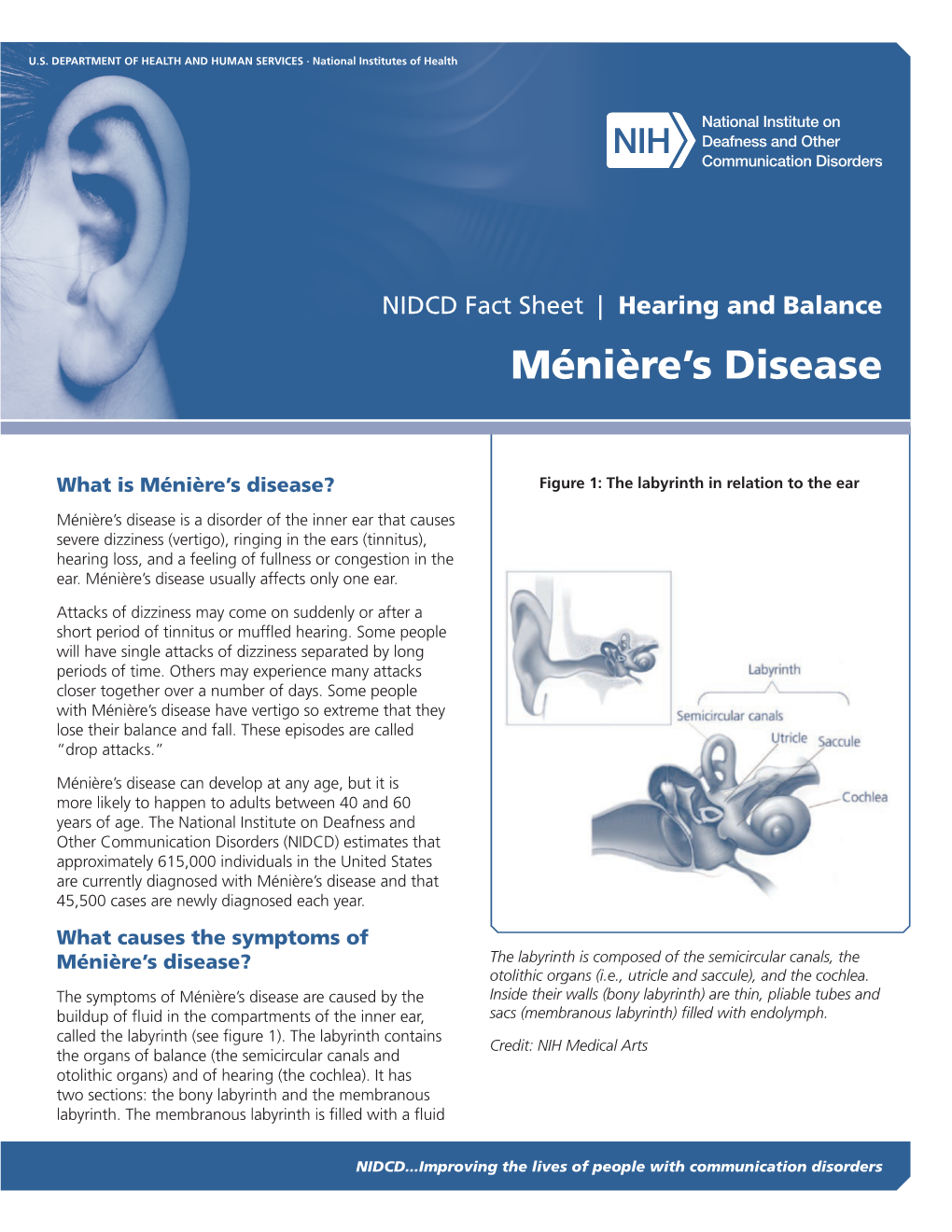
Ménière's Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hearing Screening Training Manual REVISED 12/2018
Hearing Screening Training Manual REVISED 12/2018 Minnesota Department of Health (MDH) Community and Family Health Division Maternal and Child Health Section 1 2 For more information, contact Minnesota Department of Health Maternal Child Health Section 85 E 7th Place St. Paul, MN 55164-0882 651-201-3760 [email protected] www.health.state.mn.us Upon request, this material will be made available in an alternative format such as large print, Braille or audio recording. 3 Revisions made to this manual are based on: Guidelines for Hearing Screening After the Newborn Period to Kindergarten Age http://www.improveehdi.org/mn/library/files/afternewbornperiodguidelines.pdf American Academy of Audiology, Childhood Screening Guidelines http://www.cdc.gov/ncbddd/hearingloss/documents/AAA_Childhood%20Hearing%2 0Guidelines_2011.pdf American Academy of Pediatrics (AAP), Hearing Assessment in Children: Recommendations Beyond Neonatal Screening http://pediatrics.aappublications.org/content/124/4/1252 4 Contents Introduction .................................................................................................................... 7 Audience ..................................................................................................................... 7 Purpose ....................................................................................................................... 7 Overview of hearing and hearing loss ............................................................................ 9 Sound, hearing, and hearing -

