Infections Due to Rare Cryptococcus Species. a Literature Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cryptococcus Neoformans</Em>
Clemson University TigerPrints All Dissertations Dissertations December 2019 Role of Cryptococcus neoformans Pyruvate Decarboxylase and Aldehyde Dehydrogenase Enzymes in Acetate Production and Virulence Mufida Ahmed Nagi Ammar Clemson University, [email protected] Follow this and additional works at: https://tigerprints.clemson.edu/all_dissertations Recommended Citation Ammar, Mufida Ahmed Nagi, "Role of Cryptococcus neoformans Pyruvate Decarboxylase and Aldehyde Dehydrogenase Enzymes in Acetate Production and Virulence" (2019). All Dissertations. 2488. https://tigerprints.clemson.edu/all_dissertations/2488 This Dissertation is brought to you for free and open access by the Dissertations at TigerPrints. It has been accepted for inclusion in All Dissertations by an authorized administrator of TigerPrints. For more information, please contact [email protected]. Role of Cryptococcus neoformans Pyruvate Decarboxylase and Aldehyde Dehydrogenase Enzymes in Acetate Production and Virulence A Dissertation Presented to the Graduate School of Clemson University In Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy Biochemistry and Molecular Biology by Mufida Ahmed Nagi Ammar December 2019 Accepted by: Dr. Kerry Smith, Committee Chair Dr. Julia Frugoli Dr. Cheryl Ingram-Smith Dr. Lukasz Kozubowski ABSTRACT The basidiomycete Cryptococcus neoformans is is an invasive opportunistic pathogen of the central nervous system and the most frequent cause of fungal meningitis. C. neoformans enters the host by inhalation and protects itself from immune assault in the lungs by producing hydrolytic enzymes, immunosuppressants, and other virulence factors. C. neoformans also adapts to the environment inside the host, including producing metabolites that may confer survival advantages. One of these, acetate, can be kept in reserve as a carbon source or can be used to weaken the immune response by lowering local pH or as a key part of immunomodulatory molecules. -

Idiopathic CD4 Lymphocytopenia: Spectrum of Opportunistic Infections, Malignancies, and Autoimmune Diseases
Published online: 2021-08-09 REVIEW ARTICLE Idiopathic CD4 Lymphocytopenia: Spectrum of opportunistic infections, malignancies, and autoimmune diseases Dina S. Ahmad, Mohammad Esmadi, William C. Steinmann Department of Internal Medicine, University of Missouri School of Medicine, Columbia, MO, USA Access this article online ABSTRACT Website: www.avicennajmed.com DOI: 10.4103/2231-0770.114121 Idiopathic CD4 lymphocytopenia (ICL) was first defined in 1992 by the US Centers for Disease Quick Response Code: Control and Prevention (CDC) as the repeated presence of a CD4+ T lymphocyte count of fewer than 300 cells per cubic millimeter or of less than 20% of total T cells with no evidence of human immunodeficiency virus (HIV) infection and no condition that might cause depressed CD4 counts. Most of our knowledge about ICL comes from scattered case reports. The aim of this study was to collect comprehensive data from the previously published cases to understand the characteristics of this rare condition. We searched the PubMed database and Science Direct for case reports since 1989 for Idiopathic CD4 lymphocytopenia cases. We found 258 cases diagnosed with ICL in 143 published papers. We collected data about age, sex, pathogens, site of infections, CD4 count, CD8 count, CD4:CD8 ratio, presence of HIV risk factors, malignancies, autoimmune diseases and whether the patients survived or died. The mean age at diagnosis of first opportunistic infection (or ICL if no opportunistic infection reported) was 40.7 ± 19.2 years (standard deviation), with a range of 1 to 85. One-sixty (62%) patients were males, 91 (35.2%) were females, and 7 (2.7%) patients were not identified whether males or females. -

