A Rare Arterial Branch Distributing to the Thymus, Ectopic Intrathymic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Superior Laryngeal Nerve Identification and Preservation in Thyroidectomy
ORIGINAL ARTICLE Superior Laryngeal Nerve Identification and Preservation in Thyroidectomy Michael Friedman, MD; Phillip LoSavio, BS; Hani Ibrahim, MD Background: Injury to the external branch of the su- recorded and compared on an annual basis for both be- perior laryngeal nerve (EBSLN) can result in detrimen- nign and malignant disease. Overall results were also com- tal voice changes, the severity of which varies according pared with those found in previous series identified to the voice demands of the patient. Variations in its ana- through a 50-year literature review. tomic patterns and in the rates of identification re- ported in the literature have discouraged thyroid sur- Results: The 3 anatomic variations of the distal aspect geons from routine exploration and identification of this of the EBSLN as it enters the cricothyroid were encoun- nerve. Inconsistent with the surgical principle of pres- tered and are described. The total identification rate over ervation of critical structures through identification, mod- the 20-year period was 900 (85.1%) of 1057 nerves. Op- ern-day thyroidectomy surgeons still avoid the EBSLN erations performed for benign disease were associated rather than identifying and preserving it. with higher identification rates (599 [86.1%] of 696) as opposed to those performed for malignant disease Objectives: To describe the anatomic variations of the (301 [83.4%] of 361). Operations performed in recent EBSLN, particularly at the junction of the inferior con- years have a higher identification rate (over 90%). strictor and cricothyroid muscles; to propose a system- atic approach to identification and preservation of this Conclusions: Understanding the 3 anatomic variations nerve; and to define the identification rate of this nerve of the distal portion of the EBSLN and its relation to the during thyroidectomy. -

Larynx Anatomy
LARYNX ANATOMY Elena Rizzo Riera R1 ORL HUSE INTRODUCTION v Odd and median organ v Infrahyoid region v Phonation, swallowing and breathing v Triangular pyramid v Postero- superior base àpharynx and hyoid bone v Bottom point àupper orifice of the trachea INTRODUCTION C4-C6 Tongue – trachea In women it is somewhat higher than in men. Male Female Length 44mm 36mm Transverse diameter 43mm 41mm Anteroposterior diameter 36mm 26mm SKELETAL STRUCTURE Framework: 11 cartilages linked by joints and fibroelastic structures 3 odd-and median cartilages: the thyroid, cricoid and epiglottis cartilages. 4 pair cartilages: corniculate cartilages of Santorini, the cuneiform cartilages of Wrisberg, the posterior sesamoid cartilages and arytenoid cartilages. Intrinsic and extrinsic muscles THYROID CARTILAGE Shield shaped cartilage Right and left vertical laminaà laryngeal prominence (Adam’s apple) M:90º F: 120º Children: intrathyroid cartilage THYROID CARTILAGE Outer surface à oblique line Inner surface Superior border à superior thyroid notch Inferior border à inferior thyroid notch Superior horns à lateral thyrohyoid ligaments Inferior horns à cricothyroid articulation THYROID CARTILAGE The oblique line gives attachement to the following muscles: ¡ Thyrohyoid muscle ¡ Sternothyroid muscle ¡ Inferior constrictor muscle Ligaments attached to the thyroid cartilage ¡ Thyroepiglottic lig ¡ Vestibular lig ¡ Vocal lig CRICOID CARTILAGE Complete signet ring Anterior arch and posterior lamina Ridge and depressions Cricothyroid articulation -

Penetrating Carotid Artery: Uncommon Complex and Lethal Injuries
Eur J Trauma Emerg Surg (2011) 37:429–437 DOI 10.1007/s00068-011-0132-3 REVIEW ARTICLE Penetrating carotid artery: uncommon complex and lethal injuries J. A. Asensio • T. Vu • F. N. Mazzini • F. Herrerias • G. D. Pust • J. Sciarretta • J. Chandler • J. M. Verde • P. Menendez • J. M. Sanchez • P. Petrone • C. Marini Received: 16 June 2011 / Accepted: 19 June 2011 / Published online: 15 July 2011 Ó Springer-Verlag 2011 Abstract Carotid arterial injuries are the most difficult or occasionally via surgical cricothyroidotomy. Establish- and certainly the most immediately life-threatening injuries ing a surgical airway can be a difficult procedure given the found in