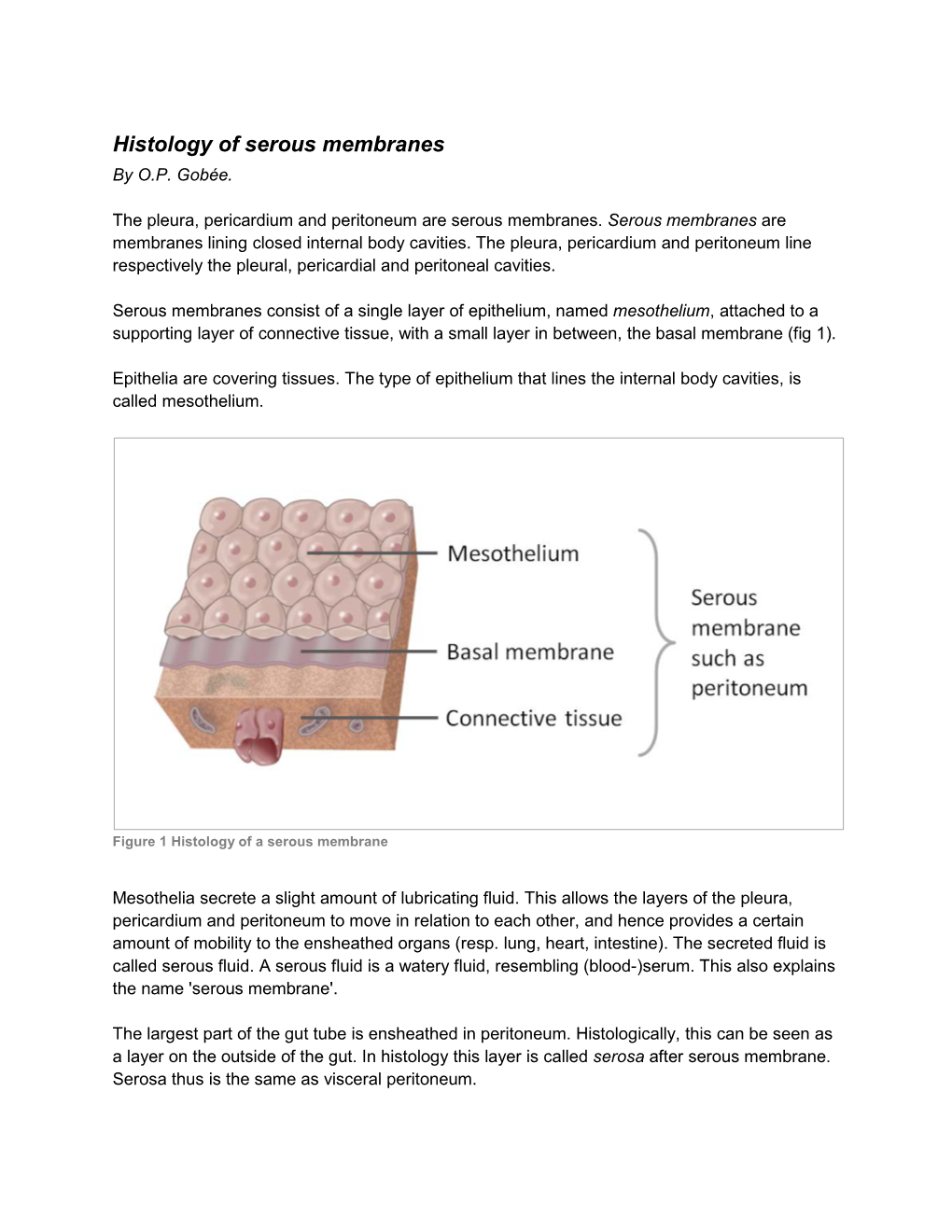
Histology of Serous Membranes by O.P
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Physiology H Digestive
2/28/18 Introduction • Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends Digestive System at the anus • Digestive functions are initiated by the parasympathetic division Chapter 29 - Digestion occurs during periods of low activity - Produces more energy than it uses Copyright © 2016 by Elsevier Inc. All rights reserved. 1 Copyright © 2016 by Elsevier Inc. All rights reserved. 2 Anatomy The Digestive System • Oral cavity • Pharynx • Esophagus • Stomach • Small intestine and large intestine • Accessory organs: Pancreas, liver, and gallbladder From Herlihy B: The human body in health and illness, ed 4, St. Louis, 2011, Saunders. Copyright © 2016 by Elsevier Inc. All rights reserved. 3 Copyright © 2016 by Elsevier Inc. All rights reserved. 4 Physiology Gastrointestinal Tract • Ingestion: Taking materials into mouth by • Muscular tube throughout digestive system eating/drinking • Accessory organs and glands secrete • Digestion: Breaking down food into molecules substance to aid in digestion that can be used by the body • GI tract wall has four layers: - Includes mechanical and enzymatic action - Mucosa • Absorption: Simple molecules from the - Submucosa gastrointestinal (GI) tract move into the - Muscle layer: Responsible for peristalsis bloodstream or lymph vessels and then into - Serosa body cells • Defecation: Eliminating indigestible or unabsorbed material from the body Copyright © 2016 by Elsevier Inc. All rights reserved. 5 Copyright © 2016 by Elsevier Inc. All rights reserved. 6 1 2/28/18 Peristalsis Oral Cavity • First portion of GI tract • Contains: - Teeth - Tongue - Openings for salivary glands From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St. -

