pitiengomon Tougbo Gogo Nambonkaha Dabadougou-Mafélé Tiasso Kimbirila Sud Dembasso Ngoloblasso Nganon Danoa Samango Fononvogo Varalé DENGUELE Taoura SODEFEL Siansoba Niofouin Madiani (! Téhini Nyamoin (! (! Koni Sinémentiali FERKESSEDOUGOU Angai Gbéléban Dabadougou (! ! Lafokpokaha Ouango-Fitini (! Bodonon Lataha Nangakaha Tiémé Villag e BSokoro 1 (! BOUNDIALI Ponond ougou Siemp urgo Koumbala ! M'b engué-Bougou (! Seydougou ODIENNE Kokoun Séguétiélé Balékaha (! Villag e C ! Nangou kaha Togoniéré Bouko Kounzié Lingoho Koumbolokoro KORHOGO Nongotiénékaha Koulokaha Pign on ! Nazinékaha Sikolo Diogo Sirana Ouazomon Noguirdo uo Panzaran i Foro Dokaha Pouan Loyérikaha Karakoro Kagbolodougou Odia Dasso ungboho (! Séguélon Tioroniaradougou -

Côte D'ivoire
AFRICAN DEVELOPMENT FUND PROJECT COMPLETION REPORT HOSPITAL INFRASTRUCTURE REHABILITATION AND BASIC HEALTHCARE SUPPORT REPUBLIC OF COTE D’IVOIRE COUNTRY DEPARTMENT OCDW WEST REGION MARCH-APRIL 2000 SCCD : N.G. TABLE OF CONTENTS Page CURRENCY EQUIVALENTS, WEIGHTS AND MEASUREMENTS ACRONYMS AND ABBREVIATIONS, LIST OF ANNEXES, SUMMARY, CONCLUSION AND RECOMMENDATIONS BASIC DATA AND PROJECT MATRIX i to xii 1 INTRODUCTION 1 2 PROJECT OBJECTIVES AND DESIGN 1 2.1 Project Objectives 1 2.2 Project Description 2 2.3 Project Design 3 3. PROJECT IMPLEMENTATION 3 3.1 Entry into Force and Start-up 3 3.2 Modifications 3 3.3 Implementation Schedule 5 3.4 Quarterly Reports and Accounts Audit 5 3.5 Procurement of Goods and Services 5 3.6 Costs, Sources of Finance and Disbursements 6 4 PROJECT PERFORMANCE AND RESULTS 7 4.1 Operational Performance 7 4.2 Institutional Performance 9 4.3 Performance of Consultants, Contractors and Suppliers 10 5 SOCIAL AND ENVIRONMENTAL IMPACT 11 5.1 Social Impact 11 5.2 Environmental Impact 12 6. SUSTAINABILITY 12 6.1 Infrastructure 12 6.2 Equipment Maintenance 12 6.3 Cost Recovery 12 6.4 Health Staff 12 7. BANK’S AND BORROWER’S PERFORMANCE 13 7.1 Bank’s Performance 13 7.2 Borrower’s Performance 13 8. OVERALL PERFORMANCE AND RATING 13 9. CONCLUSIONS, LESSONS AND RECOMMENDATIONS 13 9.1 Conclusions 13 9.2 Lessons 14 9.3 Recommendations 14 Mrs. B. BA (Public Health Expert) and a Consulting Architect prepared this report following their project completion mission in the Republic of Cote d’Ivoire on March-April 2000. -

Scoping Mission Catalyzing Women's Entrepreneurship in Côte D'ivoire
Scoping Mission Catalyzing Women’s Entrepreneurship in Côte d'Ivoire Commissioned by the Netherlands Enterprise Agency Scoping Mission Catalyzing Women’s Entrepreneurship in Côte d'Ivoire Commissioned By: The Dutch Ministry of Foreign Affairs and Netherlands Enterprise Agency (April - October 2020) Research Team: Beatrice Maneshi - Lead Investigator Judith vollebregt- Supporting Investigator Ismael Soumahoro- Lead Local Investigator Benjamin N'Dri- Supporting Local Investigator 1 Catalyzing Women’s Entrepreneurship in Côte d'Ivoire- Scoping Study (Fall 2020) Table of Contents 1. Definitions 4 Acronyms 5 2. Executive Summary 6 3. Objectives 7 4. Methodologies 8 Team Composition and Collaborative Efforts 10 Limitations: 10 5. Overall Findings 12 6. Overview 14 Economy & Politics 14 Women's Roles in Society 16 The Rural vs. Urban Divide 17 Women in Rural Settings 18 Women in Urban Settings 19 7. Legal Statutes and Government Policies 22 Women, Business, and the Law 22 The Issues around Statutory Law vs. Customary Law 23 Entrepreneurship Regulations 23 8. Women’s Entrepreneurship Culture 27 Abidjan 28 Korhogo 29 San Pedro 31 Odienné 32 Bouaké/Yamoussoukro 33 Man 34 9. Access to Finance 36 Overview 36 Cooperative Finance Models 37 Micro-Finance 37 Venture Capital & Angel Investors 38 Traditional Banks 40 10. Women’s Access to and Use of Education for Business 44 Primary Education 44 Higher Education 45 2 Catalyzing Women’s Entrepreneurship in Côte d'Ivoire- Scoping Study (Fall 2020) Incubators and Accelerators 46 Co-working Spaces 48 NGOs Focused on Women and Business 49 Corporate Social Responsibility 52 11. Entrepreneurship Ecosystem and Access for Women 53 Trends 53 Professional Associations 54 Legal Aid and Support 55 12. -

