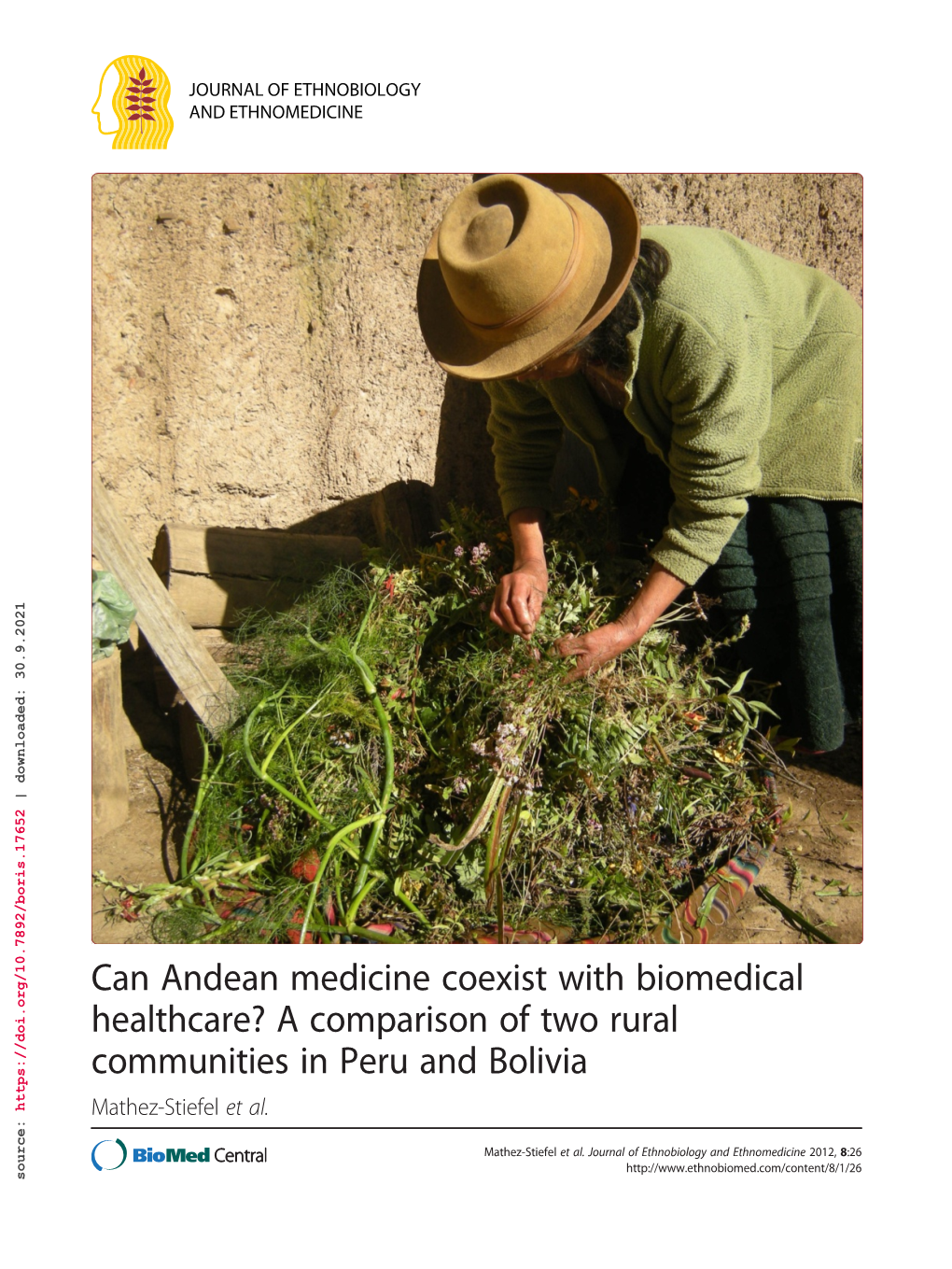
Can Andean Medicine Coexist with Biomedical Healthcare?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Culturally Appropriate Information, Education and Communication Strategies for Improving Adolescent Reproductive Health in Cusco, Peru Marco Florez-Arestegui Cornejo
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Population Council: Knowledge Commons Population Council Knowledge Commons Reproductive Health Social and Behavioral Science Research (SBSR) 2004 Culturally appropriate information, education and communication strategies for improving adolescent reproductive health in Cusco, Peru Marco Florez-Arestegui Cornejo Rosalinda Barreto Silva Follow this and additional works at: https://knowledgecommons.popcouncil.org/ departments_sbsr-rh Part of the Demography, Population, and Ecology Commons, Gender and Sexuality Commons, International Public Health Commons, Maternal and Child Health Commons, and the Public Health Education and Promotion Commons Recommended Citation Florez-Arestegui Cornejo, Marco and Rosalinda Barreto Silva. 2004. "Culturally appropriate information, education and communication strategies for improving adolescent reproductive health in Cusco, Peru," FRONTIERS Final Report. Washington, DC: Population Council. This Report is brought to you for free and open access by the Population Council. Culturally Appropriate Information, Education and Communication Strategies for Improving Adolescent Reproductive Health in Cusco, Peru Marco Flórez-Aréstegui Cornejo and Rosalinda Barreto Silva Comunicación Andina May 2004 This study was funded by the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT (USAID) under the terms of Cooperative Agreement Number HRN- A-00-98-00012-00 and Population Council Subagreement number AI00.27A. The opinions expressed herein are those of the author and do not necessarily reflect the views of USAID. Executive Summary The project Culturally Appropriate Information, Education and Communication Strategies for Improving Adolescent Reproductive Health in Cusco, Peru was designed in response to the evident lack of information and education on adolescent reproductive health in the country and, in particular, in the rural areas of the department of Cusco. -

LIBRO DE RESUMENES VIII SEMANA(1).Pdf
UNIVERSIDAD NACIONAL DE SAN ANTONIO ABAD DEL CUSCO [ VICERRECTORADO DE INVESTIGACIÓN YACHAYNINCHIS WIÑARINANPAQ Para que nuestro conocimiento crezca Comité editorial: DIRECTOR : Dr. Gilbert Alagón Huallpa INTEGRANTES : Dra. Victoria Puente de la Vega Aparicio Dr. Walter Antezana Julian Mg. Anahí Karina Cardona Rivero Mg. Miguel Ángel Mendoza Abarca DISEÑO Y DIAGRAMACIÓN: Br. Eveling Rodriguez Zelaya IMPRESIÓN: Editorial Universitaria: VicerrectoradodeInvestigación Av. De la Cultura N° 733 Junio, 2020 Páginas:77 Tiraje: 100 Los artículos son de responsabilidad exclusiva de los autores. © 2020, UNIVERSIDAD NACIONAL DE SAN ANTONIO ABAD DEL CUSCO VICERRECTORADO DE INVESTIGACIÓN Av. De la Cultura N° 733 – Pabellón “A” 2do. Piso VRIN - 2do. Piso Pabellón A. Ciudad Universitaria de Perayoq 084-222512/ 084-232398 Anexo 1543 - 1545 [email protected] Enlace: vrin.unsaac.edu.pe Hecho el Depósito Legal en la Biblioteca Nacional del Perú N.° 978-612-4236-25-9 Queda hecho el depósito que establece la Ley N° 28377, Ley N° 29165 y D.S. N°017-38 COMITÉ ORGANIZADOR DE LA VIII SEMANA Dr. Gilbert Alagón Huallpa VICERRECTOR DE INVESTIGACIÓN DIRECCIONES DEL VICERRECTORADO DE INVESTIGACIÓN Dr. Walter Orestes Antezana Julian DIRECTOR DE GESTIÓN DE LA INVESTIGACIÓN Mgt. Anahí Karina Cardona Rivero DIRECTORA DE INNOVACIÓN Y TRANSFERENCIA Mgt. Miguel Ángel Mendoza Abarca DIRECTOR DE EMPRENDIMIENTO Y GESTIÓN Dra. Victoria Puente de la Vega Aparicio DIRECTORA DEL CONSEJO DE UNIDADES DE INVESTIGACIÓN María Amalia Villavicencio Llerena JEFE ADMINISTRATIVO DEL VICERRECTORADO -