penetrating neck trauma. Their propensity to bleed distortion of anatomic landmarks caused by hemorrhage. It actively and potentially occludes the airway and makes is also fraught with danger, as the incision may release the surgical intervention very challenging. Their potential for contained hematoma, resulting in torrential bleeding that causing fatal neurological outcomes demands that trauma can obscure the operative site and place the patient at risk surgeons exercise excellent judgment in the approach to for aspiration. These injuries incur high morbidity and their definitive management. The purpose of this article is mortality. Their neurologic sequelae can be devastating. to review the diagnosis and management of these injuries. Fortunately they are not common. Keywords Vascular Á Trauma Historical perspective Introduction The first documented case of the treatment of a cervical vascular injury is attributed to the French surgeon Ambrose Carotid arterial injuries are the most difficult and certainly Pare (1510–1590) [1], who was able to ligate the lacerated the most immediate life-threatening injuries found in carotid artery and a jugular vein of a wounded soldier. -

The Role of Strap Muscles in Phonation Laryngeal Model in Vivo
Journal of Voice Vol. 11, No. 1, pp. 23-32 © 1997 Lippincott-Raven Publishers, Philadelphia The Role of Strap Muscles in Phonation In Vivo Canine Laryngeal Model Ki Hwan Hong, *Ming Ye, *Young Mo Kim, *Kevin F. Kevorkian, and *Gerald S. Berke Department of Otolaryngology, Chonbuk National University, Medical School, Chonbuk, Korea; and *Division of Head and Neck Surgery, UCLA School of Medicine, Los Angeles, California, U.S.A. Summary: In spite of the presumed importance of the strap muscles on laryn- geal valving and speech production, there is little research concerning the physiological role and the functional differences among the strap muscles. Generally, the strap muscles have been shown to cause a decrease in the fundamental frequency (Fo) of phonation during contraction. In this study, an in vivo canine laryngeal model was used to show the effects of strap muscles on the laryngeal function by measuring the F o, subglottic pressure, vocal in- tensity, vocal fold length, cricothyroid distance, and vertical laryngeal move- ment. Results demonstrated that the contraction of sternohyoid and sternothy- roid muscles corresponded to a rise in subglottic pressure, shortened cricothy- roid distance, lengthened vocal fold, and raised F o and vocal intensity. The thyrohyoid muscle corresponded to lowered subglottic pressure, widened cricothyroid distance, shortened vocal fold, and lowered F 0 and vocal inten- sity. We postulate that the mechanism of altering F o and other variables after stimulation of the strap muscles is due to the effects of laryngotracheal pulling, upward or downward, and laryngotracheal forward bending, by the external forces during strap muscle contraction. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Chapter Anatomy
Chapter Anatomy 1 Kyriakos Anastasiadis and Chandi Ratnatunga Chapter Location of extensions of the upper lobes, as well as relationships to the innominate vein, have been described (Figs. 1.3). The thymus gland is located in the anterosuperior me- Thus, rather than being located in its classical anterior po- diastinum. It usually extends from the thyroid gland to sition, one or both of the upper lobe thymus may even lie the level of the fourth costal cartilage. It lies posterior to behind the innominate vein. Moreover, it has to be noted the pretracheal fascia, the sternohyoid and sternothyroid that besides the classical location of the gland, ectopic muscles and the sternum (mostly behind the manubrium thymic tissue could be found in the mediastinal fat of the and the upper part of its body). It is located anteriorly majority of patients. This is now accepted as the normal to the innominate vein and is found between the pari- etal pleura and extrapleural fat and central to the phrenic nerves. It lies on the pericardium, with the ascending aorta and aortic arch behind it, while in the neck it lies over the trachea. Parallel to the gland on each side lie the phrenic nerves, which converge towards the gland at its middle segment (particularly important issue in thymec- tomy procedures). The gland consists classically of two lobes, even though other lobular structures may be pres- ent (Figs. 1.1, 1.2). The thyrothymic ligament connects the upper parts of its lobes to the thyroid gland. A variety Fig. 1.2 Midline cervicothoracic sagittal section material de- monstrating the thymus gland location (1=thyroid isthmus, 2=superficial layer of cervical fascia, 3=pretracheal cervical fa- scia, 4=brachiocephalic trunk, 5=pretracheal space, 6=left bra- chiocephalic vein, 7=sternothyroid muscle, 8=anterior wall of Fig. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -
