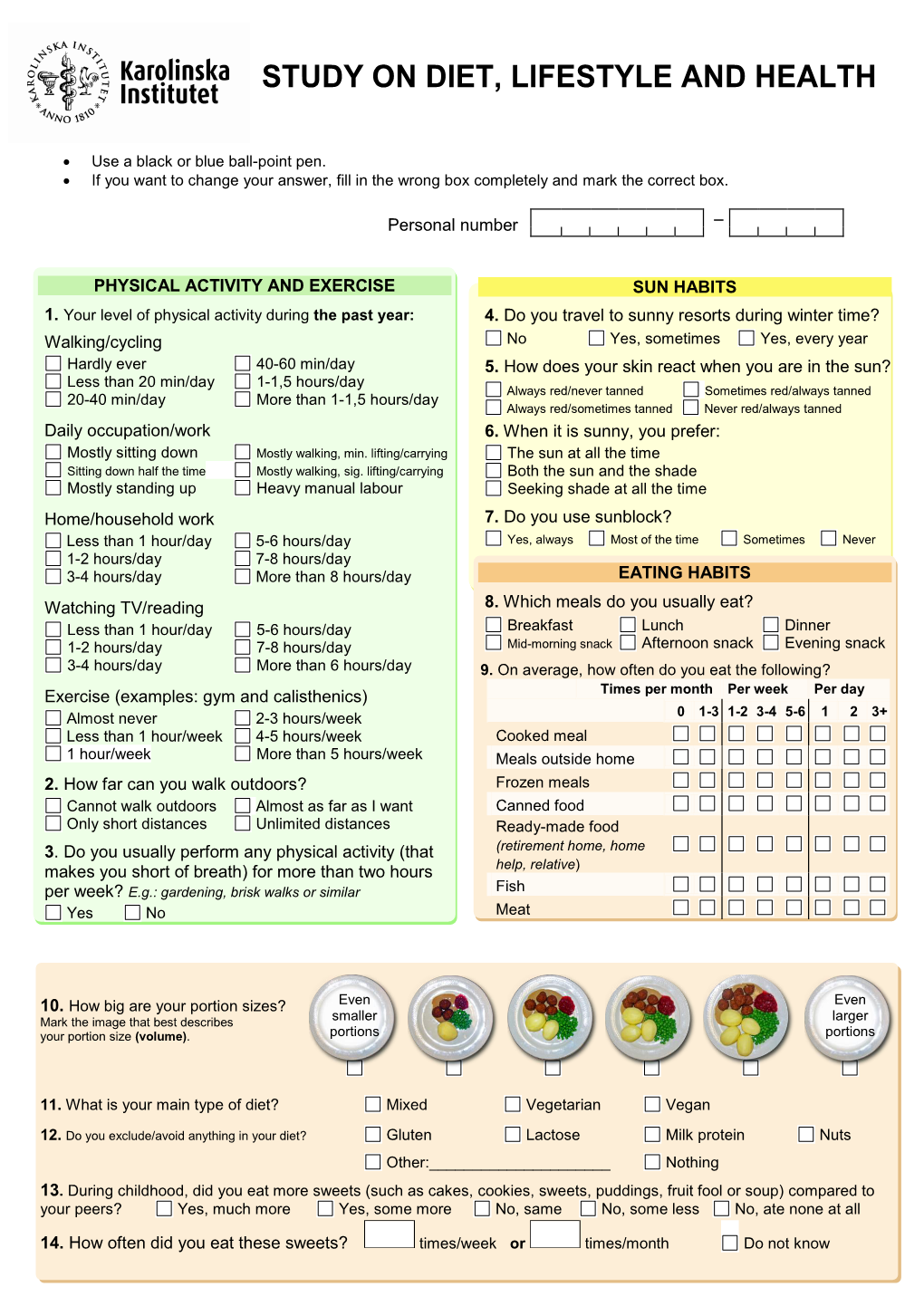
Lifestyle Questionnaire
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Contested Food
Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Social Sciences 89 Contested Food The Construction of Home and Consumer Studies as a Cultural Space KARIN HÖIJER ACTA UNIVERSITATIS UPSALIENSIS ISSN 1652-9030 ISBN 978-91-554-8712-6 UPPSALA urn:nbn:se:uu:diva-204458 2013 Dissertation presented at Uppsala University to be publicly examined in BMC C2:301, Husargatan 3, Uppsala, Friday, September 20, 2013 at 13:15 for the degree of Doctor of Philosophy. The examination will be conducted in English. Abstract Höijer, K. 2013. Contested Food: The Construction of Home and Consumer Studies as a Cultural Space. Acta Universitatis Upsaliensis. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Social Sciences 89. 101 pp. Uppsala. ISBN 978-91-554-8712-6. Education about and for the home has been part of the Swedish education system for over one hundred years, and Home and Consumer Studies (HCS) has been compulsory for all pupils since the common nine-year school system was introduced in 1962. For all this time food has been a central theme, however we know very little of what food means in this context. The aim of this thesis was to seek to understand the construction of food in HCS. This thesis consists of four papers that explore food in HCS from the perspective of teachers and pupils, the role of the classroom and how food in HCS is part of a larger cultural context. Observations and focus group interviews were used to collect data. The material consists of field notes from 13 days in three HCS classrooms and transcripts of focus group interviews with 25 HCS-teachers and 20 pupils. -

Catalog-1.Pdf
VÄLJ KÖTT FRÅN DESSA LÄNDER VÄLJ KÖTT FRÅN DESSA LÄNDER ? EU SVERIGE EU SVERIGE USA BRASILIEN USA BRASILIEN AUSTRALIEN ARGENTINA AUSTRALIEN ARGENTINA URUGUAY URUGUAY OXFILÉ ENTRECOTÉ RYGGBIFF OXBRINGA NÖTFÄRS OXKIND FRANSYSKA ROSTBIFF HÖGREV NÖTLEVER OXTUNGA SKIVAD BIFF (WOK) NÖT YTTERLÅR NÖT INNANLÅR FLANKSTEK SKIVAD ENTRECOTE (WOK) SKIVAD OXSVANS KÖTTFÄRSKÖTT NÖTRULLE NÖT GRYTBITAR STRIMLAD NÖT OXLÄGG NÖT TALG BOGSTEK 1 2 VÄLJ KÖTT FRÅN DESSA LÄNDER VÄLJ KÖTT FRÅN DESSA LÄNDER SVERIGE SVERIGE HOLLAND HOLLAND KALVFILÈ KALVENTRECOTÈ KALVYTTERFILÈ KALV SPARERIBS SKIVAD KALVLÄGG KALVLEVER KALVFRANSYSKA KALVHÖGREV KALV YTTERLÅR KALVLÄGG KALV TRIMMING KALVFÄRS KALVINNANLÅR KALVROSTBIFF KALVGRYTBITAR KALVRULLE KALVBRINGA KALVTUNGA KALVRACKS KALVRIBS KALVKOTLETTER KALVBEN KALVKIND SKIVAD KALVSVANS 3 4 VÄLJ KÖTT FRÅN DESSA LÄNDER VÄLJ KÖTT FRÅN DESSA LÄNDER SVERIGE IRLAND SVERIGE IRLAND SPANIEN NYA ZEELAND SPANIEN NYA ZEELAND AUSTRALIEN Finns även fårkött AUSTRALIEN LAMMYTTERFILÈ LAMMINNERFILÉ LAMMRACKS LAMMGRYTBITAR LAMMFÄRS LAMMLÄGG LAMMROSTBIFF LAMMKARRÉ LAMMSTEK BENFRI LAMMHJÄRTA LAMMTALG LAMMTUNGA LAMMKOTLETTER ENKLA LAMMKOTLETTER DUBBLA LAMMBOG LAMMLEVER LAMMNJURE LAMMTARM LAMMBRINGA LAMMSTEK MED BEN LAMMNACKE SKIVAD LAMMBAKLÄGG HEL LAMM LAMM MAGE 5 6 VÄLJ KÖTT FRÅN DESSA LÄNDER VÄLJ KÖTT FRÅN DESSA LÄNDER SVERIGE TYSKLAND SVERIGE DENMARK ESTLAND NYA ZEELAND FLÄSKFILÉ UTAN HUVUD FLÄSKFILÉ MED HUVUD FLÄSKYTTERFILÉ RÖKT HJORTSTEK RULLE HJORTSTEK HJORTINNANLÅR FLÄSKKARRE REVBENSSPJÄLL TUNNA REVBENSSPJÄLL HJORTINNERFILÉ HJORTYTTERFILÉ HJORTRACKS -