Migraine Associated Vertigo
Headache: The Journal of Head and Face Pain VC 2015 American Headache Society Published by JohnWiley & Sons, Inc. doi: 10.1111/head.12704 Headache Toolbox Migraine Associated Vertigo Between 30 and 50% of migraineurs will sometimes times a condition similar to benign positional vertigo experience dizziness, a sense of spinning, or feeling like called vestibular neuronitis (or vestibular neuritis/labyrinthi- their balance is off in the midst of their headaches. This is tis) is triggered by a viral infection of the inner ear, result- now termed vestibular migraine, but is also called ing in constant vertigo or unsteadiness. Symptoms can migraine associated vertigo. Sometimes migraineurs last for a few days to a few weeks and then go away as experience these symptoms before the headache, but mysteriously as they came on. Vestibular migraine, by they can occur during the headache, or even without any definition, should have migraine symptoms in at least head pain. In children, vertigo may be a precursor to 50% of the vertigo episodes, and these include head migraines developing in the teens or adulthood. Migraine pain, light and noise sensitivity, and nausea. associated vertigo may be more common in those with There are red flags, which are warning signs that ver- motion sickness. tigo is not part of a migraine. Sudden hearing loss can be For some patients this vertiginous sensation resem- the sign of an infection that needs treatment. Loss of bal- bles migraine aura, which is a reversible, relatively short- ance alone, or accompanied by weakness can be the lived neurologic symptom associated with their migraines. -

Vestibular Neuritis and Labyrinthitis
Vestibular Neuritis and DISORDERS Labyrinthitis: Infections of the Inner Ear By Charlotte L. Shupert, PhD with contributions from Bridget Kulick, PT and the Vestibular Disorders Association INFECTIONS Result in damage to inner ear and/or nerve. ARTICLE 079 DID THIS ARTICLE HELP YOU? SUPPORT VEDA @ VESTIBULAR.ORG Vestibular neuritis and labyrinthitis are disorders resulting from an 5018 NE 15th Ave. infection that inflames the inner ear or the nerves connecting the inner Portland, OR 97211 ear to the brain. This inflammation disrupts the transmission of sensory 1-800-837-8428 information from the ear to the brain. Vertigo, dizziness, and difficulties [email protected] with balance, vision, or hearing may result. vestibular.org Infections of the inner ear are usually viral; less commonly, the cause is bacterial. Such inner ear infections are not the same as middle ear infections, which are the type of bacterial infections common in childhood affecting the area around the eardrum. VESTIBULAR.ORG :: 079 / DISORDERS 1 INNER EAR STRUCTURE AND FUNCTION The inner ear consists of a system of fluid-filled DEFINITIONS tubes and sacs called the labyrinth. The labyrinth serves two functions: hearing and balance. Neuritis Inflamation of the nerve. The hearing function involves the cochlea, a snail- shaped tube filled with fluid and sensitive nerve Labyrinthitis Inflamation of the labyrinth. endings that transmit sound signals to the brain. Bacterial infection where The balance function involves the vestibular bacteria infect the middle organs. Fluid and hair cells in the three loop-shaped ear or the bone surrounding semicircular canals and the sac-shaped utricle and Serous the inner ear produce toxins saccule provide the brain with information about Labyrinthitis that invade the inner ear via head movement. -