Carcinomatous Cirrhosis of the Liver with Sarcomatosis of the Peritoneum 1
CARCINOMATOUS CIRRHOSIS OF THE LIVER WITH SARCOMATOSIS OF THE PERITONEUM 1 S. SANES, M.D., AND K. TERPLAN, M.D. (From tile Pathological Laboratory of the Buffalo General Hospital and School of Medicine, University of Buffalo) The following case is reported because of the occurrence of two different types of malignant neoplasm with typical portal cirrhosis of the liver. That a pathogenetic relationship exists between Laennec's cirrhosis and primary carcinoma of the liver is generally recognized. Whether the association of a peritoneal sarcoma with the cirrhosis in this case was more than a coincidence seemed an interesting point for discussion. REPORT OF CASE E. G., 11 white Italian male fifty-seven years old, was admitted to the Buffalo General Hospital on the service of Drs. N. G. Russell and A. H. Aaron, Nov. 25, 1934. He died Nov. 29, 1934. All his adult life he had partaken of large amounts of wine and whiskey daily. At the age of seventeen years he had suffered an attack of jaundice of several weeks' duration. The patient first began to lose weight and strength in 1932 and noticed that his skin was becoming dark. In March 1934 he complained of cramp-like abdominal pain, diarrhea, and bloating. The stools were watery. There was no nausea or vomiting. Upon hos pitalization, April 9, 1934, physical examination revealed that the pupils reacted to light and accommodation. The chest was emphysematous; breath sounds were diminished in both bases. The heart was regular; a systolic murmur was heard. The blood pressure was 118/70. The liver and spleen were palpable three finger breadths below the costal margin. -

7) Anatomy of OMENTUM
OMENTUM ANATOMY DEPARTMENT DR.SANAA AL-SHAARAWY Dr. Essam Eldin Salama OBJECTIVES • At the end of the lecture the students must know: • Brief knowledge about peritoneum as a thin serous membrane and its main parts; parietal and visceral. • The peritonial cavity and its parts the greater sac and the lesser sac (Omental bursa). • The peritoneal folds : omenta, mesenteries, and ligaments. • The omentum, as one of the peritonial folds • The greater omentum, its boundaries, and contents. • The lesser omentum, its boundaries, and contents. • The omental bursa, its boundaries. • The Epiploic foramen, its boundaries. • Mesentery of the small intestine, and ligaments of the liver. • Nerve supply of the peritoneum. • Clinical points. The peritoneum vIs a thin serous membrane, §Lining the wall of the abdominal and pelvic cavities, (the parietal peritoneum). §Covering the existing organs, (the visceral peritoneum). §The potential space between the two layers is the peritoneal cavity. Parietal Visceral The peritoneal Cavity vThe peritoneal cavity is the largest one in the body. vDivisions of the peritoneal cavity : §Greater sac; extends from Lesser Sac diaphragm down to the pelvis. §Lesser sac; lies behind the stomach. §Both cavities are interconnected through the epiploic foramen. §In male : the peritoneum is a closed sac . §In female : the sac is not completely closed because it Greater Sac communicates with the exterior through the uterine tubes, uterus and vagina. The peritoneum qIntraperitoneal and Intraperitoneal viscera retroperitoneal organs; describe the relationship between various organs and their peritoneal covering; §Intraperitonial structure; which is nearly totally covered by visceral peritoneum. §Retroperitonial structure; lies behind the peritoneum, and partially covered by visceral peritoneum. -

