Idiopathic CD4 Lymphocytopenia Presenting As Refractory Cryptococcal Meningitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic CD4 Lymphocytopenia: Spectrum of Opportunistic Infections, Malignancies, and Autoimmune Diseases
Published online: 2021-08-09 REVIEW ARTICLE Idiopathic CD4 Lymphocytopenia: Spectrum of opportunistic infections, malignancies, and autoimmune diseases Dina S. Ahmad, Mohammad Esmadi, William C. Steinmann Department of Internal Medicine, University of Missouri School of Medicine, Columbia, MO, USA Access this article online ABSTRACT Website: www.avicennajmed.com DOI: 10.4103/2231-0770.114121 Idiopathic CD4 lymphocytopenia (ICL) was first defined in 1992 by the US Centers for Disease Quick Response Code: Control and Prevention (CDC) as the repeated presence of a CD4+ T lymphocyte count of fewer than 300 cells per cubic millimeter or of less than 20% of total T cells with no evidence of human immunodeficiency virus (HIV) infection and no condition that might cause depressed CD4 counts. Most of our knowledge about ICL comes from scattered case reports. The aim of this study was to collect comprehensive data from the previously published cases to understand the characteristics of this rare condition. We searched the PubMed database and Science Direct for case reports since 1989 for Idiopathic CD4 lymphocytopenia cases. We found 258 cases diagnosed with ICL in 143 published papers. We collected data about age, sex, pathogens, site of infections, CD4 count, CD8 count, CD4:CD8 ratio, presence of HIV risk factors, malignancies, autoimmune diseases and whether the patients survived or died. The mean age at diagnosis of first opportunistic infection (or ICL if no opportunistic infection reported) was 40.7 ± 19.2 years (standard deviation), with a range of 1 to 85. One-sixty (62%) patients were males, 91 (35.2%) were females, and 7 (2.7%) patients were not identified whether males or females. -

153.Full.Pdf
Copyright Ó 2010 by the Genetics Society of America DOI: 10.1534/genetics.109.113027 A Tetrad Analysis of the Basidiomycete Fungus Cryptococcus neoformans Alexander Idnurm Division of Cell Biology and Biophysics, School of Biological Sciences, University of Missouri-Kansas City, Kansas City, Missouri 64110 Manuscript received December 10, 2009 Accepted for publication February 9, 2010 ABSTRACT Cryptococcus neoformans is a basidiomycete fungus that is found worldwide and causes disease in humans and animal species. The fungus grows asexually as a budding yeast. Under laboratory conditions it is capable of sexual reproduction between two mating types. After cell fusion a dikaryotic filament develops, at the tip of which a basidium gives rise to four chains of basidiospores. Because the chains each comprise 10–30 spores, rather than single spores, the analysis of individual meiotic events has not been attempted in C. neoformans in the style of tetrad analyses performed in other fungal species. Here, the basidiospores from .100 basidia were micromanipulated and the resultant .2500 progeny analyzed for three genetic markers to understand the sexual process in this fungus, leading to four observations: (i) Marker seg- regation provides genetic evidence for a single meiotic event within the basidium followed by multiple rounds of mitosis. (ii) Using each basidium as an unordered tetrad, the ADE2 and URA5 genes are linked to their centromeres, consistent with adjacent genomic regions rich in repetitive elements predicted to comprise Cryptococcus centromeres. (iii) Lack of germination of basidiospores is attributed to aneuploidy, rather than dormancy. (iv) Analysis of basidiospores derived from single chains demonstrates that each chain can contain different genotypes. -