Vestibular Neuritis, Labyrinthitis, and a Few Comments Regarding Sudden Sensorineural Hearing Loss Marcello Cherchi
Vestibular neuritis, labyrinthitis, and a few comments regarding sudden sensorineural hearing loss Marcello Cherchi §1: What are these diseases, how are they related, and what is their cause? §1.1: What is vestibular neuritis? Vestibular neuritis, also called vestibular neuronitis, was originally described by Margaret Ruth Dix and Charles Skinner Hallpike in 1952 (Dix and Hallpike 1952). It is currently suspected to be an inflammatory-mediated insult (damage) to the balance-related nerve (vestibular nerve) between the ear and the brain that manifests with abrupt-onset, severe dizziness that lasts days to weeks, and occasionally recurs. Although vestibular neuritis is usually regarded as a process affecting the vestibular nerve itself, damage restricted to the vestibule (balance components of the inner ear) would manifest clinically in a similar way, and might be termed “vestibulitis,” although that term is seldom applied (Izraeli, Rachmel et al. 1989). Thus, distinguishing between “vestibular neuritis” (inflammation of the vestibular nerve) and “vestibulitis” (inflammation of the balance-related components of the inner ear) would be difficult. §1.2: What is labyrinthitis? Labyrinthitis is currently suspected to be due to an inflammatory-mediated insult (damage) to both the “hearing component” (the cochlea) and the “balance component” (the semicircular canals and otolith organs) of the inner ear (labyrinth) itself. Labyrinthitis is sometimes also termed “vertigo with sudden hearing loss” (Pogson, Taylor et al. 2016, Kim, Choi et al. 2018) – and we will discuss sudden hearing loss further in a moment. Labyrinthitis usually manifests with severe dizziness (similar to vestibular neuritis) accompanied by ear symptoms on one side (typically hearing loss and tinnitus). -

Inner Ear Infection (Otitis Interna) in Dogs
Hurricane Harvey Client Education Kit Inner Ear Infection (Otitis Interna) in Dogs My dog has just been diagnosed with an inner ear infection. What is this? Inflammation of the inner ear is called otitis interna, and it is most often caused by an infection. The infectious agent is most commonly bacterial, although yeast and fungus can also be implicated in an inner ear infection. If your dog has ear mites in the external ear canal, this can ultimately cause a problem in the inner ear and pose a greater risk for a bacterial infection. Similarly, inner ear infections may develop if disease exists in one ear canal or when a benign polyp is growing from the middle ear. A foreign object, such as grass seed, may also set the stage for bacterial infection in the inner ear. Are some dogs more susceptible to inner ear infection? Dogs with long, heavy ears seem to be predisposed to chronic ear infections that ultimately lead to otitis interna. Spaniel breeds, such as the Cocker spaniel, and hound breeds, such as the bloodhound and basset hound, are the most commonly affected breeds. Regardless of breed, any dog with a chronic ear infection that is difficult to control may develop otitis interna if the eardrum (tympanic membrane) is damaged as it allows bacteria to migrate down into the inner ear. "Dogs with long, heavy ears seem to bepredisposed to chronic ear infections that ultimately lead to otitis interna." Excessively vigorous cleaning of an infected external ear canal can sometimes cause otitis interna. Some ear cleansers are irritating to the middle and inner ear and can cause signs of otitis interna if the eardrum is damaged and allows some of the solution to penetrate too deeply. -

Hearing Loss, Vertigo and Tinnitus
HEARING LOSS, VERTIGO AND TINNITUS Jonathan Lara, DO April 29, 2012 Hearing Loss Facts S Men are more likely to experience hearing loss than women. S Approximately 17 percent (36 million) of American adults report some degree of hearing loss. S About 2 to 3 out of every 1,000 children in the United States are born deaf or hard-of-hearing. S Nine out of every 10 children who are born deaf are born to parents who can hear. Hearing Loss Facts S The NIDCD estimates that approximately 15 percent (26 million) of Americans between the ages of 20 and 69 have high frequency hearing loss due to exposure to loud sounds or noise at work or in leisure activities. S Only 1 out of 5 people who could benefit from a hearing aid actually wears one. S Three out of 4 children experience ear infection (otitis media) by the time they are 3 years old. Hearing Loss Facts S There is a strong relationship between age and reported hearing loss: 18 percent of American adults 45-64 years old, 30 percent of adults 65-74 years old, and 47 percent of adults 75 years old or older have a hearing impairment. S Roughly 25 million Americans have experienced tinnitus. S Approximately 4,000 new cases of sudden deafness occur each year in the United States. Hearing Loss Facts S Approximately 615,000 individuals have been diagnosed with Ménière's disease in the United States. Another 45,500 are newly diagnosed each year. S One out of every 100,000 individuals per year develops an acoustic neurinoma (vestibular schwannoma). -