Of Council Regulation (EEC) No 2082/92 on Certificates of Specific Character
C 78/16EN Official Journal of the European Communities 10.3.2001 Publication of an application for registration pursuant to the second subparagraph of Article 8(1) of Council Regulation (EEC) No 2082/92 on certificates of specific character (2001/C 78/08) This publication confers the right to object to the application pursuant to Articles 8 and 9 of the abovementioned Regulation. Any objection to the application must be submitted via the competent authority in the Member State concerned within a time limit of five months from the date of this publication. Supporting arguments for publication are set out below, in particular under points 4.2, 4.3 and 4.4, and are considered to justify the application within the meaning of Regulation (EEC) No 2082/92. COUNCIL REGULATION (EEC) No 2082/92 APPLICATION FOR REGISTRATION OF A CERTIFICATE OF SPECIFIC CHARACTER National application No: 1 1. Competent authority Name: Statens livsmedelsverk, Address: Box 622, S-751 26 Uppsala Tel. (46-18) 17 55 00 Fax (46-18) 10 58 48. 2. Applicant group 2.1. Name: Swedish Meats ek för., Köttbranschens Riksförbund 2.2. Address: 121 86 Johanneshov, Box 5093, S-121 16 Johanneshov 2.3. Composition: producer/processor (x) other ( ). 3. Type of product: Meat products (cooked, salted, smoked, etc.) class 1.2. 4. Summary of product specification (Summary of requirements under Article 6(2)) 4.1. Name: Falukorv. 4.2. Specific production or manufacturing method Raw materials raw or salted beef, horsemeat or pork with rind removed. Such meat is defined as skeletal muscle including the naturally adherent fatty tissue and ligaments from which larger tendons have been removed. -

Sortimentskatalog Nr9 2021 LR.Pdf
SORTIMENT NR 9 Innehåll Fisk och skaldjur 6 - 15 Potatis 64 “Hela företaget genomsyras Fågel 16 - 21 Svamp 65 Kött 22 - 40 Pasta 66 - 71 avFredrik Svanberg, kärleken grundare till mat” Egen produktion 41 - 45 Bröd och bakverk 72 - 75 Vilt 46 - 47 Mejeri och ost 76 - 79 Chark 48 - 61 Olja och vinäger 80 - 82 Frukt och bär 62 Skafferi 83 - 91 Grönsaker 63 Om oss 92 - 93 Saknar du något? Vi på Gourmet Food utvecklar hela tiden sortimentet tillsammans med våra kunder. Tveka inte att höra av dig till oss om det är något du saknar. Tillgången av varor kan variera beroende på säsong och efterfrågan. Vissa varor kan behöva anskaffas med viss ledtid, prata med din säljare. 