153.Full.Pdf
Copyright Ó 2010 by the Genetics Society of America DOI: 10.1534/genetics.109.113027 A Tetrad Analysis of the Basidiomycete Fungus Cryptococcus neoformans Alexander Idnurm Division of Cell Biology and Biophysics, School of Biological Sciences, University of Missouri-Kansas City, Kansas City, Missouri 64110 Manuscript received December 10, 2009 Accepted for publication February 9, 2010 ABSTRACT Cryptococcus neoformans is a basidiomycete fungus that is found worldwide and causes disease in humans and animal species. The fungus grows asexually as a budding yeast. Under laboratory conditions it is capable of sexual reproduction between two mating types. After cell fusion a dikaryotic filament develops, at the tip of which a basidium gives rise to four chains of basidiospores. Because the chains each comprise 10–30 spores, rather than single spores, the analysis of individual meiotic events has not been attempted in C. neoformans in the style of tetrad analyses performed in other fungal species. Here, the basidiospores from .100 basidia were micromanipulated and the resultant .2500 progeny analyzed for three genetic markers to understand the sexual process in this fungus, leading to four observations: (i) Marker seg- regation provides genetic evidence for a single meiotic event within the basidium followed by multiple rounds of mitosis. (ii) Using each basidium as an unordered tetrad, the ADE2 and URA5 genes are linked to their centromeres, consistent with adjacent genomic regions rich in repetitive elements predicted to comprise Cryptococcus centromeres. (iii) Lack of germination of basidiospores is attributed to aneuploidy, rather than dormancy. (iv) Analysis of basidiospores derived from single chains demonstrates that each chain can contain different genotypes. -

Organismic Interactions
Poster Category 4: Organismic Interactions PR4.1 Co‐cultivations of fungi: microscopic analysis and influence on protein production Isabelle Benoit[1,2] Arman Vinck[1] Jerre van Veluw[1] Han A.B. Wösten[1] Ronald P. de Vries[2] 1Utrecht University 2CBS‐KNAW During their natural life cycle most fungi encounter other microorganisms and live in mixed communities with complex interactions, such as symbiosis or competition. Industrial fermentations, on purpose or by accident, can also result in mixed cultures. Fungal co‐cultivations have been previously described for the production of specific enzymes, however, little is known about the interactions between two species that are grown together. A. niger and A. oryzae are two of the most important industrial fungi worldwide and both have a long history of strain improvement to optimize enzyme and metabolite production. Co‐cultivation of these two Aspergilli with each other and with the ascomycete phytopathogen Magnaporthe grisea, and the basidiomycete white rot fungus Phanerochaete chrysosporium, has recently been described by our group (Hu et al, 2010). Total secreted protein, enzymatic activities related to plant biomass degradation and growth phenotype were analyzed from cultures on wheat bran demonstrating positive effects of the co‐cultivation compared to the individual cultivations. In a follow‐up study the morphology and mechanism of the interaction is addressed using microscopy and proteomics. Data from this study will be presented. Reference Hu et al. International Biodeterioration & Biodegradation 65 (2011) PR4.2 A novel effector secreted by the anthracnose pathogen Colletotrichum truncatum is required for the transition from biotrophy to necrotrophy in fungal pathogens Vijai Bhadauria[1] Sabine Banniza[1] Vandenberg Albert[1] Selvaraj Gopalan[2] Wei Yangdou[3] 1. -

Product Sheet Info
Product Information Sheet for NR-50430 Cryptococcus gattii, Strain C10 Propagation: 1. Keep vial frozen until ready for use; thaw rapidly. Catalog No. NR-50430 2. Inoculate an agar plate with approximately 50 µL of thawed culture and/or transfer the entire thawed aliquot into a single tube of broth For research use only. Not for human use. 3. Incubate the plate and/or tube at 25°C for 2 to 4 days. Contributor: Citation: Brian Wong, M.D., Professor, and Igor Bruzual, Ph.D., Acknowledgment for publications should read “The following Infectious Disease Division, Department of Medicine, Oregon reagent was obtained through BEI Resources, NIAID, NIH: Health and Science University, Portland, Oregon, USA Cryptococcus gattii, Strain C10, NR-50430.” Manufacturer: Biosafety Level: 2 BEI Resources Appropriate safety procedures should always be used with this material. Laboratory safety is discussed in the following Product Description: publication: U.S. Department of Health and Human Services, Classification: Tremellaceae, Cryptococcus Public Health Service, Centers for Disease Control and Species: Cryptococcus gattii Prevention, and National Institutes of Health. Biosafety in Strain: C10 Microbiological and Biomedical Laboratories. 5th ed. Original Source: Cryptococcus gattii (C. gattii), strain C10 Washington, DC: U.S. Government Printing Office, 2009; see was isolated from an unknown human source in the Pacific www.cdc.gov/biosafety/publications/bmbl5/index.htm. Northwest region of North America.1 Comments: C. gattii, strain C10 was deposited as lineage Disclaimers: VGIIa and resistant to azoles.1 You are authorized to use this product for research use only. The Cryptococcus species complex is comprised of four It is not intended for human use. -

