Safety Precautions for Working with Cryptococcus Neoformans
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cryptococcus Neoformans</Em>
Clemson University TigerPrints All Dissertations Dissertations December 2019 Role of Cryptococcus neoformans Pyruvate Decarboxylase and Aldehyde Dehydrogenase Enzymes in Acetate Production and Virulence Mufida Ahmed Nagi Ammar Clemson University, [email protected] Follow this and additional works at: https://tigerprints.clemson.edu/all_dissertations Recommended Citation Ammar, Mufida Ahmed Nagi, "Role of Cryptococcus neoformans Pyruvate Decarboxylase and Aldehyde Dehydrogenase Enzymes in Acetate Production and Virulence" (2019). All Dissertations. 2488. https://tigerprints.clemson.edu/all_dissertations/2488 This Dissertation is brought to you for free and open access by the Dissertations at TigerPrints. It has been accepted for inclusion in All Dissertations by an authorized administrator of TigerPrints. For more information, please contact [email protected]. Role of Cryptococcus neoformans Pyruvate Decarboxylase and Aldehyde Dehydrogenase Enzymes in Acetate Production and Virulence A Dissertation Presented to the Graduate School of Clemson University In Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy Biochemistry and Molecular Biology by Mufida Ahmed Nagi Ammar December 2019 Accepted by: Dr. Kerry Smith, Committee Chair Dr. Julia Frugoli Dr. Cheryl Ingram-Smith Dr. Lukasz Kozubowski ABSTRACT The basidiomycete Cryptococcus neoformans is is an invasive opportunistic pathogen of the central nervous system and the most frequent cause of fungal meningitis. C. neoformans enters the host by inhalation and protects itself from immune assault in the lungs by producing hydrolytic enzymes, immunosuppressants, and other virulence factors. C. neoformans also adapts to the environment inside the host, including producing metabolites that may confer survival advantages. One of these, acetate, can be kept in reserve as a carbon source or can be used to weaken the immune response by lowering local pH or as a key part of immunomodulatory molecules. -

Idiopathic CD4 Lymphocytopenia: Spectrum of Opportunistic Infections, Malignancies, and Autoimmune Diseases
Published online: 2021-08-09 REVIEW ARTICLE Idiopathic CD4 Lymphocytopenia: Spectrum of opportunistic infections, malignancies, and autoimmune diseases Dina S. Ahmad, Mohammad Esmadi, William C. Steinmann Department of Internal Medicine, University of Missouri School of Medicine, Columbia, MO, USA Access this article online ABSTRACT Website: www.avicennajmed.com DOI: 10.4103/2231-0770.114121 Idiopathic CD4 lymphocytopenia (ICL) was first defined in 1992 by the US Centers for Disease Quick Response Code: Control and Prevention (CDC) as the repeated presence of a CD4+ T lymphocyte count of fewer than 300 cells per cubic millimeter or of less than 20% of total T cells with no evidence of human immunodeficiency virus (HIV) infection and no condition that might cause depressed CD4 counts. Most of our knowledge about ICL comes from scattered case reports. The aim of this study was to collect comprehensive data from the previously published cases to understand the characteristics of this rare condition. We searched the PubMed database and Science Direct for case reports since 1989 for Idiopathic CD4 lymphocytopenia cases. We found 258 cases diagnosed with ICL in 143 published papers. We collected data about age, sex, pathogens, site of infections, CD4 count, CD8 count, CD4:CD8 ratio, presence of HIV risk factors, malignancies, autoimmune diseases and whether the patients survived or died. The mean age at diagnosis of first opportunistic infection (or ICL if no opportunistic infection reported) was 40.7 ± 19.2 years (standard deviation), with a range of 1 to 85. One-sixty (62%) patients were males, 91 (35.2%) were females, and 7 (2.7%) patients were not identified whether males or females. -