4 FISK FÄRSK FISK FÄRSK LAXFILÉ BENFRI Salmo salar, odlad, skuren av 4/5-lax, 1,4-1,8 kg/st, endast hel kartong FRÖYA LAXLOIN FÄRSK NORGE Färdiga skinn- och benfria loin av lax, endast 02145 CA 13 KG/KRT backloin, sashimikvalitet, ca 400 g/st KOLJAFILÉ FÄRSK NORGE Melanogrammus aeglefinus, skinn 02116 CA 5 KG/KRT och benfri, MSC-certifierad FÄRSK NORGE 02080 5 KG/KRT FISK FÄRSK ART.NR VARUSLAG/BESKRIVNING VIKT/ST VIKT/KRT LAXFILÉ, BENFRI 02130 1,4-1,8 kg ca 13 kg Salmo salar, odlad, vakuumpaketerad, Norge SEJFILÉ 02300 145 g+ 5 kg Pollachius virens, MSC-certifierad, Norge När blir torsken skrei? Visste du att... SEJTAILS, SKINN- OCH BENFRI VARJE ÅR UNDER PERIODEN 02399 100-200 g 5 kg januari till april vandrar torsken från Barents Av omkring en halv miljard skrei Pollachius virens, MSC-certifierad, Norge hav ner till nordnorska kusten för att leka. -

Delsbo Charkuteri Tilldelades Guld I Chark SM 2010 I Klassen Isterband
Chark-SM 2010 l 2010 Chark-SM 2010 l Chark-SM 2010 l Chark-SM 2010 l Chark-SM 2010 Kött ,Br a n s c h e 28 OKTOBERn Chark–SM 2010 Resultaten & alla vinnarna!!! Här hittar du resultaten för varje kategori: Sidan 1. Falukorv 4 2. Köttbullar 4 3. Julskinka (kokt) 4 4. Hela köttprodukter, kokta 6 5. Hela köttprodukter, rökta 6 6. Lufttorkade/kallrökta, hela köttprodukter 8 7. Varmrökt småkorv, smal 8 8. Varmrökt småkorv, tjock 10 9. Skinnfri korv (hot dog, kryddkorv) 11 10. Grova emulsionsprodukter 12 11. Isterband 12 12. Kallrökt korv, vattenaktivitet under 0,9 12 13. Kallrökt korv, vattenaktivitet över 0,9 14 14. Pastej/sylta 14 15. Innovativa produkter 15 16. Ekologiska produkter 15 Foto: Anna Sigge Svenska Mästarna – Chark-SM 2010 Klass 1: Falukorv Klass 5: Helköttsprodukter, rökta Jägarfalukorv Samiskt rökt skinka Scan AB Jokkmokks Korv & Rökeri Tidigare bondeägda Scan AB ingår numera i den finska HKScan- Jokkmokks Korv & Rökeri grundades 1945 av smålänningen och koncernen som är ett av norra Europas största livsmedelsföretag inom charkuteristen Johan Wilhelm Johansson. I produktsortimentet finns kött, chark och färdigmat. Scan AB omsätter 11 Mdr SEK och har ca bland annat falukorvar av olika slag samt vedrökta och lavarökta skin- 3000 medarbetare. Huvudkontoret ligger i Stockholm och produk- kor. Omsättningen var 2009 cirka 23 miljoner kronor, vd är Magnus tionsanläggningar finns i bland annat Kristianstad, Linköping och Qvickström. www.jokkmokkskorv.se Skara. www.scan.se Klass 2: Köttbullar Klass 6: Lufttorkade kallrökta, hela Köttbullar Svenska Favoriter NyhlénsHugosons tyrolerskinka Värmlands Chark AB NyhlénsHugosons Chark AB Värmlands Chark AB är ett nystartat dotterbolag till Konsum Värm- NyhlénsHugosons startade 2005 och ägs till 51 procent av Mikael Hu- land. -

Resultaten & Alla Medaljerna!!!
Chark-SM 2012 l 2010 Chark-SM 2012 l Chark-SM 2012 l Chark-SM 2012 l Chark-SM 2012 En tidning utgiven av Kött och Chark- företagen (KCF) Grundad 1943 Specialutgåva Chark-SM 2012 Chark–SM 2012 Här hittar du resultaten för varje kategori: Sidan 1. Falukorv 4 2. Köttbullar 4 3. Julskinka (kokt) 4 4. Kokta helköttsprodukter 5 5.Rökta helköttsprodukter 6 6. Lufttorkade/kallrökta, hela köttprodukter 8 7. Smal småkorv 8 8. Tjock småkorv 9 9. Skinnfri korv 10 Resultaten & 10. Traditionella charkprodukter 11 11. Isterband 12 12. Kallrökt, torkad korv 12 13. Rökt påläggskorv 13 14. Pastej/sylta 14 alla medaljerna!!! 