Sudden Bilateral Simultaneous Deafness with Vertigo As a Sole Manifestation of Vertebrobasilar Insufficiency H Lee, H a Yi, R W Baloh
539 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.4.539 on 1 April 2003. Downloaded from SHORT REPORT Sudden bilateral simultaneous deafness with vertigo as a sole manifestation of vertebrobasilar insufficiency H Lee, H A Yi, R W Baloh ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:539–541 CASE REPORT A 68 year old woman presented with bilateral sudden A 68 year old woman with long standing non-insulin depend- simultaneous hearing loss and transient spontaneous ent diabetes mellitus and hypertension suddenly developed vertigo as a sole manifestation of vertebrobasilar vertigo, vomiting, and bilateral tinnitus. Five minutes later, insufficiency. Extensive investigation to exclude other she noticed bilateral hearing loss. She had difficulty hearing causes was unremarkable. Magnetic resonance imaging her husband speak. She did not have dysarthria, numbness, of the brain, including diffusion images, showed no abnor- weakness, visual distortion, or incoordination. The hearing malities. A magnetic resonance angiogram showed severe loss persisted, but vertigo resolved over a few hours. Two days stenosis of the middle third of the basilar artery. A pure previously, she had had two episodes of transient vertigo and tone audiogram showed moderate sensorineural-type hearing loss involving the left ear that lasted no more than a hearing loss bilaterally. The localisation and mechanism of few minutes without any accompanying neurological symp- an isolated cochleovestibular dysfunction are discussed. toms. The patient had no previous history of hearing difficulty. There was no prior history of temporal bone fracture, menin- gitis, autoimmune disease, or exposure to ototoxic drugs. On admission, she had persistent bilateral hearing loss and ertebrobasilar insufficiency (VBI) can cause sudden non-specific dizziness with lightheadedness. -

Mathematical Model of the Cupula-Endolymph System with Morphological Parameters for the Axolotl (Ambystoma Tigrinum) Semicircular Canals
138 The Open Medical Informatics Journal, 2008, 2, 138-148 Open Access Mathematical Model of the Cupula-Endolymph System with Morphological Parameters for the Axolotl (Ambystoma tigrinum) Semicircular Canals Rosario Vega1, Vladimir V. Alexandrov2,3, Tamara B. Alexandrova1,3 and Enrique Soto*,1 1Instituto de Fisiología, Universidad Autónoma de Puebla, 2Facultad de Ciencias Físico Matemáticas, Universidad Autónoma de Puebla, 3 Lomonosov Moscow State University, Mexico Abstract: By combining mathematical methods with the morphological analysis of the semicircular canals of the axolotl (Ambystoma tigrinum), a system of differential equations describing the mechanical coupling in the semicircular canals was obtained. The coefficients of this system have an explicit physiological meaning that allows for the introduction of morphological and dynamical parameters directly into the differential equations. The cupula of the semicircular canals was modeled both as a piston and as a membrane (diaphragm like), and the duct canals as toroids with two main regions: i) the semicircular canal duct and, ii) a larger diameter region corresponding to the ampulla and the utricle. The endolymph motion was described by the Navier-Stokes equations. The analysis of the model demonstrated that cupular behavior dynamics under periodic stimulation is equivalent in both the piston and the membrane cupular models, thus a general model in which the detailed cupular structure is not relevant was derived. Keywords: Inner ear, vestibular, hair cell, transduction, sensory coding, physiology. 1. INTRODUCTION linear acceleration detectors, and the SCs as angular accel- eration detectors, notwithstanding that both sensory organs The processing of sensory information in the semicircular are based on a very similar sensory cell type. -
Central Auditory Function Evaluation to Diagnose Central Auditory Processing Disorder Product Applicability
bmchp.org | 888-566-0008 wellsense.org | 877-957-1300 Medical Policy Central Auditory Function Evaluation to Diagnose Central Auditory Processing Disorder Policy Number: OCA 3.82 Version Number: 17 Version Effective Date: 01/01/21 + Product Applicability All Plan Products Well Sense Health Plan ∆ Boston Medical Center HealthNet Plan ∆ Well Sense Health Plan MassHealth ACO MassHealth MCO Qualified Health Plans/ConnectorCare/Employer Choice Direct Senior Care Options Notes: + Disclaimer and audit information is located at the end of this document. ∆ As required by state regulations and/or benefit coverage, different Plan definitions are specified for BMC HealthNet Plan products and Well Sense Health Plan products. See the applicable Definitions section for the Plan member. Policy Summary The evaluation of central auditory functioning to diagnose central auditory processing disorder (CAPD) is considered medically necessary for an adult or pediatric member when applicable Plan criteria are met. The evaluation is medically necessary when it is not part of a member’s individualized education plan (IEP) when one is appropriate for the member, it is a covered benefit for the member, and the Plan’s medical criteria are met (as specified in the Medical Policy Statement section of this Plan policy). Prior authorization is required for Plan covered services. See the member’s applicable benefit document available at www.bmchp.org for a member enrolled in a BMC HealthNet Plan product or Central Auditory Function Evaluation to Diagnose Central Auditory Processing Disorder + Plan refers to Boston Medical Center Health Plan, Inc. and its affiliates and subsidiaries offering health coverage plans to enrolled members. -