153.Full.Pdf
Copyright Ó 2010 by the Genetics Society of America DOI: 10.1534/genetics.109.113027 A Tetrad Analysis of the Basidiomycete Fungus Cryptococcus neoformans Alexander Idnurm Division of Cell Biology and Biophysics, School of Biological Sciences, University of Missouri-Kansas City, Kansas City, Missouri 64110 Manuscript received December 10, 2009 Accepted for publication February 9, 2010 ABSTRACT Cryptococcus neoformans is a basidiomycete fungus that is found worldwide and causes disease in humans and animal species. The fungus grows asexually as a budding yeast. Under laboratory conditions it is capable of sexual reproduction between two mating types. After cell fusion a dikaryotic filament develops, at the tip of which a basidium gives rise to four chains of basidiospores. Because the chains each comprise 10–30 spores, rather than single spores, the analysis of individual meiotic events has not been attempted in C. neoformans in the style of tetrad analyses performed in other fungal species. Here, the basidiospores from .100 basidia were micromanipulated and the resultant .2500 progeny analyzed for three genetic markers to understand the sexual process in this fungus, leading to four observations: (i) Marker seg- regation provides genetic evidence for a single meiotic event within the basidium followed by multiple rounds of mitosis. (ii) Using each basidium as an unordered tetrad, the ADE2 and URA5 genes are linked to their centromeres, consistent with adjacent genomic regions rich in repetitive elements predicted to comprise Cryptococcus centromeres. (iii) Lack of germination of basidiospores is attributed to aneuploidy, rather than dormancy. (iv) Analysis of basidiospores derived from single chains demonstrates that each chain can contain different genotypes. -

Product Sheet Info
Product Information Sheet for NR-50430 Cryptococcus gattii, Strain C10 Propagation: 1. Keep vial frozen until ready for use; thaw rapidly. Catalog No. NR-50430 2. Inoculate an agar plate with approximately 50 µL of thawed culture and/or transfer the entire thawed aliquot into a single tube of broth For research use only. Not for human use. 3. Incubate the plate and/or tube at 25°C for 2 to 4 days. Contributor: Citation: Brian Wong, M.D., Professor, and Igor Bruzual, Ph.D., Acknowledgment for publications should read “The following Infectious Disease Division, Department of Medicine, Oregon reagent was obtained through BEI Resources, NIAID, NIH: Health and Science University, Portland, Oregon, USA Cryptococcus gattii, Strain C10, NR-50430.” Manufacturer: Biosafety Level: 2 BEI Resources Appropriate safety procedures should always be used with this material. Laboratory safety is discussed in the following Product Description: publication: U.S. Department of Health and Human Services, Classification: Tremellaceae, Cryptococcus Public Health Service, Centers for Disease Control and Species: Cryptococcus gattii Prevention, and National Institutes of Health. Biosafety in Strain: C10 Microbiological and Biomedical Laboratories. 5th ed. Original Source: Cryptococcus gattii (C. gattii), strain C10 Washington, DC: U.S. Government Printing Office, 2009; see was isolated from an unknown human source in the Pacific www.cdc.gov/biosafety/publications/bmbl5/index.htm. Northwest region of North America.1 Comments: C. gattii, strain C10 was deposited as lineage Disclaimers: VGIIa and resistant to azoles.1 You are authorized to use this product for research use only. The Cryptococcus species complex is comprised of four It is not intended for human use. -
Cryptococcus Gattii Outbreak
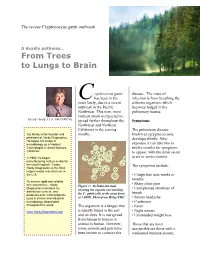
The recent Cryptococcus gattii outbreak A deadly pathway… From Trees to Lungs to Brain ryptococcus gattii disease. The route of C has been in the infection is from breathing the news lately, due to a recent airborne organism, which outbreak in the Pacific becomes lodged in the Northwest. This new, more pulmonary tissues. virulent strain is expected to by Jay Hardy, CLS, SM (NRCM) spread further throughout the Symptoms Northwest and Northern California in the coming The pulmonary disease, Jay Hardy is the founder and months. known as cpryptococcosis, president of Hardy Diagnostics. develops slowly. After He began his career in exposure it can take two to microbiology as a Medical Technologist in Santa Barbara, twelve months for symptoms California. to appear, with the usual onset In 1980, he began at six or seven months. manufacturing culture media for the local hospitals. Today, The symptoms include: Hardy Diagnostics is the third largest media manufacturer in the U.S. • Cough that lasts weeks or months To ensure rapid and reliable turn around time, Hardy • Sharp chest pain Figure 1: An India ink stain Diagnostics maintains six • Unexplained shortness of showing the capsule surrounding distribution centers, and breath produces over 3,000 products the C. gattii cells in the yeast form used in clinical and industrial at 1,000X. Photo from Haley/CDC. • Severe headache microbiology laboratories • Confusion throughout the world. The organism is a fungus that • Fever is usually found in the soil • Night sweats www.HardyDiagnostics.com and on trees. It is not spread • Unintended weight loss from human to human or animal to human. -