15. Innovativa produkter 15 16. Ekologiska produkter Foto: Anna16 Sigge FOTO ANNA SIGGE Vi är Svenska Mästare i chark 2012! Klass 1: Falukorv Klass 5: Rökta helköttsprodukter Jokkmokks Rökt sidfläsk Original Falu Nässjö Chark AB Jokkmokks Korv & Rökeri AB www.nassjochark.se www.jokkmokkskorv.se Klass 6: Lufttorkade/kallrökta Klass 2: Köttbullar hela köttprodukter Köttbullar Bjärhus luft- Helmut Walch Charkuteri AB torkade karré www.walch.se Bjärhus Gårdsbutik HB www.bjarhus.se Klass 3: Julskinka (kokt) Julskinka av rapsgris Klass 7: Smal småkorv Kosackenwurst Scan AB www.scan.se Helmut Walch Charkuteri AB www.walch.se Klass 4: Kokta helköttsprodukter Högrev Barbeque Klass 8: Tjock småkorv Sous Vide Puszta Signal & Anderssons Wurstmaster AB Charkuterifabrik AB www.signal-andersson.com www.wurstmaster.se Kött & Chark - enda tidningen i sitt slag! 2 Kött&Chark Kött&Chark Logotyper Kött&Chark. För tidningen. Fristående. Vi är Svenska Mästare -

Carbon Footprint of Retail Food Wastage
Carbon footprint of retail food wastage a case study of six Swedish retail stores Katharina Scholz Institutionen för energi och teknik Independent thesis 2013:05 Department of Energy and Technology ISSN 1654-9392 Uppsala 2013 SLU, Sveriges lantbruksuniversitet SUAS, Swedish University of Agricultural Sciences Institutionen för energi och teknik Department of Energy and technology English title: Carbon footprint of retail food wastage – a case study of six Swedish retail stores Author: Katharina Scholz Main supervisor: Mattias Eriksson; Swedish University of Agricultural Sciences Co-supervisor: Prof. Dr. Joachim Müller, Dr. Wolfram Spreer; University of Hohenheim Examiner: Dr. Ingrid Strid; Swedish University of Agricultural Sciences Credits: 30.0 hp Name of course: Independent Project in Environmental Science – Master’s thesis Course code: EX0431 Program: EnvEuro – European Master in Environmental Science Serial title: Independent thesis 2013:05 ISSN 1654-9392 Uppsala 2013 Keywords: food waste, carbon footprint, LCA, environmental impact, GHG emissions, supermarket Abstract Globally, about 1.3 billion tons of food are wasted every year. Besides economic, ethic and social aspects, food wastage bears a considerable environmental burden. The production of food causes greenhouse gases (GHG) at all stages along the food supply chain. Especially for animal products, the agricultural stage is crucial with CH4 and N2O emissions being of major importance. Agriculture was estimated to be the cause of 10-12 % of global anthropogenic GHG emissions and 15 % of production related emissions at EU level. Other steps like processing and transportation of food also cause GHG emissions. Therefore, wasting food not only means that resources are wasted but also that GHG emissions have been caused in vain. -

Chark-SM 2016 Har Nu Avgjorts Och För Nionde Gången Har Branschen Utsett Sveriges Bästa Charkuterier