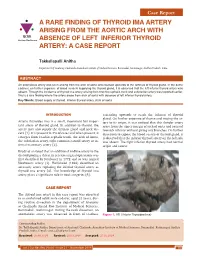
A RARE FINDING of THYROID IMA ARTERY ARISING from the AORTIC ARCH with IJCRR Section: Healthcare ABSENCE of LEFT INFERIOR THYROID ARTERY: a CASE REPORT
Case Report A RARE FINDING OF THYROID IMA ARTERY ARISING FROM THE AORTIC ARCH WITH IJCRR Section: Healthcare ABSENCE OF LEFT INFERIOR THYROID ARTERY: A CASE REPORT Takkallapalli Anitha Department of Anatomy, Chalmeda Anandrao Institute of Medical Sciences, Bommakal, Karimnagar, Andhra Pradesh, India. ABSTRACT An anomalous artery was seen arising from the arch of aorta and coursed upwards to the isthmus of thyroid gland. In the same cadaver, on further exposure of blood vessels supplying the thyroid gland, it is observed that the left inferior thyroid artery was absent. Though the incidence of thyroid ima artery arising from brachio cephalic trunk and subclavian artery was reported earlier, this is a rare finding where the artery arose from arch of aorta with absence of left inferior thyroid artery. Key Words: Blood supply of thyroid, Inferior thyroid artery, Arch of aorta INTRODUCTION ascending upwards to reach the isthmus of thyroid gland. On further exposure of thorax and tracing the ar- Arteria thyroidea ima is a small, inconstant but impor- tery to its origin, it was noticed that this slender artery tant artery of thyroid gland. In addition to thyroid, the arose from the upper margin of arch of aorta and coursed artery may also supply the thymus gland and neck vis- towards isthmus without giving any branches. On further cera [1]. It is present in 3% of cases and when present, it dissection to expose the blood vessels of thyroid gland, it emerges from brachio cephalic trunk, the arch of Aorta, is observed that the inferior thyroid artery on the left side the subclavian artery, right common carotid artery or in- was absent. -

Spontaneous Arteriovenous Malformations in the Cervical Area
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.3.303 on 1 June 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 303-309 Spontaneous arteriovenous malformations in the cervical area J. GREENBERG, M.D. From the Department of Neurology, Episcopal Hospital, Philadelphia, Pennsylvania 19125, U.S.A. SUMMARY Four patients with spontaneous arteriovenous malformations of cervical vessels have been presented. The embryology of these vessels has been discussed in order to suggest an ex- planation for the apparent difference in the incidence of arteriovenous malformations involving the internal carotid artery and those involving either the vertebral or the external carotid arteries. A fifth case (S.T.) is presented as a probable iatrogenic arteriovenous fistula and is to be added to the steadily growing reports of this phenomenon. Trauma is the most common cause of arteriovenous had sustained a minor injury to the posterior aspect communications between the blood vessels in of the right ear. Routine skull films at the time did not the cervical area (Aronson, 1961). Iatrogenic reveal a fracture, and there was no evidence of local Protected by copyright. deep tissue injury noted. fistulae occurring after carotid or vertebral angio- On the present admission, a slight prominence of the graphy are being reported with regularity in the right retroauricular region was noted and a thrill and recent literature (Sutton, 1962). Spontaneous mal- bruit were present. The bruit could be obliterated by formations in this area also occur. Thus far, eight local pressure. cases have been reported involving the vertebral The neurological examination was within normal vessels (Norman, Schmidt, and Grow, 1950; limits. -
Study on Branching Pattern of Aortic Arch in Indian