Product Sheet Info
Product Information Sheet for NR-50430 Cryptococcus gattii, Strain C10 Propagation: 1. Keep vial frozen until ready for use; thaw rapidly. Catalog No. NR-50430 2. Inoculate an agar plate with approximately 50 µL of thawed culture and/or transfer the entire thawed aliquot into a single tube of broth For research use only. Not for human use. 3. Incubate the plate and/or tube at 25°C for 2 to 4 days. Contributor: Citation: Brian Wong, M.D., Professor, and Igor Bruzual, Ph.D., Acknowledgment for publications should read “The following Infectious Disease Division, Department of Medicine, Oregon reagent was obtained through BEI Resources, NIAID, NIH: Health and Science University, Portland, Oregon, USA Cryptococcus gattii, Strain C10, NR-50430.” Manufacturer: Biosafety Level: 2 BEI Resources Appropriate safety procedures should always be used with this material. Laboratory safety is discussed in the following Product Description: publication: U.S. Department of Health and Human Services, Classification: Tremellaceae, Cryptococcus Public Health Service, Centers for Disease Control and Species: Cryptococcus gattii Prevention, and National Institutes of Health. Biosafety in Strain: C10 Microbiological and Biomedical Laboratories. 5th ed. Original Source: Cryptococcus gattii (C. gattii), strain C10 Washington, DC: U.S. Government Printing Office, 2009; see was isolated from an unknown human source in the Pacific www.cdc.gov/biosafety/publications/bmbl5/index.htm. Northwest region of North America.1 Comments: C. gattii, strain C10 was deposited as lineage Disclaimers: VGIIa and resistant to azoles.1 You are authorized to use this product for research use only. The Cryptococcus species complex is comprised of four It is not intended for human use. -
Cryptococcus Gattii Outbreak
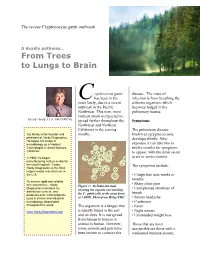
The recent Cryptococcus gattii outbreak A deadly pathway… From Trees to Lungs to Brain ryptococcus gattii disease. The route of C has been in the infection is from breathing the news lately, due to a recent airborne organism, which outbreak in the Pacific becomes lodged in the Northwest. This new, more pulmonary tissues. virulent strain is expected to by Jay Hardy, CLS, SM (NRCM) spread further throughout the Symptoms Northwest and Northern California in the coming The pulmonary disease, Jay Hardy is the founder and months. known as cpryptococcosis, president of Hardy Diagnostics. develops slowly. After He began his career in exposure it can take two to microbiology as a Medical Technologist in Santa Barbara, twelve months for symptoms California. to appear, with the usual onset In 1980, he began at six or seven months. manufacturing culture media for the local hospitals. Today, The symptoms include: Hardy Diagnostics is the third largest media manufacturer in the U.S. • Cough that lasts weeks or months To ensure rapid and reliable turn around time, Hardy • Sharp chest pain Figure 1: An India ink stain Diagnostics maintains six • Unexplained shortness of showing the capsule surrounding distribution centers, and breath produces over 3,000 products the C. gattii cells in the yeast form used in clinical and industrial at 1,000X. Photo from Haley/CDC. • Severe headache microbiology laboratories • Confusion throughout the world. The organism is a fungus that • Fever is usually found in the soil • Night sweats www.HardyDiagnostics.com and on trees. It is not spread • Unintended weight loss from human to human or animal to human. -

Safety Precautions for Working with Cryptococcus Neoformans
Safety Precautions for Working with Cryptococcus neoformans The basidiomycete fungus Cryptococcus neoformans is an invasive opportunistic pathogen of the central nervous system and the most frequent cause of fungal meningitis worldwide. Although Cryptococcus is a problem in the United States, it is significantly more prevalent and especially devastating in the developing world, such as sub-Saharan Africa, resulting in in more than 625,000 deaths per year worldwide. C. neoformans survives in the environment within soil, trees, and bird guano, where it can interact with wild animals or microbial predators, maintaining its virulence. Human infection is thought to be acquired by inhalation of desiccated yeast cells or spores from an environmental source. C. neoformans can colonize the host respiratory tract without producing any disease. Infection is typically asymptomatic, and it can be either cleared or enter a dormant, latent form. When host immunity is compromised, the dormant form can be reactivated and disseminate hematogenously to cause systemic infection. C. neoformans can infect or spread to any organ to cause localized infections involving the skin, eyes, myocardium, bones, joints, lungs, prostate gland, or urinary tract, in addition to its propensity to infect the central nervous systems. The following diseases and medications are risk factors for C. neoformans infection and are associated with at least some degree of immunosuppression: Ø HIV/AIDs (CD4 < 100cells/mm) Ø Corticosteroids or other immunosuppressive medications for cancer, chemotherapy, or organ transplants Ø Solid organ transplantations Ø Diabetes mellitus Ø Heart, lung, or liver disease Ø Pregnancy Even otherwise healthy, fully immunocompetent individuals can develop cryptococcosis, as may well be the case in a lab accident. -