Idiopathic CD4 Lymphocytopenia Presenting As Refractory Cryptococcal Meningitis
Case Report Idiopathic CD4 lymphocytopenia presenting as refractory cryptococcal meningitis A. Sharma, V. Lal, M. Modi, D. Khurana, S. Bal, S. Prabhakar Department of Neurology, Postgraduate Institute of Medical Education and Research, Chandigarh-160 012, India Abstract Idiopathic CD4 T-lymphocytopenia (ICL) is a syndrome characterized by depletion of CD4 T-cells without evidence of human immunodeficiency virus (HIV) infection. There are a few reported cases of ICL associated with different diseases and clinical conditions, most commonly the opportunistic infections like Tuberculosis, fungal and parasitic diseases which are also seen in HIV-positive patients. We report a case without risk factors or laboratory evidence of HIV infection who presented with refractory cryptococcal meningitis and was found to have ICL. Key Words Cryptococcus, CD4, idiopathic For correspondence: Dr. Vivek Lal, Department of Neurology, PGIMER, Sector-12, Chandigarh-160 012, India. E-mail: [email protected] Ann Indian Acad Neurol 2010;13:136-8 [DOI: 10.4103/0972-2327.64646] Introduction and decreased pain and temperature sensation in the right half of the body, with sparing of the face. The neurological Idiopathic CD4 lymphocytopenia (ICL) was defi ned by the examination was otherwise normal. Plain magnetic resonance United States Centers for Disease Control and Prevention imaging (MRI) brain revealed a T2 hyperintensity in the (CDC) as a clinical condition in patients with depressed left thalamus, extending to involve the left corona radiata numbers of circulating CD4 T lymphocytes (<300 cells/µl or [Figure 1]. There was no meningeal enhancement on contrast- <20% of total T cells) at a minimum of two separate time points enhanced MRI. -

Chronic Mucocutaneous Candidiasis Associated with Paracoccidioidomycosis in a Patient with Mannose Receptor Deficiency: First Case Reported in the Literature
Revista da Sociedade Brasileira de Medicina Tropical Journal of the Brazilian Society of Tropical Medicine Vol.:54:(e0008-2021): 2021 https://doi.org/10.1590/0037-8682-0008-2021 Case Report Chronic mucocutaneous candidiasis associated with paracoccidioidomycosis in a patient with mannose receptor deficiency: First case reported in the literature Dewton de Moraes Vasconcelos[1], Dalton Luís Bertolini[1] and Maurício Domingues Ferreira[1] [1]. Universidade de São Paulo, Faculdade de Medicina, Hospital das Clinicas, Departamento de Dermatologia, Ambulatório das Manifestações Cutâneas das Imunodeficiências Primárias, São Paulo, SP, Brasil. Abstract We describe the first report of a patient with chronic mucocutaneous candidiasis associated with disseminated and recurrent paracoccidioidomycosis. The investigation demonstrated that the patient had a mannose receptor deficiency, which would explain the patient’s susceptibility to chronic infection by Candida spp. and systemic infection by paracoccidioidomycosis. Mannose receptors are responsible for an important link between macrophages and fungal cells during phagocytosis. Deficiency of this receptor could explain the susceptibility to both fungal species, suggesting the impediment of the phagocytosis of these fungi in our patient. Keywords: Chronic mucocutaneous candidiasis. Paracoccidioidomycosis. Mannose receptor deficiency. INTRODUCTION “chronic mucocutaneous candidiasis and mannose receptor deficiency,” “chronic mucocutaneous candidiasis and paracoccidioidomycosis,” Chronic mucocutaneous -