University of California Santa Cruz Responding to An
UNIVERSITY OF CALIFORNIA SANTA CRUZ RESPONDING TO AN EMERGENT PLANT PEST-PATHOGEN COMPLEX ACROSS SOCIAL-ECOLOGICAL SCALES A dissertation submitted in partial satisfaction of the requirements for the degree of DOCTOR OF PHILOSOPHY in ENVIRONMENTAL STUDIES with an emphasis in ECOLOGY AND EVOLUTIONARY BIOLOGY by Shannon Colleen Lynch December 2020 The Dissertation of Shannon Colleen Lynch is approved: Professor Gregory S. Gilbert, chair Professor Stacy M. Philpott Professor Andrew Szasz Professor Ingrid M. Parker Quentin Williams Acting Vice Provost and Dean of Graduate Studies Copyright © by Shannon Colleen Lynch 2020 TABLE OF CONTENTS List of Tables iv List of Figures vii Abstract x Dedication xiii Acknowledgements xiv Chapter 1 – Introduction 1 References 10 Chapter 2 – Host Evolutionary Relationships Explain 12 Tree Mortality Caused by a Generalist Pest– Pathogen Complex References 38 Chapter 3 – Microbiome Variation Across a 66 Phylogeographic Range of Tree Hosts Affected by an Emergent Pest–Pathogen Complex References 110 Chapter 4 – On Collaborative Governance: Building Consensus on 180 Priorities to Manage Invasive Species Through Collective Action References 243 iii LIST OF TABLES Chapter 2 Table I Insect vectors and corresponding fungal pathogens causing 47 Fusarium dieback on tree hosts in California, Israel, and South Africa. Table II Phylogenetic signal for each host type measured by D statistic. 48 Table SI Native range and infested distribution of tree and shrub FD- 49 ISHB host species. Chapter 3 Table I Study site attributes. 124 Table II Mean and median richness of microbiota in wood samples 128 collected from FD-ISHB host trees. Table III Fungal endophyte-Fusarium in vitro interaction outcomes. -

Diversity of the Cryptococcus Neoformans-Cryptococcus Gattii Species Complex Marjan Bovers1, Ferry Hagen1 and Teun Boekhout1,2
S4 Rev Iberoam Micol 2008; 25: S4-S12 Review Diversity of the Cryptococcus neoformans-Cryptococcus gattii species complex Marjan Bovers1, Ferry Hagen1 and Teun Boekhout1,2 1Yeast Research Group, CBS Fungal Diversity Centre, Uppsalalaan 8, 3584 CT Utrecht, The Netherlands; 2Department of Internal Medicine and Infectious Diseases, University Medical Centre Utrecht, The Netherlands Summary More than 110 years of study of the Cryptococcus neoformans and Cryptococcus gattii species complex has resulted in an enormous accumulation of fundamental, applied biological and clinical knowledge. Recent developments in our understanding of the diversity within the species complex are presented, emphasizing the intraspecific complexity, which includes species, microspecies, hybrids, serotypes and genotypes. Each of these may have different roles in disease. An overview of obsolete and current names is presented. Key words Cryptococcus neoformans, Cryptococcus gattii, Yeast, Taxonomy, Pathogen. Diversidad del complejo de especies Cryptococcus neoformans-Cryptococcus gattii Resumen Más de 110 años de estudio sobre el complejo de especies Cryptococcus neoformans y Cryptococcus gattii han dado lugar a un gran acúmulo de conocimiento básico, aplicado y clínico. En este artículo se describen los avances recientes en la comprensión de su diversidad, haciendo énfasis en la complejidad intraespecífica que presenta y que llega a englobar especies, microespecies, híbridos, serotipos y genotipos. Cada uno de estos grupos puede jugar un papel diferente en la enfermedad. Se presenta también una visión global de los nombres obsoletos y actuales de estos taxones. Palabras clave Cryptococcus neoformans, Cryptococcus gattii, Levaduras, Patógeno, Taxonomía. Introduction racteristics of the genus Saccharomyces were not present, he placed these species in the genus Cryptococcus [166]. -
Cryptococcus Gattii Outbreak
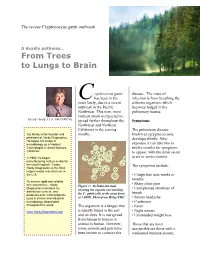
The recent Cryptococcus gattii outbreak A deadly pathway… From Trees to Lungs to Brain ryptococcus gattii disease. The route of C has been in the infection is from breathing the news lately, due to a recent airborne organism, which outbreak in the Pacific becomes lodged in the Northwest. This new, more pulmonary tissues. virulent strain is expected to by Jay Hardy, CLS, SM (NRCM) spread further throughout the Symptoms Northwest and Northern California in the coming The pulmonary disease, Jay Hardy is the founder and months. known as cpryptococcosis, president of Hardy Diagnostics. develops slowly. After He began his career in exposure it can take two to microbiology as a Medical Technologist in Santa Barbara, twelve months for symptoms California. to appear, with the usual onset In 1980, he began at six or seven months. manufacturing culture media for the local hospitals. Today, The symptoms include: Hardy Diagnostics is the third largest media manufacturer in the U.S. • Cough that lasts weeks or months To ensure rapid and reliable turn around time, Hardy • Sharp chest pain Figure 1: An India ink stain Diagnostics maintains six • Unexplained shortness of showing the capsule surrounding distribution centers, and breath produces over 3,000 products the C. gattii cells in the yeast form used in clinical and industrial at 1,000X. Photo from Haley/CDC. • Severe headache microbiology laboratories • Confusion throughout the world. The organism is a fungus that • Fever is usually found in the soil • Night sweats www.HardyDiagnostics.com and on trees. It is not spread • Unintended weight loss from human to human or animal to human. -