2016 chark sm Chark-SM 2016 har nu avgjorts och för nionde gången har branschen utsett Sveriges bästa charkuterier. Cirka 750 produkter från cirka 61 företag har i år gjort upp om titeln Svensk Mästare i 16 olika klasser och hedersutmärkelser till klimatanpassade och ekologiska charkuterier. Tidning- en Kött & Chark presenterar som enda tidning hela listan. TEXT BO LINDMARK FOTO FARAMARZ GOSHEH 24 VINJETT Och motiveringen lyder... ”En otraditionell falukorv med hög ”En härlig, mustig korv med en god köttkvalitet. Tydlig rökfärg, tät struktur köttsmak och varm hetta. Med en fläkt och fast konsistens. Tydlig nötköttssmak, från Centraleuropa blir den en höjdare på tydlig röksmak.” grillen.” _Jokkmokks Korv: _Tulip Food Comany AB: Tulip Pusta Jokkmokks Korv Basturökt ”En korv klädd i bacon som (genast) sätter ”En rund fin köttbulle med en väl balanse- fart på smaklökarna.” SVENSK MÄSTARE rad smak som, dessutom är allergenfri.” _Lindvalls Chark: I VARJE KLASS ÄR _HKScan: Mamma Scan Bacon Wrapped Sausage ////////////////////////////////////////////////////// ”En vacker skinka med perfekt avvägning ”Klassiskt hantverk med hög kvalitet, bra mellan sälta, sötma och en bra saftighet. balans mellan sälta och syra, lagom rök- FALUKORV En riktigt God Julskinka!” smak. En fulländad smakupplevelse.” _ Jokkmokks Korv: Jokkmokks Korv _Björk & Co: Julskinka, kokt _Wiktor Ohlssons: Isterband Basturökt KÖTTBULLAR OCH HAMBURGARE ”En ny innovativ produkt med fräsch och ”Med stor kunskap och noggrannhet välbalanserad smak där smaksättaren har man skapat detta vackra hantverk. _HKScan: Mamma Scan spelar huvudrollen. En klar vinnare!” Resultatet blev en salami med en frisk _Direkt Chark: Sparrisskinka färg och aromatisk smak. Helt enkelt en JULSKINKA vinnarsalami.” _Björk & Co: Julskinka, kokt ”En bra förädlad styckningsdetalj. -

COLLAGEN NIPPI & FIBRAN / PRODUCT GUIDE 2019 USA EN Viskoteepak Contents
COLLAGEN NIPPI & FIBRAN / PRODUCT GUIDE 2019 USA EN ViskoTeepak Contents. in brief. ViskoTeepak history ________________________ 4 ViskoTeepak locations ______________________ 5 ViskoTeepak is one of the biggest Strategic values ___________________________ 6 manu facturers of fibrous, cellulose and Company culture __________________________ 7 plastic casings in the world, and we Collagen _________________________________ 8 have production plants, converting fa- Nippi edible collagen casing _________________ 8 cilities and technical support offices Nippi R-type _____________________________ 10 worldwide. We're also proud to have Nippi T, T3 and K-type _____________________ 13 the industry's largest business-partner Nippi F-type _____________________________ 14 network, through which our products Nippi NF ________________________________ 17 are offered in nearly 100 countries. Nippi product offering _____________________ 18 Fibran non-edible collagen casing ____________20 Our newly built head office (ViskoTeepak Holding Ab), which opened in May 2018, is located in Mariehamn, in Fibran S1 ________________________________ 22 Finland's Aland Islands. In Europe, we have fibrous and Fibran NF _______________________________ 22 cellulose production