Viewees Who Donated Their Time and Knowledge to the Dissertation Research
SSStttooonnnyyy BBBrrrooooookkk UUUnnniiivvveeerrrsssiiitttyyy The official electronic file of this thesis or dissertation is maintained by the University Libraries on behalf of The Graduate School at Stony Brook University. ©©© AAAllllll RRRiiiggghhhtttsss RRReeessseeerrrvvveeeddd bbbyyy AAAuuuttthhhooorrr... Selling Sacred Cities: Tourism, Region, and Nation in Cusco, Peru A Dissertation Presented by Mark Charles Rice to The Graduate School in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in History Stony Brook University May 2014 Copyright by Mark Rice 2014 Stony Brook University The Graduate School Mark Charles Rice We, the dissertation committee for the above candidate for the Doctor of Philosophy degree, hereby recommend acceptance of this dissertation. Paul Gootenberg – Dissertation Advisor SUNY Distinguished Professor, History, Stony Brook University Eric Zolov – Chairperson of Defense Associate Professor, History, Stony Brook University Brooke Larson Professor, History, Stony Brook University Deborah Poole Professor, Anthropology, Johns Hopkins University This dissertation is accepted by the Graduate School Charles Taber Dean of the Graduate School ii Abstract of the Dissertation Selling Sacred Cities: Tourism, Region, and Nation in Cusco, Peru by Mark Charles Rice Doctor of Philosophy in History Stony Brook University 2014 It is hard to imagine a more iconic representation of Peru than the Inca archeological complex of Machu Picchu located in the Cusco region. However, when US explorer, Hiram Bingham, announced that he had discovered the “lost city” in 1911, few would have predicted Machu Picchu’s rise to fame during the twentieth century. My dissertation traces the unlikely transformation of Machu Picchu into its present-day role as a modern tourism destination and a representation of Peruvian national identity. -

Pos(ICRC2019)631
High Altitude Sites for Astroparticle Observatories in Peru Jose Bellido∗ The University of Adelaide, Australia E-mail: [email protected] PoS(ICRC2019)631 Andres Romero-Wolf Jet Propulsion Laboratory, California Institute of Technology, USA E-mail: [email protected] Rolando Perca Gonzales, Jose Vega Ramirez Universidad Nacional de San Agustín de Arequipa, Perú E-mail: [email protected], [email protected] Sayri Garcia Roca, Marco Zamalloa Universidad Nacional San Antonio Abad del Cusco, Perú E-mail: [email protected], [email protected] Jorge Samanes, Luis Otiniano Comisión Nacional de Investigación y Desarrollo Aeroespacial del Perú E-mail: [email protected], [email protected] Walter Guevara Day Facultad de Ciencias Físicas, Universidad Mayor de San Marcos, Perú E-mail: [email protected] Fabian Schüssler IRFU, CEA, Université Paris-Saclay, F-91191 Gif-sur-Yvette, France E-mail: [email protected] Samridha Kunwar Max-Planck-Institut für Kernphysik, Saupfercheckweg 1, D-69117 Heidelberg, Germany E-mail: [email protected] This paper describes four high altitude sites in southern Peru that were visited, in March 2019, by members of the SGSO Alliance (currently the SWGO Collaboration). The sites are located above 4000 m.a.s.l. with access to water resources and are located between 1 to 4 hours drive from the closest airport. Peruvian authorities, local populations and universities offer support and encourage international collaborations to consider these sites for Astroparticle Observatories. 36th International Cosmic Ray Conference -ICRC2019- July 24th - August 1st, 2019 Madison, WI, U.S.A. -