Mucormycosis of the Central Nervous System
Journal of Fungi Review Mucormycosis of the Central Nervous System 1 1,2, , 3, , Amanda Chikley , Ronen Ben-Ami * y and Dimitrios P Kontoyiannis * y 1 Infectious Diseases Unit, Tel Aviv Sourasky Medical Center, Tel Aviv 64239, Israel 2 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv 64239, Israel 3 Department of Infectious Diseases, The University of Texas, M.D. Anderson Cancer Center, Houston, TX 77030, USA * Correspondence: [email protected] (R.B.-A.); [email protected] (D.P.K.) These authors contribute equally to this paper. y Received: 6 June 2019; Accepted: 7 July 2019; Published: 8 July 2019 Abstract: Mucormycosis involves the central nervous system by direct extension from infected paranasal sinuses or hematogenous dissemination from the lungs. Incidence rates of this rare disease seem to be rising, with a shift from the rhino-orbital-cerebral syndrome typical of patients with diabetes mellitus and ketoacidosis, to disseminated disease in patients with hematological malignancies. We present our current understanding of the pathobiology, clinical features, and diagnostic and treatment strategies of cerebral mucormycosis. Despite advances in imaging and the availability of novel drugs, cerebral mucormycosis continues to be associated with high rates of death and disability. Emerging molecular diagnostics, advances in experimental systems and the establishment of large patient registries are key components of ongoing efforts to provide a timely diagnosis and effective treatment to patients with cerebral mucormycosis. Keywords: central nervous system; mucormycosis; Mucorales; zygomycosis 1. Introduction Mucormycosis is the second most frequent invasive mold disease after aspergillosis [1–3], with rising incidence reported in some countries [4–7]. -