Identification of Culture-Negative Fungi in Blood and Respiratory Samples
IDENTIFICATION OF CULTURE-NEGATIVE FUNGI IN BLOOD AND RESPIRATORY SAMPLES Farida P. Sidiq A Dissertation Submitted to the Graduate College of Bowling Green State University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY May 2014 Committee: Scott O. Rogers, Advisor W. Robert Midden Graduate Faculty Representative George Bullerjahn Raymond Larsen Vipaporn Phuntumart © 2014 Farida P. Sidiq All Rights Reserved iii ABSTRACT Scott O. Rogers, Advisor Fungi were identified as early as the 1800’s as potential human pathogens, and have since been shown as being capable of causing disease in both immunocompetent and immunocompromised people. Clinical diagnosis of fungal infections has largely relied upon traditional microbiological culture techniques and examination of positive cultures and histopathological specimens utilizing microscopy. The first has been shown to be highly insensitive and prone to result in frequent false negatives. This is complicated by atypical phenotypes and organisms that are morphologically indistinguishable in tissues. Delays in diagnosis of fungal infections and inaccurate identification of infectious organisms contribute to increased morbidity and mortality in immunocompromised patients who exhibit increased vulnerability to opportunistic infection by normally nonpathogenic fungi. In this study we have retrospectively examined one-hundred culture negative whole blood samples and one-hundred culture negative respiratory samples obtained from the clinical microbiology lab at the University of Michigan Hospital in Ann Arbor, MI. Samples were obtained from randomized, heterogeneous patient populations collected between 2005 and 2006. Specimens were tested utilizing cetyltrimethylammonium bromide (CTAB) DNA extraction and polymerase chain reaction amplification of internal transcribed spacer (ITS) regions of ribosomal DNA utilizing panfungal ITS primers. -

Fungal Infections Fungi
Antifungal, Antiprotozoal, Anthelmintic Drugs Dr n. med. Marta Jóźwiak-Bębenista Department of Pharmacology Medical University of Lodz Fungal infections • also called mycoses; widespread in the population (e.g. „athlete's foot” or „thrush”) • become a more serious problem (immunocompromised patients – even fetal!) • are more difficult to treat than bacterial infections • therapy of fungal infections usually requires prolonged treatment! • opportunistic infections- Pneumocystis carinii Fungi Yeasts Moulds Higher Fungi 1 Clinically important fungi may be classified into: • yeasts (e.g. Cryptococcus neoformans) • yeast-like fungi that produce a structure resembling a mycelium (e.g. Candida albicans) • filamentous fungi with a true mycelium (e.g. Trichophyton spp., Microsporum spp., Epidermophyton spp., Tinea spp., Aspergillus fumigatus ) • „dimorphic” fungi that, depending on nutritional constraints, may grow as either yeasts or filamentous fungi (e.g. Histoplasma capsulatum, Coccidioides immitis, Blastomyces dermatides) Fungal infections Superficial (topical) Systemic („disseminated”) 1. cutaneous surfaces - skin, nails, hair 2. mucous membrane surfaces - oropharynx, vagina Fungal infections Superficial Systemic • Dermatomycoses - infections • Candidiasis of the skin, hair and nails; caused by • Cryptococcal meningitis Trichophyton • Pulmonary aspergillosis Microsporum Epidermophyton • Blastomycosis Tinea capitis (scalp) • Histoplasmosis Tinea cruris (groin) • Coccidiomycosis Tinea pedis (athlete's foot) • Paracoccidiomycosis Tinea corporis -

Department of Biological Sciences Redeemer's
DEPARTMENT OF BIOLOGICAL SCIENCES REDEEMER’S UNIVERSITY MCB 313 PATHOGENIC MYCOLOGY DURUGBO ERNEST UZODIMMA (Ph.D.) COURSE OUTLINE 1. Introduction 2. Structure, reproduction and classification of pathogenic Fungi Eg. Aspergillus, Trichphyton spp., Tinea spp.,Yeasts 3.Superficial systematic mycoses and antimycoses 4. Fungal infections ( Candidiasis , Histoplasmosis etc) 5. Laboratory methods of study 5. Pathology and immunology 6. Cultivation techniques in Mycology Structure, Reproduction and Classification of Pathogenic Fungi About 30% of the 100,000 known species of Fungi make a living as parasites, or pathogens , mostly of plants. E. g Cryphonectria parasitica, the Ascomycete fungus causes chestnut blight. Fusarium circinatum causes pith pine canker a diseae that threatens pine worldwide. Puccinia graminis causes black stem rust of wheat. Some of the fungi that attack food crops are toxic to humans for example certain species of the ascomycete mold Aspergillus contaminate improperly stored grain and peanuts by secreting aflatoxins which are carcinogenic. The ascomycete Claviceps purpurea which grows on rye plants forming purple structures called ergots. If diseased rye is milled into flour and consumed it causes ergotism, a condition characterized by gangrene, nervous spasms, burning sensations, hallucinations, and temporary insanity. An epidemic of this around 944 C.E, killed more than 40,000 people in France. Animals are much less susceptible to parasitic fungi than plants. Only about 50 species of fungi are known to parasitize humans and animals . Such fungal infections are mycosis . Skin mycoses includes ringworm. The ascomycetes that causes ringworm can infect almost any skin surface. Most commonly, they grow on the feet, causing the intense itching and blisters known as athlete ’s foot. -