Variations in Social Organization of Textile Production at the Household Level : Adaptive Strategies of Guatemalan and Peruvian
VARIATIONS IN SOCIAL ORGANIZATION OF TEXTILE PRODUCTION AT THE HOUSEHOLD LEVEL: ADAPTIVE STRATEGIES OF GUATEMALAN AND PERUVIAN HIGHLAND ARTISANS Linda L. Chalmers B.A., Simon Fraser University THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS in the Department of Sociology and Anthropology @ Linda L. Chalmers 1985 SIMON FRASER UNIVERSITY March, 1985 All rights reserved. This work may not be reproduced in whole or in part, by photocopy or other means, without permission of the author. APPROVAL NAME : Linda L. Chalmers DEGREE : Master of Arts TITLE OF THESIS: Variations in Social Organization of Textile Production at the Household Level: Adaptive Strategies of Guatemalan and Peruvian Highland Artisans EXAMINING COMMITTEE: Chairman: Ian Whi taker MARILYN GATES SENIOR SUPERVISOR - --. - 1 8 MARY LEE STEARNS I I -- / PHILIP WAGNER EXTERNAL EXAKINER Dept. of Geography Simon Fraser University DATE APPROVED: March 27, 1985 PARTIAL COPYRIGHT LICENSE I hereby grant to Simon Fraser University the right to lend my thesis, project or extended essay (the title of which is shown below) to users of the Simon Fraser University Library, and to make partial or single copies only for such users or in response to a request from the library of any other university, or other educational institution, on its own behalf or for one of its users. I further agree that permission for multiple copying of this work for scholarly purposes may be granted by me or the Dean of Graduate Studies. It is understood that copying or pub1 ication of this work for financial gain shall not be allowed without my written permission. -
Moving Away from Silence: Music of the Peruvian Altiplano and the Experiment of Urban Migration / Thomas Turino
MOVING AWAY FROM SILENCE CHICAGO STUDIES IN ETHNOMUSICOLOGY edited by Philip V. Bohlman and Bruno Nettl EDITORIAL BOARD Margaret J. Kartomi Hiromi Lorraine Sakata Anthony Seeger Kay Kaufman Shelemay Bonnie c. Wade Thomas Turino MOVING AWAY FROM SILENCE Music of the Peruvian Altiplano and the Experience of Urban Migration THE UNIVERSITY OF CHICAGO PRESS Chicago & London THOMAS TURlNo is associate professor of music at the University of Ulinois, Urbana. The University of Chicago Press, Chicago 60637 The University of Chicago Press, Ltd., London © 1993 by The University of Chicago All rights reserved. Published 1993 Printed in the United States ofAmerica 02 01 00 99 98 97 96 95 94 93 1 2 3 4 5 6 ISBN (cloth): 0-226-81699-0 ISBN (paper): 0-226-81700-8 Library of Congress Cataloging-in-Publication Data Turino, Thomas. Moving away from silence: music of the Peruvian Altiplano and the experiment of urban migration / Thomas Turino. p. cm. - (Chicago studies in ethnomusicology) Discography: p. Includes bibliographical references and index. I. Folk music-Peru-Conirna (District)-History and criticism. 2. Folk music-Peru-Lirna-History and criticism. 3. Rural-urban migration-Peru. I. Title. II. Series. ML3575.P4T87 1993 761.62'688508536 dc20 92-26935 CIP MN @) The paper used in this publication meets the minimum requirements of the American National Standard for Information Sciences-Permanence of Paper for Printed Library Materials, ANSI 239.48-1984. For Elisabeth CONTENTS List of Illustrations ix Acknowledgments xi Introduction: From Conima to Lima -

Religious Murals of Colonial Peru