Fungal Infections – an Overview
REVIEW Fungal infections – An overview Natalie Schellack, BCur, BPharm, PhD(Pharmacy); Jade du Toit, BPharm; Tumelo Mokoena, BPharm; Elmien Bronkhorst, BPharm, MSc(Med) School of Pharmacy, Faculty of Health Sciences, Sefako Makgatho Health Sciences University Correspondence to: Prof Natalie Schellack, [email protected] Abstract Fungi normally originate from the environment that surrounds us, and appear to be harmless until inhaled or ingestion of spores occurs. A pathogenic fungus may lead to infection. People who are at risk of acquiring fungal infection are those living with human immunodeficiency virus (HIV), cancer, receiving immunosuppressant therapy, neonates and those of advanced age. The management of superficial fungal infections is mainly topical, with agents including terbinafine, miconazole and ketoconazole. Oral treatment includes griseofulvin and fluconazole. Invasive fungal infections are difficult to treat, and are managed with agents including the azoles, echinocandins and amphotericin B. This paper provides a general overview of the management of fungus infections. © Medpharm S Afr Pharm J 2019;86(1):33-40 Introduction more advanced biochemical or molecular testing.4 Fungi normally originate from the environment that surrounds Superficial fungal infections us, and appear to be harmless until inhaled or ingestion of spores Either yeasts or fungi can cause dermatomycosis, or superficial occurs. Infection with fungi is also more likely when the body’s fungal infections.7 Fungi that infect the hair, skin, nails and mucosa immune system becomes weakened. A pathogenic fungus may lead to infection. The number of fungus species ranges in the can cause a superficial fungal infection. Dermatophytes are found millions and only a few species seem to be harmful to humans; the naturally in soil, human skin and keratin-containing structures, 3 ones found mostly on the mucous membrane and the skin have which provide them with a source of nutrition. -

Safety Precautions for Working with Cryptococcus Neoformans
Safety Precautions for Working with Cryptococcus neoformans The basidiomycete fungus Cryptococcus neoformans is an invasive opportunistic pathogen of the central nervous system and the most frequent cause of fungal meningitis worldwide. Although Cryptococcus is a problem in the United States, it is significantly more prevalent and especially devastating in the developing world, such as sub-Saharan Africa, resulting in in more than 625,000 deaths per year worldwide. C. neoformans survives in the environment within soil, trees, and bird guano, where it can interact with wild animals or microbial predators, maintaining its virulence. Human infection is thought to be acquired by inhalation of desiccated yeast cells or spores from an environmental source. C. neoformans can colonize the host respiratory tract without producing any disease. Infection is typically asymptomatic, and it can be either cleared or enter a dormant, latent form. When host immunity is compromised, the dormant form can be reactivated and disseminate hematogenously to cause systemic infection. C. neoformans can infect or spread to any organ to cause localized infections involving the skin, eyes, myocardium, bones, joints, lungs, prostate gland, or urinary tract, in addition to its propensity to infect the central nervous systems. The following diseases and medications are risk factors for C. neoformans infection and are associated with at least some degree of immunosuppression: Ø HIV/AIDs (CD4 < 100cells/mm) Ø Corticosteroids or other immunosuppressive medications for cancer, chemotherapy, or organ transplants Ø Solid organ transplantations Ø Diabetes mellitus Ø Heart, lung, or liver disease Ø Pregnancy Even otherwise healthy, fully immunocompetent individuals can develop cryptococcosis, as may well be the case in a lab accident. -

Cryptococcosis in Cats
12 Cryptococcosis in cats FACT SHEET What is cryptococcosis? ! Atypical forms are characterized by one or more skin nodules that are not ! Cryptococcosis is the most common systemic fungal disease in cats worldwide. painful but may be firm or fluctuant. Solitary nodules are suggestive of direct inoculation. ! It is caused by the C. neoformans-C. gattii species complex which can also infect o Multiple nodules are suggestive of haematogenous spread from the primary humans, domestic and wild mammals and birds. o site of infection. ! C. neoformans is considered an opportunistic pathogen in human urban ! populations, whereas C. gattii is a true pathogen, more prevalent in rural areas. Haematogenous dissemination may lead to meningoencephalomyelitis, uveitis, chorioretinitis, osteomyelitis, polyarthritis, systemic lymphadenitis and multi- ! Cryptococcosis is a rare non-contagious fungal disease, acquired from a organ involvement. contaminated environment. ! CNS involvement may occur following local dissemination through the cribriform plate, causing sudden blindness, seizures and/or behavioural changes. ! Apathy and cachexia appear in chronic cases with systemic dissemination. Pathogenesis ! Cryptococcus is mainly an airborne pathogen, and basidiospores, which develop in the environment, penetrate the cat’s respiratory system and induce primary Diagnosis infection. ! Cutaneous inoculation or spread from the respiratory to the central nervous ! Cytology: samples stained with Romanowsky-type stains demonstrate pink to system (CNS) is also possible. violet, round or budding yeasts that vary in size (4-15 microns) and shape. They are typically surrounded by a clear, more or less thick halo corresponding to the ! The yeast cell survives inside phagocytic cells such as macrophages, dendritic unstained capsule. cells, and neutrophils, replicating both extracellularly and intracellularly.