Environmental Factors That Contribute to the Maintenance of Cryptococcus Neoformans Pathogenesis
microorganisms Review Environmental Factors That Contribute to the Maintenance of Cryptococcus neoformans Pathogenesis Maphori Maliehe, Mathope A. Ntoi, Shayanki Lahiri, Olufemi S. Folorunso , Adepemi O. Ogundeji , Carolina H. Pohl and Olihile M. Sebolai * Department of Microbial, Biochemical and Food Biotechnology, University of the Free State, Bloemfontein 9301, Free State, South Africa; [email protected] (M.M.); [email protected] (M.A.N.); [email protected] (S.L.); [email protected] (O.S.F.); [email protected] (A.O.O.); [email protected] (C.H.P.) * Correspondence: [email protected]; Tel.: +27-(0)51-401-2004 Received: 15 November 2019; Accepted: 11 December 2019; Published: 28 January 2020 Abstract: The ability of microorganisms to colonise and display an intracellular lifestyle within a host body increases their fitness to survive and avoid extinction. This host–pathogen association drives microbial evolution, as such organisms are under selective pressure and can become more pathogenic. Some of these microorganisms can quickly spread through the environment via transmission. The non-transmittable fungal pathogens, such as Cryptococcus, probably return into the environment upon decomposition of the infected host. This review analyses whether re-entry of the pathogen into the environment causes restoration of its non-pathogenic state or whether environmental factors and parameters assist them in maintaining pathogenesis. Cryptococcus (C.) neoformans is therefore used as a model organism to evaluate the impact of environmental stress factors that aid the survival and pathogenesis of C. neoformans intracellularly and extracellularly. Keywords: Cryptococcus; environmental factors; pathogenesis; survival; virulence factors; transcriptional factors; signalling factors 1. Introduction The genus Cryptococcus is defined by basidiomycetous fungi that can transform into a yeast state [1]. -

Pulmonary Cryptococcus Infections As a Manifestation of Idiopathic CD4 Lymphocytopenia: Case Report and Literature Review
University of Calgary PRISM: University of Calgary's Digital Repository Libraries & Cultural Resources Open Access Publications 2019-10-17 Pulmonary Cryptococcus infections as a manifestation of idiopathic CD4 lymphocytopenia: case report and literature review Thornton, Christina S; Larios, Oscar; Grossman, Jennifer; Griener, Thomas P; Vaughan, Steven BMC Infectious Diseases. 2019 Oct 17;19(1):862 http://hdl.handle.net/1880/111155 Journal Article Downloaded from PRISM: https://prism.ucalgary.ca Thornton et al. BMC Infectious Diseases (2019) 19:862 https://doi.org/10.1186/s12879-019-4453-x CASE REPORT Open Access Pulmonary Cryptococcus infections as a manifestation of idiopathic CD4 lymphocytopenia: case report and literature review Christina S. Thornton1* , Oscar Larios2, Jennifer Grossman3, Thomas P. Griener4 and Steven Vaughan2 Abstract Background: Idiopathic CD4 lymphocytopenia (ICL) is a rare clinical disease with relative CD4 deficiency in the absence of HIV infection. The pathogenicity of ICL is poorly understood with an unclear incidence rate in the general population. Sequelae of ICL includes AIDS-defining infections, which most commonly includes Cryptococcus neoformans. Typically, C. neoformans infections present with CNS involvement but rarely with extra-CNS manifestations. Here, we present a rare case of ICL with exclusively primary pulmonary cryptococcus and a review of the literature. Case presentation: A 56-year-old female presented to our tertiary care hospital requiring a right hip open reduction intervention. The patient became febrile during admission, prompting a work-up that included a chest X-ray showing a peripheral pulmonary solitary nodule. Transthoracic biopsy revealed encapsulated yeast forms in keeping with C. neoformans. CD4 counts, repeated at least one month apart, were < 200 cells/mm3, with negative HIV testing. -
Influence of Galectin-3 on the Innate Immune Response During
Journal of Fungi Article Influence of Galectin-3 on the Innate Immune Response during Experimental Cryptococcosis Caroline Patini Rezende 1, Patricia Kellen Martins Oliveira Brito 2 , Thiago Aparecido Da Silva 2 , Andre Moreira Pessoni 1 , Leandra Naira Zambelli Ramalho 3 and Fausto Almeida 1,* 1 Department of Biochemistry and Immunology, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto 14049-900, SP, Brazil; [email protected] (C.P.R.); [email protected] (A.M.P.) 2 Department of Cellular and Molecular Biology, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto 14049-900, SP, Brazil; [email protected] (P.K.M.O.B.); [email protected] (T.A.D.S.) 3 Department of Pathology, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto 14049-900, SP, Brazil; [email protected] * Correspondence: [email protected] Abstract: Cryptococcus neoformans, the causative agent of cryptococcosis, is the primary fungal pathogen that affects the immunocompromised individuals. Galectin-3 (Gal-3) is an animal lectin involved in both innate and adaptive immune responses. The present study aimed to evaluate the influence of Gal-3 on the C. neoformans infection. We performed histopathological and gene profile analysis of the innate antifungal immunity markers in the lungs, spleen, and brain of the wild-type (WT) and Gal-3 knockout (KO) mice during cryptococcosis. These findings suggest that Gal-3 absence does not cause significant histopathological alterations in the analyzed tissues. The expression profile of the genes related to innate antifungal immunity showed that the presence of cryptococcosis in Citation: Rezende, C.P.; Brito, the WT and Gal-3 KO animals, compared to their respective controls, promoted the upregulation P.K.M.O.; Da Silva, T.A.; Pessoni, of the pattern recognition receptor (PRR) responsive to mannose/chitin (mrc1) and a gene involved A.M.; Ramalho, L.N.Z.; Almeida, F. -