plants in Lommel (Belgium) and Hanko (Finland). Additionally, we have a plastic-casing Fibran Color offering ______________________ 24 production plant in Nuevo Laredo (Mexico). Our convert- ViskoTepeak product portfolio _______________ 25 ing facilities are located in Delfzijl (Netherlands), Brno (Czech Republic) and Kenosha (Wisconsin, USA). Our ViskoTeepak principles and guiding values _____ 26 sales offices are in Moscow, Hamburg and Mexico City. ViskoTeepak is owned by the Eriksson Capital Group, based in Mariehamn, Finland. Eriksson Capital is a pri- vately owned investment company with a focus on small to medium-size high-tech industrial companies operat- ing in the global marketplace. -

The Importance of Diet for Uptake of Phthalates in Pregnant Women
The importance of diet for uptake of phthalates in pregnant women Kostens betydelse för upptag av ftalater hos gravida kvinnor Anna Roos Fakulteten för hälsa, natur och teknikvetenskap Folkhälsovetenskap Examensarbete i folkhälsovetenskap I (magister) 15 HP Handledare: Carl-Gustaf Bornehag, Huan Shu Examinator: Carl-Gustaf Bornehag 2017-05-24 SAMMANFATTNING Bakgrund: Kemikalier med hormonstörande egenskaper (Endocrine Disruptor Chemicals) – EDCs, är ämnen som kan påverka det naturliga hormonsystemet hos människor och djur. Ftalater är industriproducerade kemikalier, flera av dem med misstänkt hormonstörande egenskaper. Ftalater är vanligt förekommande i många olika typer av produkter. De sprids till sin omgivning och förorenar miljön. De finns även i livsmedel. Genom att mäta biomarkörer i urin, blod, bröstmjölk och fostervatten kan man konstatera att både gravida kvinnor och foster är exponerade för ftalater. Detta är av stor oro då man vet att fosterstadiet är den period i livet då exponering för kemikalier med hormonstörande egenskaper är som mest kritiskt, på grund av negativa hälsoeffekter. Syfte: Syftet med studien är att undersöka hur intag av mejeriprodukter, fett, kött och fisk påverkar urinnivåer av ftalater hos gravida kvinnor. Metod: Urinprov analyserade för innehåll av ftalater från 1,670 kvinnor deltagande i SELMA-studien har använts för statistisk analys, tillsammans med enkätsvar angående kostvanor besvarade av de 1,670 kvinnorna i vecka 25 av graviditeten. Resultat: Mejeriprodukter och fett: Kostintag av grädde, standardmjölk, färskost, margarin för matlagning, majonnäs och flytande margarin hade signifikant samband med högre nivåer av mono-n-butyl ftalat (MnBP) och mono-benzyl ftalat (MBzP) i urinen hos gravida kvinnor. Kött: Ett kostintag av bacon och påläggskorv hade significant samband med högre nivåer av mono-n-butyl ftalat (MnBP) och mono-benzyl ftalat MBzP) i urinen hos gravida kvinnor. -

Geografiska Ursprungsbeteckningar Och Landsbygdsutveckling I EU