E Pleura and Lungs
Bailey & Love · Essential Clinical Anatomy · Bailey & Love · Essential Clinical Anatomy Essential Clinical Anatomy · Bailey & Love · Essential Clinical Anatomy · Bailey & Love Bailey & Love · Essential Clinical Anatomy · Bailey & Love · EssentialChapter Clinical4 Anatomy e pleura and lungs • The pleura ............................................................................63 • MCQs .....................................................................................75 • The lungs .............................................................................64 • USMLE MCQs ....................................................................77 • Lymphatic drainage of the thorax ..............................70 • EMQs ......................................................................................77 • Autonomic nervous system ...........................................71 • Applied questions .............................................................78 THE PLEURA reections pass laterally behind the costal margin to reach the 8th rib in the midclavicular line and the 10th rib in the The pleura is a broelastic serous membrane lined by squa- midaxillary line, and along the 12th rib and the paravertebral mous epithelium forming a sac on each side of the chest. Each line (lying over the tips of the transverse processes, about 3 pleural sac is a closed cavity invaginated by a lung. Parietal cm from the midline). pleura lines the chest wall, and visceral (pulmonary) pleura Visceral pleura has no pain bres, but the parietal pleura covers -

The Digestive System
69 chapter four THE DIGESTIVE SYSTEM THE DIGESTIVE SYSTEM The digestive system is structurally divided into two main parts: a long, winding tube that carries food through its length, and a series of supportive organs outside of the tube. The long tube is called the gastrointestinal (GI) tract. The GI tract extends from the mouth to the anus, and consists of the mouth, or oral cavity, the pharynx, the esophagus, the stomach, the small intestine, and the large intes- tine. It is here that the functions of mechanical digestion, chemical digestion, absorption of nutrients and water, and release of solid waste material take place. The supportive organs that lie outside the GI tract are known as accessory organs, and include the teeth, salivary glands, liver, gallbladder, and pancreas. Because most organs of the digestive system lie within body cavities, you will perform a dissection procedure that exposes the cavities before you begin identifying individual organs. You will also observe the cavities and their associated membranes before proceeding with your study of the digestive system. EXPOSING THE BODY CAVITIES should feel like the wall of a stretched balloon. With your skinned cat on its dorsal side, examine the cutting lines shown in Figure 4.1 and plan 2. Extend the cut laterally in both direc- out your dissection. Note that the numbers tions, roughly 4 inches, still working with indicate the sequence of the cutting procedure. your scissors. Cut in a curved pattern as Palpate the long, bony sternum and the softer, shown in Figure 4.1, which follows the cartilaginous xiphoid process to find the ventral contour of the diaphragm. -

The Formation of Peritoneal Adhesions
THE FORMATION OF PERITONEAL ADHESIONS Christian DellaCorte, Ph.D., C.M.T. The increased incidence of postoperative adhesions and their complications has focused attention on trying to understand the adhesion, adhesion formation, clinical consequences, and prevention of adhesion formation. Adhesions are highly differentiated, formed through an intricate process involving a complex organ, the peritoneum, whose surface lining is the key site in adhesion formation. The peritoneum, a serous membrane, serves a protective function for the contents of the abdominal cavity. Homeostasis is maintained by allowing exchange of molecules and production of peritoneal fluid. This provides an environment for optimal function of intra-abdominal organs. Forms of trauma to the peritoneum (i.e., mechanical, thermal, chemical, infectious, surgical, and/or ischemic) can result in the formation of peritoneal adhesions. In 1919, it was shown that peritoneal healing differed from that of skin. When the peritoneal membrane is traumatized, a dynamic response results that produces a series of steps toward rapid regeneration in approximately five to seven days of the injured peritoneum via re-epithelialization, irrespective of the size of injury. Microscopic studies showed the new peritoneal cells are derived from mesodermal cells of the underlying granulation tissue, multipotent mesenchymal cells that are able to take the form of fibroblasts or mesothelial cells. When a defect is made in the parietal peritoneum the entire surface becomes simultaneously epithelialized, differing from the gradual epidermalization from the borders as is found in skin wounds. Multiplication and migration of mesothelial cells from the margins of the wound may play a small part in the regenerative process, but it does not play a major role. -