Cryptococcus Randhawai Sp. Nov., a Novel Anamorphic Basidiomycetous Yeast Isolated from Tree Trunk Hollow of Ficus Religiosa (Peepal Tree) from New Delhi, India
Antonie van Leeuwenhoek (2010) 97:253–259 DOI 10.1007/s10482-009-9406-8 ORIGINAL PAPER Cryptococcus randhawai sp. nov., a novel anamorphic basidiomycetous yeast isolated from tree trunk hollow of Ficus religiosa (peepal tree) from New Delhi, India Zia U. Khan • Suhail Ahmad • Ferry Hagen • Jack W. Fell • Tusharantak Kowshik • Rachel Chandy • Teun Boekhout Received: 16 September 2009 / Accepted: 8 December 2009 / Published online: 20 December 2009 Ó Springer Science+Business Media B.V. 2009 Abstract A novel anamorphic Cryptococcus spe- ethylamine. With respect to C. friedmannii, it differed cies is described, which was isolated in New Delhi in growth temperature, ability to assimilate lactose, (India) from decaying wood of a tree trunk hollow of raffinose, L-rhamnose, myo-inositol, and inability to Ficus religiosa. On the basis of sequence analysis of utilize citrate. Furthermore, our isolate also differed the D1/D2 domains of the 26S rRNA gene and the from C. cerealis in growth temperature, presence of internally transcribed spacer (ITS)-1 and ITS-2 capsule and inability to assimilate L-sorbose. In view region sequences, the isolate belonged to the Cryp- of the above phenotypic differences and unique tococcus albidus cluster (Filobasidiales, Tremello- rDNA sequences, we consider that our isolate repre- mycetes) and was closely related to Cryptococcus sents a new species of Cryptococcus, and therefore, a saitoi, Cryptococcus cerealis and Cryptococcus new species, Cryptococcus randhawai is proposed for friedmannii with 98% sequence identity. Phenotypi- this taxon. The type strain J11/2002 has been cally, the species differed from C. saitoi with respect deposited in the culture collection of the Centraalbu- to growth temperature (up to 37oC), presence of a reau voor Schimmelcultures (CBS10160) and CABI thin capsule, ability to grow in the absence of Biosciences (IMI 393306). -

12 Tremellomycetes and Related Groups
12 Tremellomycetes and Related Groups 1 1 2 1 MICHAEL WEIß ,ROBERT BAUER ,JOSE´ PAULO SAMPAIO ,FRANZ OBERWINKLER CONTENTS I. Introduction I. Introduction ................................ 00 A. Historical Concepts. ................. 00 Tremellomycetes is a fungal group full of con- B. Modern View . ........................... 00 II. Morphology and Anatomy ................. 00 trasts. It includes jelly fungi with conspicuous A. Basidiocarps . ........................... 00 macroscopic basidiomes, such as some species B. Micromorphology . ................. 00 of Tremella, as well as macroscopically invisible C. Ultrastructure. ........................... 00 inhabitants of other fungal fruiting bodies and III. Life Cycles................................... 00 a plethora of species known so far only as A. Dimorphism . ........................... 00 B. Deviance from Dimorphism . ....... 00 asexual yeasts. Tremellomycetes may be benefi- IV. Ecology ...................................... 00 cial to humans, as exemplified by the produc- A. Mycoparasitism. ................. 00 tion of edible Tremella fruiting bodies whose B. Tremellomycetous Yeasts . ....... 00 production increased in China alone from 100 C. Animal and Human Pathogens . ....... 00 MT in 1998 to more than 250,000 MT in 2007 V. Biotechnological Applications ............. 00 VI. Phylogenetic Relationships ................ 00 (Chang and Wasser 2012), or extremely harm- VII. Taxonomy................................... 00 ful, such as the systemic human pathogen Cryp- A. Taxonomy in Flow -