SLI-SKRIFT 2006:1 Geografiska Ursprungsbeteckningar och landsbygdsutveckling i EU Livsmedelsekonomiska Carina Folkeson Livsmedelsekonomiska institutet KORT OM SLI Livsmedelsekonomiska institutet (SLI) är en analysmyndighet med uppdrag att utföra kvalificerade ekonomiska analyser inom jordbruks-, livsmedels- och fiskeområdet. Kärnan i institutets verksamhetsområde är EU:s gemensamma jordbrukspolitik, med betoning på reformbehovet och på effektiviteten i olika styrmedel, samt jordbruks- och livsmedelsfrågornas hantering dels vid en utvidgning av EU, dels i WTO- förhandlingarna. Alla publikationer från SLI kan beställas kostnadsfritt på institutets hemsida på www.sli.lu.se Livsmedelsekonomiska institutet Box 730 220 07 Lund http:www.sli.lu.se Carina Folkeson SLI-skrift 2006:1 ISSN 1651-4742 Tryckt av MCT/Rahms i Malmö, 2006 2 INNEHÅLLSFÖRTECKNING 1 INLEDNING 7 1.1 Ämnet 7 1.2 Syfte och avgränsning 8 1.3 Skriftens disposition 8 2 GEOGRAFISKA URSPRUNGSBETECKNINGAR – HISTORIA, UTBREDNING OCH FÖRDELNING 9 2.1 Historia 9 2.2 Global fördelning av GU-produkter 12 3 TEORI BAKOM GEOGRAFISKA URSPRUNGSBETECKNINGAR 14 3.1 Immaterialrättsfamiljen 15 3.2 Varuteori 17 3.3 Samband mellan landsbygdsutveckling och Geografiska Ursprungsbeteckningar 19 3.4 Sammanfattning 21 4 VÄRLDSHANDELSORGANISATIONEN OCH TRIPS-AVTALET 21 4.1 GU-produkternas WTO-historia 21 4.2 Vad debatteras i Doha-rundan? 22 4.3 Kort beskrivning av de olika positionerna i GU-frågan 23 5 EU OCH GEOGRAFISKA URSPRUNGSBETECKNINGAR 26 5.1 Syftet med CAP samt målsättningen med reformerna 26 5.2 -
Mise En Page 1
The official quality and origin signs Appellation d’origine contrôlée AOC A guarantee of quality linked to a“ terroir” Protected designation of origin PDO The European equivalent guarantee Protected geographical indication PGI A guarantee of the link between a product and its géographical origin Traditional speciality guaranteed TSG A guarantee of the traditional character of a product Agriculture biologique A guarantee of quality linked to a type of production protective of environment Organic farming The European equivalent guarantee Label rouge LR A guarantee that the product is of superior quality The policy on the quality and origin of agricultural and agrifood products implemented by the Agriculture Ministry is a longstanding one. It was first applied more than a century ago. The French scheme guiding the application of that policy is linked into the European system put in place in 1991 and 1992. It was deeply modified by the French Agricultural Reform Law of 5 January 2006 in order: •to offer consumers a comprehensive and clear view of the whole of the French and European system for official recognition of quality in agricultural and agrifood products; •to enhance the credibility of that official recognition by strengthening the guarantee given by govern- ment and the checks that underpin the system’s legitimacy; •to allow producers and economic actors to extract more value from their products. Signs identifying product quality and origin A government guarantee A guarantee of quality linked to origin • AOC and PDO: the guarantee of quality deriving from a “terroir” . • PGI: the guarantee of quality deriving from a link between the product and the geographical area in which it has been produced .