DIFLUCAN Capsule and IV
Generic Name: Fluconazole Trade Name: Diflucan CDS Effective Date: April 16, 2020 Supersedes: March 19, 2020 Approved by BPOM: April 19, 2021 PT. PFIZER INDONESIA Local Product Document Generic Name: Fluconazole Trade Name: Diflucan CDS Effective Date: April 16, 2020 Supersedes: March 19, 2020 DESCRIPTION Fluconazole is a bis-triazole: 2-(2,4-difluorophenyl)-1,3-bis (1H-1,2,4-triazol-1yl)-2 propanol. It has the following structural formula: N OH N N N CH2 C CH2 N N F F Fluconazole is a white to off-white crystalline powder which is sparingly soluble in water and saline. It has a molecular weight of 306.3. Diflucan capsules contain 50 mg and 150 mg of fluconazole and the following inactive ingredients: hard gelatin capsules (which may contain Blue 5 and other inert ingredients), lactose, corn starch, silicon dioxide, magnesium stearate and sodium lauryl sulfate. Diflucan for injection is an iso-osmotic, sterile, non-pyrogenic solution of fluconazole in a sodium chloride diluent. Each ml contains 2 mg of fluconazole and 9 mg of sodium chloride. The pH ranges from 4.0 to 8.6. Injection volumes of 100 ml are packaged in glass infusion vials. 2020-0059186 Page 1 of 19 Generic Name: Fluconazole Trade Name: Diflucan CDS Effective Date: April 16, 2020 Supersedes: March 19, 2020 Approved by BPOM: April 19, 2021 PHARMACOLOGICAL PROPERTIES Pharmacodynamic Properties Pharmacotherapeutic group: Antimycotics for systemic use, triazole derivatives, ATC code J02AC01. Mode of Action Fluconazole, a triazole antifungal agent, is a potent and specific inhibitor of fungal sterol synthesis. Its primary mode of action is the inhibition of fungal cytochrome P-450-mediated 14-alpha-lanosterol demethylation, an essential step in fungal ergosterol biosynthesis. -

Pulmonary Cryptococcosis Secondary To
& My gy co lo lo ro g i y V Ramana et al., Virol Mycol 2012, 1:3 Virology & Mycology DOI: 10.4172/2161-0517.1000107 ISSN: 2161-0517 Case Report Open Access Pulmonary Cryptococcosis Secondary to Bronchial Asthma Presenting as Type I Respiratory Failure- A Case Report with Review of Literature KV Ramana*, Moses Vinay Kumar, Sanjeev D Rao, Akhila R, Sandhya, Shruthi P, Pranuthi M, Krishnappa M, Anand K Department of Microbiology, Prathima Inst of Medical Sciences, Nagunur, Karimnagar, Andhrapradesh, India Introduction mellitus, pleuritis, systemic lupus erythematus, cushings syndrome, Continous Ambulatory Peritoneal Dialysis (CAPD), liver cirrhosis, Cryptococcus spp, was first isolated and described in 1894 by cancer, organ transplants, spleenectomy, malnutrition, leprosy, Sanfelice F in Italy from peach juice and named it as Saccharomyces pulmonary tuberculosis and those on cortico steroid therapy [13-20]. neoformans, is an yeast like fungus [1], first isolated from a clinical Pulmonary Cryptococcosis may be presenting as pleural effusions, specimen by Busse in the same year from Germany [2]. Cryptococci solitary or multiple masses, glass-ground interstitial opacities, dense are a saprophytic fungi present in soil contaminated with bird consolidations, patchy, segmented or lobar air space consolidation droppings mainly of pigeons, roosting sites and decaying vegetables (cryptococcal pneumonia) and nodular and reticulonodular cavities. [3]. Previous reports have also showed the presence of Cryptococcus Differential diagnosis of pulmonary cryptococcosis should be done spp colonized in the nasopharynx and on skin of healthy individuals with pneumonia [21,22]. Review of literature showed only two previous [4]. Belonging to Basidiomyctes group of fungi Cryptococcus spp reported cases of pulmonary cryptococcosis presenting as acute primarily infects central nervous system causing meningoencephalitis respiratory failure [7,23,24].