Cryptococcus Gattii Reporting and Investigation Guideline
Cryptococcus gattii Signs and • Symptoms depend on affected body system; typically pneumonia (cough, Symptoms shortness of breath, chest pain, fever) and/or meningitis (headache, fever, neck pain, nausea and vomiting, sensitivity to light, altered mental status). May be asymptomatic. • Cryptococcomas in the lungs, skin, brain, or other organs. Incubation Not well-established; average 6-7 months (range 2-13 months), potentially years. Case Clinical criteria: None required classification Confirmed: A case with any of the following from a clinical specimen: isolation of C. gattii; detection of C. gattii-specific nucleic acid; demonstration of C. gattii by immunohistochemistry; MALDI-TOF result specific for C. gattii Differential Coccidioidomycosis, histoplasmosis, blastomycosis, other fungal infections, viral or diagnosis bacterial causes of pneumonia or meningitis Treatment Appropriate antifungal, generally fluconazole for asymptomatic to moderate pulmonary infections or amphotericin B and flucytosine for severe lung infections or CNS infections. Case fatality rate in published literature ranges from 13-33%. Duration Can cause long-term infection; treatment needs to be continued for at least 6 months. Some people may require surgery to remove cryptococcomas. Exposure Inhalation of fungal spores from the environment in endemic regions. No person-to- person or animal-to-person transmission. Laboratory Local Health Jurisdiction (LHJ) and Communicable Disease Epidemiology (CDE) arrange testing testing for individual cases and environmental testing for suspected outbreaks. Isolates should be submitted for speciation. • Washington State Public Health Laboratories can facilitate testing at CDC • Best specimens: Fungal isolate. Testing can be arranged for serum or cerebrospinal fluid (CSF), although tests on these specimens do not differentiate C. gattii from other Cryptococcus species Specimen shipping (Section 4): • Isolates must be submitted on a slant with a screw top. -

Innate Immunity Against Cryptococcus, from Recognition to Elimination
Journal of Fungi Review Innate Immunity against Cryptococcus, from Recognition to Elimination Althea Campuzano 1,2 ID and Floyd L. Wormley Jr. 1,2,* 1 Department of Biology, The University of Texas at San Antonio, San Antonio, TX 78249, USA; [email protected] 2 South Texas Center for Emerging Infectious Diseases, The University of Texas at San Antonio, San Antonio, TX 78249, USA * Correspondence: fl[email protected]; Tel.: +1-210-458-7021 Received: 20 February 2018; Accepted: 4 March 2018; Published: 7 March 2018 Abstract: Cryptococcus species, the etiological agents of cryptococcosis, are encapsulated fungal yeasts that predominantly cause disease in immunocompromised individuals, and are responsible for 15% of AIDS-related deaths worldwide. Exposure follows the inhalation of the yeast into the lung alveoli, making it incumbent upon the pattern recognition receptors (PRRs) of pulmonary phagocytes to recognize highly conserved pathogen-associated molecular patterns (PAMPS) of fungi. The main challenges impeding the ability of pulmonary phagocytes to effectively recognize Cryptococcus include the presence of the yeast’s large polysaccharide capsule, as well as other cryptococcal virulence factors that mask fungal PAMPs and help Cryptococcus evade detection and subsequent activation of the immune system. This review will highlight key phagocyte cell populations and the arsenal of PRRs present on these cells, such as the Toll-like receptors (TLRs), C-type lectin receptors, NOD-like receptors (NLRs), and soluble receptors. Additionally, we will highlight critical cryptococcal PAMPs involved in the recognition of Cryptococcus. The question remains as to which PRR–ligand interaction is necessary for the recognition, phagocytosis, and subsequent killing of Cryptococcus.