Conversations: An Online Journal of the Center for the Study of Material and Visual Cultures of Religion (mavcor.yale.edu) Collection - Painting Beyond the Frame: Religious Murals of Colonial Peru Ananda Cohen-Suarez Fig. 1 Mateo Pérez de Alesio or follower, Cupola murals, funerary chapel of Captain Bernardo Vil- legas, Church of La Merced, Lima, early 17th century. Photo by author. Mural painting was a longstanding artistic practice in the Andean region of South America, stretching back to at least the third millennium BCE. Numerous coastal cultures of Peru, including the Cupisnique, Moche, and Chimú civilizations, produced stunning polychrome murals that decorated both the interiors and exteriors of religious temples and residences. Their iconography was diverse, including mythological scenes, representations of deities, and sacrificial rituals. Fewer mural remains are found at highland sites due to preservation issues, but traces of mural decoration can be found at the pre-Columbian sites of Raqchi and Quispiguanca, among others. Mural paintings frequently possessed iconographic and stylistic resemblances to portable media such as ceramics, textiles, and metalwork. These large-scale public works of art broadcast religious ideologies, mythologies, and cultural values to their constituents, serving as an important conduit for the transmission of knowledge and belief systems. Conversations: An Online Journal of the Center for the Study of Material and Visual Cultures of Religion (mavcor.yale.edu) With the Spanish invasion and colonization of Peru in the 1530s, the visual arts played an integral role in the religious indoctrination of indigenous and Afro-descendant communities to Catholicism. Mural painting in particular became a favored medium in early evangelization efforts because of its relatively low cost and shorter execution time in comparison to multimedia pieces such as retablos (altarpieces) and polychrome sculptures. -

Museum GUIDE 1
The Pedro de Osma Museum GUIDE 1 4 5 The Pedro de Osma Museum GUIDE ACKNOWLEDGMENTS PEDRO AND ANGÉLICA DE OSMA PEDRO DE OSMA MUSEUM GILDEMEISTER FOUNDATION Advisory Council Audience Management Assistant The Pedro de Osma Museum guide was Daniel Chero Ramírez made possible by the generous spon- Board of Trustees Felipe de Osma Berckemeyer sorship of Los Portales S.A. and the Cecilia Alayza de Losada President Guides institutional alliance with Country Club Felipe de Osma Berckemeyer Armando Andrade de Lucio Andrea Narro Taco Lima Hotel. Alfonso Castrillón Vizcarra Giovanna Sembrero Huaranga Vice President CEO Ana María de Osma Ayulo María del Carmen de Reparaz Zamora Guillermo Velaochaga Raffo Ticket Office Ramón Mujica Pinilla Mabel Chipana Jordán Treasurer Business Manager - Hotels Nélida Huamaccto Zumaeta Diego Pedro de Osma Ayulo Eduardo Ibarra Rooth Director Pedro Pablo Alayza Tijero Secretary Oscar de Osma Berckemeyer CREDITS Assistant to The Director Chairperson Silvana Vargas-Machuca Barrantes Editor Martín Fariña Von Buchwald Pedro Pablo Alayza Tijero Communications Chairperson Naisha Vergara Diaz Editorial Coordinator R. Jorge Christopherson Petit Teresa Marcos Juez 8 9 Collections Management Chairperson Luis Adawi Schreiber Designer Fr. Piero Véliz Valencia Carmen Sifuentes Alba Catalogue Records General Manager Javier Chuquiray Garibay Texts Diego La Rosa Injoque Pedro Pablo Alayza Tijero Conservation and Restoration Carlos Trivelli Avila Coordinator Gemma Ballesteros Tejerizo Copy Editors Anaís Blanco Chávez Conservation and Restoration Elisa Granda Armas © 2019 Pedro and Angélica de Osma Consultant Luis Adawi Schreiber Gildemeister Foundation Av. Pedro de Osma 421, Barranco, Lima Álvaro Sandoval Espinola Translator Phone 01 467-0063 www.museopedrodeosma.org Conservation and Restoration Alessandra Pinasco García Miró © From the texts: the autors Assistant Printed by First edition, August 2019 / 750 copys Sandra Flores Goicochea Impresso Gráfica S.A. -

Re-Animating Andean Worlds