Latin Language and Medical Terminology
ODESSA NATIONAL MEDICAL UNIVERSITY Department of foreign languages Latin Language and medical terminology TextbookONMedU for 1st year students of medicine and dentistry Odessa 2018 Authors: Liubov Netrebchuk, Tamara Skuratova, Liubov Morar, Anastasiya Tsiba, Yelena Chaika ONMedU This manual is meant for foreign students studying the course “Latin and Medical Terminology” at Medical Faculty and Dentistry Faculty (the language of instruction: English). 3 Preface Textbook “Latin and Medical Terminology” is designed to be a comprehensive textbook covering the entire curriculum for medical students in this subject. The course “Latin and Medical Terminology” is a two-semester course that introduces students to the Latin and Greek medical terms that are commonly used in Medicine. The aim of the two-semester course is to achieve an active command of basic grammatical phenomena and rules with a special stress on the system of the language and on the specific character of medical terminology and promote further work with it. The textbook consists of three basic parts: 1. Anatomical Terminology: The primary rank is for anatomical nomenclature whose international version remains Latin in the full extent. Anatomical nomenclature is produced on base of the Latin language. Latin as a dead language does not develop and does not belong to any country or nation. It has a number of advantages that classical languages offer, its constancy, international character and neutrality. 2. Clinical Terminology: Clinical terminology represents a very interesting part of the Latin language. Many clinical terms came to English from Latin and people are used to their meanings and do not consider about their origin. -

Anatomy and Physiology of the Bowel and Urinary Systems
PMS1 1/26/05 10:52 AM Page 1 Anatomy and Physiology of the Bowel and 1 Urinary Systems Anthony McGrath INTRODUCTION The aim of this chapter is to increase the reader’s under- standing of the small and large bowel and urinary system as this will enhance their knowledge base and allow them to apply this knowledge when caring for patients who are to undergo stoma formation. LEARNING OBJECTIVES By the end of this chapter the reader will have: ❏ an understanding of the anatomy and physiology of the small and large bowel; ❏ an understanding of the anatomy and physiology of the urinary system. GASTROINTESTINAL TRACT The gastrointestinal (GI) tract (Fig. 1.1) consists of the mouth, pharynx, oesophagus, stomach, duodenum, jejunum, small and large intestines, rectum and anal canal. It is a muscular tube, approximately 9m in length, and it is controlled by the autonomic nervous system. However, while giving a brief outline of the whole system and its makeup, this chapter will focus on the anatomy and physiology of the small and large bowel and the urinary system. The GI tract is responsible for the breakdown, digestion and absorption of food, and the removal of solid waste in the form of faeces from the body. As food is eaten, it passes through each section of the GI tract and is subjected to the action of various 1 PMS1 1/26/05 10:52 AM Page 2 1 Anatomy and Physiology of the Bowel and Urinary Systems Fig. 1.1 The digestive system. Reproduced with kind permission of Coloplast Ltd from An Introduction to Stoma Care 2000 2 PMS1 1/26/05 10:52 AM Page 3 Gastrointestinal Tract 1 digestive fluids and enzymes (Lehne 1998). -

Human Anatomy and Physiology
LECTURE NOTES For Nursing Students Human Anatomy and Physiology Nega Assefa Alemaya University Yosief Tsige Jimma University In collaboration with the Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education 2003 Funded under USAID Cooperative Agreement No. 663-A-00-00-0358-00. Produced in collaboration with the Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education. Important Guidelines for Printing and Photocopying Limited permission is granted free of charge to print or photocopy all pages of this publication for educational, not-for-profit use by health care workers, students or faculty. All copies must retain all author credits and copyright notices included in the original document. Under no circumstances is it permissible to sell or distribute on a commercial basis, or to claim authorship of, copies of material reproduced from this publication. ©2003 by Nega Assefa and Yosief Tsige All rights reserved. Except as expressly provided above, no part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without written permission of the author or authors. This material is intended for educational use only by practicing health care workers or students and faculty in a health care field. Human Anatomy and Physiology Preface There is a shortage in Ethiopia of teaching / learning material in the area of anatomy and physicalogy for nurses. The Carter Center EPHTI appreciating the problem and promoted the development of this lecture note that could help both the teachers and students. -