Benign Paroxysmal Positional Vertigo (BPPV)
Patient Information Patient Information Benign Paroxysmal Positional Vertigo (BPPV) BPPV causes spinning dizziness (‘vertigo’) due to crystals in the inner ear breaking loose. The crystals are normally embedded in a jelly and when we move forwards and backwards, or up and down, in space they send our brain messages about where we are. If they become loose they can find their way into the wrong area and cause the sensation that we are moving when we are actually not – the result is a sudden feeling of spinning, usually set off by turning your head. What causes BPPV? Perhaps half of all cases of BPPV are "idiopathic" – they occur for no known reason. The most common identified cause of BPPV in people under fifty is a previous head injury. In older people the most common cause is ‘wear and tear’ of the vestibular (balance) system of the inner ear. Some people have a history of previous inner ear inflammation with a period of severe, prolonged dizziness. Diagnosing BPPV The diagnosis is made based on history, physical examination and sometimes with hearing or balance testing. Other diagnostic tests may be required: for example, a CT or MRI may be required for cases that don't fit the usual pattern. It is possible to have BPPV in both ears, which may make the diagnosis and treatment more challenging. How is BPPV Treated? BPPV is often described as ‘self-limiting’ because symptoms often subside or disappear without any medical treatment. Symptoms tend to wax and wane. Physical manoeuvres and exercises are very effective in stopping your symptoms, and are the main basis of treatment. -

Tonic Tensor Tympani Syndrome (TTTS)
Tonic Tensor Tympani Syndrome (TTTS) http://www.dineenandwestcott.com.au/hyperacusis.php?fid=1 Retrieved 15ththth May 2009 In the middle ear, the tensor tympani muscle and the stapedial muscle contract to tighten the middle ear bones (the ossicles) as a reaction to loud, potentially damaging sound. This provides protection to the inner ear from these loud sounds. In many people with hyperacusis, an increased, involuntary activity can develop in the tensor tympani muscle in the middle ear as part of a protective and startle response to some sounds. This lowered reflex threshold for tensor tympani contraction is activated by the perception/anticipation of sudden, unexpected, loud sound, and is called tonic tensor tympani syndrome (TTTS). In some people with hyperacusis, it appears that the tensor tympani muscle can contract just by thinking about a loud sound. Following exposure to intolerable sounds, this heightened contraction of the tensor tympani muscle: • tightens the ear drum • stiffens the middle ear bones (ossicles) • can lead to irritability of the trigeminal nerve, which innervates the tensor tympani muscle; and to other nerves supplying the ear drum • can affect the airflow into the middle ear. The tensor tympani muscle functions in coordination with the tensor veli palatini muscle. When we yawn or swallow, these muscles work together to open the Eustachian tube. This keeps the ears healthy by clearing the middle ear of any accumulated fluid and allows the ears to “pop” by equalising pressure caused by altitude changes. TTTS can lead to a range of symptoms in and around the ear(s): ear pain; pain in the jaw joint and down the neck; a fluttering sensation in the ear; a sensation of fullness in the ear; burning/numbness/tingling in and around the ear; unsteadiness; distorted hearing. -

Endolymphatic Hydrops Meniere's
ENDOLYMPHATIC HYDROPS MENIERE’S DISEASE Introduction: Meniere’s Disease, or endolymphatic hydrops, is a disorder of the inner ear. This condition occurs because of abnormal fluctuations in the inner ear fluid called endolymph. A system of membranes, called the membranous labyrinth, contains a fluid called endolymph. This fluid bathes the inner ear balance and hearing system sensory cells and allows them to function normally. The membranes can become dilated like a balloon when pressure increases. This is called "hydrops". The amount of fluid is normally kept constant by altering the production and absorption of the fluid. Endolymph also contains a specific concentration of sodium, potassium, chloride, and other electrolytes. If the inner ear is damaged by disease, injury, or other causes, the volume and composition of the inner ear fluid can fluctuate with changes in the body’s fluid and electrolyte levels. This fluctuation in inner ear fluid can cause the symptoms of hydrops, including pressure or fullness of the affected ear, tinnitus, hearing loss, and imbalance or dizziness. Treatment of this condition is geared towards stabilizing the body fluid levels so that fluctuations in the endolymph volume can be avoided. Meniere's episodes may occur in clusters in which several attacks may occur within a short period of time. On the other hand, years may pass between episodes. Between the acute attacks, most people are free of symptoms or note mild imbalance, tinnitus, and/or hearing loss. Meniere’s affects roughly 0.2% of the population, about 200 out of 100,000 people (or in other words, 2/1000).