RE-ANIMATING ANDEAN WORLDS: KAMAYOQ, THE POLITICS OF ‘CULTURALLY APPROPRIATE’ KNOWLEDGE EXTENSION, AND ETHNODEVELOPMENT IN THE PERUVIAN ANDES by Julian Sebastian Yates B.A., University of Manchester, 2004 M.A., University of Victoria, 2009 A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY in THE FACULTY OF GRADUATE AND POSTDOCTORAL STUDIES (Geography) THE UNIVERSITY OF BRITISH COLUMBIA (Vancouver) April 2015 © Julian Sebastian Yates 2015 ABSTRACT This dissertation positions the kamayoq of the Southern Peruvian Andes (Sierra Sur) within the context of globalized ethnodevelopment networks. Contemporary kamayoq are indigenous, community-based specialists who act as “transcultural bridges” within a “culturally appropriate” methodology of campesino-a-campesino (farmer-to-farmer) knowledge transfer. Building on the results of a follow-the-thing methodology (deployed across fourteen months of multi-sited ethnographic fieldwork), I use the case of the kamayoq to develop a critique of ethnodevelopment – a notion that encapsulates how development programmes put culture and cultural groups to work in order both to incorporate them within broader development trajectories, and to protect them from some of the negative effects of such participation. I draw on – and contribute to – relevant debates in political economy, political ecology, development studies, and Andean studies to make a series of empirical and theoretical contributions. I conduct a Polanyian historical analysis of how the kamayoq have supported economic integration across different modes of production and forms of governance (since the fifteenth century). I develop a contemporary analysis of how ethnodevelopment programmes construct the kamayoq as ‘ethnic experts’ and ethno-entrepreneurial subjects within a new rural economy of Peru, thereby transforming a dynamic form of Andean learning-by-doing (aprender hacer) – as embodied by the kamayoq – into a form of ‘ethnic expertise’ on display (saber hacer). -

“From Machupicchu to Lake Titicaca”
Format for Proposals of Candidate Systems For The Globally-important Ingenious Agricultural Heritage Systems (GIAHS) Programme SUMMARY INFORMATION a. Country and location Perú, (Cusco-Puno) b. Project title / name of the system “From Machupicchu to Lake Titicaca” c. Funding requested ( five year project) d. Requesting agency GEF e. Governmental counterparts and other partners CONAM-(IMA-ANPE-ITDG-CARE) f. Summary (max. 200 words) The transect proposed as a site pilot under the GIAHS project, is located in the southern area of the Peruvian Andes and includes the environment around the sacred city of the Incas, Machu Picchu, (1900 m.), follows the whole Vilcanota river watershed up to the divortium aquarium in the Raya (4,300 m), crosses the northern part of the peruvian highplateau to reach lake Titicaca at 3,800 m (Map 1). Actual presence of traditional agricultural knowledge includes terraces, ridges fields, local irrigation systems and traditional agricultural tools, crops and livestock spread at different altitudes that goes from mesothermic areas at 2400 m. altitude called “Quechua” agroecological zone, with maize as the main crop, to the coldest environment used for the marginal cultivation of a great number of native crops and varieties including frost resistant crops as quinua, kañiwa and high altitude tubers (Table 1). Mostly native livestock is grazing the native pastures with llamas and alpacas at high altitudes over 4,300 m, in the so called “Puna” agroecological zone. Two main ethnic groups, the “quechuas” in Cuzco region and “aymaras” in southern Puno, have contributed to develop those endogenous local agriculture systems of production. Quechuas are located around the Cuzco area (the capital city of the former Inca empire) and the aymara of the former Tiahuanaco kingdom area around lake Titicaca. -