The Mesocolon a Histological and Electron Microscopic Characterization of the Mesenteric Attachment of the Colon Prior to and After Surgical Mobilization
ORIGINAL ARTICLE The Mesocolon A Histological and Electron Microscopic Characterization of the Mesenteric Attachment of the Colon Prior to and After Surgical Mobilization Kevin Culligan, MRCS,∗ Stewart Walsh, FRCSEd,∗ Colum Dunne, PhD,∗ Michael Walsh, PhD,† Siobhan Ryan, MB,‡ Fabio Quondamatteo, MD,‡ Peter Dockery, PhD,§ and J. Calvin Coffey, FRCSI∗¶ uring fetal development, the dorsal mesentery suspends the en- Background: Colonic mobilization requires separation of mesocolon from tire gastrointestinal tract from the posterior abdominal wall. The underlying fascia. Despite the surgical importance of planes formed by these D mesocolon is the adult remnant of that part of the dorsal mesentery structures, no study has formally characterized their microscopic features. associated with the colon.1 In the adult human, the transverse and The aim of this study was to determine the histological and electron micro- lateral sigmoid portions of the mesocolon are mobile whereas the as- scopic appearance of mesocolon, fascia, and retroperitoneum, prior to and cending, descending, and medial sigmoid portions are nonmobile and after colonic mobilization. attached to underlying retroperitoneum.2–4 Classic anatomic teaching Methods: In 24 cadavers, samples were taken from right, transverse, de- maintains that the ascending and descending mesocolon “disappear” scending, and sigmoid mesocolon. In 12 cadavers, specimens were stained during embryogenesis.5,6 In keeping with this, the identification of a with hematoxylin and eosin (3 sections) or Masson trichrome (3 sections). In right or left mesocolon in the adult is frequently depicted as anoma- the second 12 cadavers, lymphatic channels were identified by staining im- lous rather than accepted as an anatomic norm.7 Accordingly, the munohistochemically for podoplanin. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -

ABDOMINOPELVIC CAVITY and PERITONEUM Dr
ABDOMINOPELVIC CAVITY AND PERITONEUM Dr. Milton M. Sholley SUGGESTED READING: Essential Clinical Anatomy 3 rd ed. (ECA): pp. 118 and 135141 Grant's Atlas Figures listed at the end of this syllabus. OBJECTIVES:Today's lectures are designed to explain the orientation of the abdominopelvic viscera, the peritoneal cavity, and the mesenteries. LECTURE OUTLINE PART 1 I. The abdominopelvic cavity contains the organs of the digestive system, except for the oral cavity, salivary glands, pharynx, and thoracic portion of the esophagus. It also contains major systemic blood vessels (aorta and inferior vena cava), parts of the urinary system, and parts of the reproductive system. A. The space within the abdominopelvic cavity is divided into two contiguous portions: 1. Abdominal portion that portion between the thoracic diaphragm and the pelvic brim a. The lower part of the abdominal portion is also known as the false pelvis, which is the part of the pelvis between the two iliac wings and above the pelvic brim. Sagittal section drawing Frontal section drawing 2. Pelvic portion that portion between the pelvic brim and the pelvic diaphragm a. The pelvic portion of the abdominopelvic cavity is also known as the true pelvis. B. Walls of the abdominopelvic cavity include: 1. The thoracic diaphragm (or just “diaphragm”) located superiorly and posterosuperiorly (recall the domeshape of the diaphragm) 2. The lower ribs located anterolaterally and posterolaterally 3. The posterior abdominal wall located posteriorly below the ribs and above the false pelvis and formed by the lumbar vertebrae along the posterior midline and by the quadratus lumborum and psoas major muscles on either side 4.