Document of the World Bank
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: PAD1671 INTERNATIONAL DEVELOPMENT ASSOCIATION PROJECT PAPER ON A Public Disclosure Authorized PROPOSED ADDITIONAL CREDIT IN THE AMOUNT OF EUR 53.9 MILLION (US$60 MILLION EQUIVALENT) AND PROPOSED RESTRUCTURING TO THE REPUBLIC OF CÔTE D’IVOIRE FOR THE Public Disclosure Authorized INFRASTRUCTURE RENEWAL AND URBAN MANAGEMENT PROJECT (FORMERLY EMERGENCY INFRASTRUCTURE RENEWAL PROJECT) July 7, 2016 Social, Urban, Rural and Resilience Global Practice Africa Region Public Disclosure Authorized This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective – May 31, 2016) Currency Unit = FCFA FCFA 588 = US$1 1 USD = EUR 0.89670014 FISCAL YEAR January 1 – December 31 ABBREVIATIONS AND ACRONYMS AF Additional Financing AGEROUTE Ivorian Road Agency (Agence de Gestion des Routes) CBA Cost-Benefit Analysis CDP Performance-based City Contract (contrat de performance) CERC Contingent Emergency Response Component CI-Energie Côte d’Ivoire Energy Company (Société des Energies de Côte d’Ivoire) CIP Communal Investment Program CMP Communal Maintenance Program CMSP Communal Management Support Program CPF Country Partnership Framework DCM Directorate of Construction and Maintenance (Direction de la Construction et de la Maintenance) DCPP Directorate of Accounting and Parapublic Accounting -
Project: Air Cote D'ivoire Modernization & Expansion Program Country
AFRICAN DEVELOPMENT BANK GROUP zed Public Disclosire Authori PROJECT: AIR COTE D’IVOIRE MODERNIZATION & EXPANSION PROGRAM COUNTRY: COTE D’IVOIRE PROJECT APPRAISAL REPORT Public Dsclosure Authorized PICU DEPARTMENT October 2017 TABLE OF CONTENTS 1. STRATEGIC THRUST AND RATIONALE OF THE PROJECT............................................. 1 1.1 Project Linkages with Country Strategy and Objectives ..........................................................................1 1.2 Rationale for the Bank’s Involvement ......................................................................................................1 1.3 Donor Coordination ..................................................................................................................................3 2. PROJECT DESCRIPTION ............................................................................................................ 4 2.1 Project Objectives and Components .........................................................................................................4 2.2 Technical Solution Retained and Alternative Solutions Considered ........................................................5 2.3 Project Type..............................................................................................................................................6 2.4 Project Cost Estimate and Financing Mechanisms ...................................................................................7 2.5 Project Area and Beneficiaries .................................................................................................................9 -

African Development Bank Cote D'ivoire
AFRICAN DEVELOPMENT BANK Public Disclosure Authorized Public Disclosure COTE D’IVOIRE POWER TRANSMISSION AND DISTRIBUTION NETWORKS REINFORCEMENT PROJECT (PRETD) APPRAISAL REPORT Public Disclosure Authorized Public Disclosure ONEC DEPARTMENT November 2016 Translated Document TABLE OF CONTENTS PROJECT OVERVIEW ......................................................................................................................... ii I. IPROJECT PRESENTATION, ALIGNMENT AND BENEFICIARIES ..................................... 1 A. Project Context, Development Objectives and Specific Objectives ....................................... 1 B. Expected Project Outcomes and Impacts ............................................................................... 1 C. Project Outputs ....................................................................................................................... 2 D. Project Rationale..................................................................................................................... 2 E. Project’s Alignment with National Development Goals ........................................................ 2 F. Project Alignment on Bank Strategies and Policies ............................................................... 3 G. Integration of Requirements Set Out Under Presidential Directive No. 02/2005 ................... 3 H. Consultation Process and Ownership by the Country ............................................................ 3 I. Project Target Areas, Beneficiaries and Selection Criteria ....................................................... -
Statistiques De GUEMON
AVANT-PROPOS AVANT- PROPOS La publication des données statistiques contribue au pilotage du système éducatif. Elle participe à la planification des besoins recensés au niveau du Ministère de l’Education Nationale, de l’Enseignement Technique et de la Formation Professionnelle sur l’ensemble du territoire National. A cet effet, la Direction des Stratégies, de la Planification et des Statistiques (DSPS) publie, tous les ans, les statistiques scolaires par degré d’enseignement (Préscolaire, Primaire, Secondaire général et technique). Compte tenu de l’importance des données statistiques scolaires, la DSPS, après la publication du document « Statistiques Scolaires de Poche » publié au niveau national, a jugé nécessaire de proposer aux usagers, le même type de document au niveau de chaque région administrative. Ce document comportant les informations sur l’éducation est le miroir expressif de la réalité du système éducatif régional. La possibilité pour tous les acteurs et partenaires de l’école ivoirienne de pouvoir disposer, en tout temps et en tout lieu, des chiffres et indicateurs présentant une vision d’ensemble du système éducatif d’une région donnée, constitue en soi une valeur ajoutée. La DSPS est résolue à poursuivre la production des statistiques scolaires de poche nationales et régionales de façon régulière pour aider les acteurs et partenaires du système éducatif dans les prises de décisions adéquates et surtout dans ce contexte de crise sanitaire liée à la COVID-19. DRENET DUEKOUE : Statistiques scolaires de poche 2019-2020: Région du Guemon 2 PRESENTATION La Direction des Stratégies, de la Planification et des Statistiques (DSPS) est heureuse de mettre à la disposition de la communauté éducative les statistiques scolaires de poche 2019- 2020 de la Région.