Connor King 502 Thesis Final
Using diatoms preserved in peat deposits to track environmental changes in the Cordillera Vilcanota, Peru Connor P. King Student Number: 20032567 An undergraduate thesis submitted to the School of Environmental Studies in partial fulfillment of the requirements for the degree of Bachelor of Science (Honours) Queen’s University Kingston, Ontario, Canada Supervised by Dr. John Smol Examined by Dr. Brian Cumming April 2020 2 Abstract Recent climate change in alpine regions is outpacing many other parts of the world, threatening to degrade specialized ecosystems and their associated ecological services. Long- term data are sparse, especially in remote regions such as the Cordillera Vilcanota in Peru. Diatoms preserved in peat deposits (known locally as bofedales) have the potential to provide a long-term context for environmental changes resulting from recent climate change. This thesis examined diatom assemblages and other siliceous indicators preserved in a 90 cm peat core to reveal long-term environmental changes spanning the past several centuries. The diatom assemblages indicate that cool, oligotrophic conditions occurred contemporaneously with peat initiation at the end of the Little Ice Age, and that these conditions persisted until the late 20th century, at which point drier conditions became prevalent. Recently, the diatoms indicate a shift to wetter and more acidic conditions that are characteristic of a poor fen. These changes may reflect glacial retreat due to climate change or ENSO events, the latter of which is known to modulate precipitation in the western tropical Andes. This research also tracked peat accumulation rates that are amongst the highest in the world, highlighting the important role these environments play in carbon sequestration. -
Jonathan Alderman Phd Thesis
THE PATH TO ETHNOGENESIS AND AUTONOMY: KALLWAYA- CONSCIOUSNESS IN PLURINATIONAL BOLIVIA Jonathan Alderman A Thesis Submitted for the Degree of PhD at the University of St Andrews 2016 Full metadata for this item is available in Research@StAndrews:FullText at: http://research-repository.st-andrews.ac.uk/ Please use this identifier to cite or link to this item: http://hdl.handle.net/10023/8600 This item is protected by original copyright This item is licensed under a Creative Commons Licence The Path to Ethnogenesis and Autonomy: Kallawaya- consciousness in Plurinational Bolivia Jonathan Alderman This thesis is submitted in partial fulfilment for the degree of PhD at the University of St Andrews 2016 1 The Path to Ethnogenesis and Autonomy: Kallawaya-consciousness in Plurinational Bolivia Kallawaya Autonomy Assembly meeting 24th March 2012 2 Declarations 1. Candidate’s declarations: I, …Jonathan Alderman…, hereby certify that this thesis, which is approximately …80,000.. words in length, has been written by me, and that it is the record of work carried out by me, or principally by myself in collaboration with others as acknowledged, and that it has not been submitted in any previous application for a higher degree. I was admitted as a research student in September 2009 and as a candidate for the degree of phd Social Anthropology..…. in Octpber 2010; the higher study for which this is a record was carried out in the University of St Andrews between 2010 and 2015. (If you received assistance in writing from anyone other than your supervisor/s): I, …..., received assistance in the writing of this thesis in respect of [language, grammar, spelling or syntax], which was provided by …… Date …… signature of candidate ……… 2.