Original Article http://dx.doi.org/10.5115/acb.2012.45.3.203 pISSN 2093-3665 eISSN 2093-3673 Study on branching pattern of aortic arch in Indian Sumit Tulshidas Patil, Meena M. Meshram, Namdeo Y. Kamdi, Arun P. Kasote, Madhukar P. Parchand Department of Anatomy, Government Medical College, Nagpur, Maharashtra, India Abstract: Knowledge of the branching pattern of aortic arch is important during supra-aortic angiography, aortic instrumentation, thoracic and neck surgery. The purpose of this study is to describe different branching pattern of arch of aorta in Indian subjects, in order to offer useful data to anatomists, radiologists, vascular surgeons while relating it to the embryological basis. Seventy five arches of adult Indian cadavers were exposed and their branches examined during cadaveric dissection in the Department of Anatomy, Government Medical College, Nagpur. The usual three-branched aortic arch was found in 58 cadavers (77.3%); the 11 (14.66%) remaining aortic arch showed only two branches, out of which one was a common trunk, which incorporated the brachiocephalic trunk and left common carotid and other left subclavian artery and 6 (8%) aortic arches showed direct arch origin of the left vertebral artery. Although the variations are usually asymptomatic, they may cause dyspnoea, dysphasia, intermittent claudication, misinterpretation of radiological examinations and complications during neck and thorax surgery. Knowledge of different patterns of arch of aorta is critical when invading the arch of aorta and its branches by instruments, as all these areas are delicate. Key words: Thoracic aorta, Variations, Branches, Vascular surgery Received March 28, 2012; Revised July 5, 2012; Accepted August 23, 2012 Introduction between them. -

Blood Vessels and Circulation
19 Blood Vessels and Circulation Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Functional Anatomy of Blood Vessels Learning Outcomes 19.1 Distinguish between the pulmonary and systemic circuits, and identify afferent and efferent blood vessels. 19.2 Distinguish among the types of blood vessels on the basis of their structure and function. 19.3 Describe the structures of capillaries and their functions in the exchange of dissolved materials between blood and interstitial fluid. 19.4 Describe the venous system, and indicate the distribution of blood within the cardiovascular system. © 2018 Pearson Education, Inc. Module 19.1: The heart pumps blood, in sequence, through the arteries, capillaries, and veins of the pulmonary and systemic circuits Blood vessels . Blood vessels conduct blood between the heart and peripheral tissues . Arteries (carry blood away from the heart) • Also called efferent vessels . Veins (carry blood to the heart) • Also called afferent vessels . Capillaries (exchange substances between blood and tissues) • Interconnect smallest arteries and smallest veins © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Two circuits 1. Pulmonary circuit • To and from gas exchange surfaces in the lungs 2. Systemic circuit • To and from rest of body © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Circulation pathway through circuits 1. Right atrium (entry chamber) • Collects blood from systemic circuit • To right ventricle to pulmonary circuit 2. Pulmonary circuit • Pulmonary arteries to pulmonary capillaries to pulmonary veins © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Circulation pathway through circuits (continued) 3. Left atrium • Receives blood from pulmonary circuit • To left ventricle to systemic circuit 4. -

An Unusual Origin and Course of the Thyroidea Ima Artery, with Absence of Inferior Thyroid Artery Bilaterally
Surgical and Radiologic Anatomy (2019) 41:235–237 https://doi.org/10.1007/s00276-018-2122-1 ANATOMIC VARIATIONS An unusual origin and course of the thyroidea ima artery, with absence of inferior thyroid artery bilaterally Doris George Yohannan1 · Rajeev Rajan1 · Akhil Bhuvanendran Chandran1 · Renuka Krishnapillai1 Received: 31 May 2018 / Accepted: 21 October 2018 / Published online: 25 October 2018 © Springer-Verlag France SAS, part of Springer Nature 2018 Abstract We report an unusual origin and course of the thyroidea ima artery in a male cadaver. The ima artery originated from the right subclavian artery very close to origin of the right vertebral artery. The artery coursed anteriorly between the common carotid artery medially and internal jugular vein laterally. It then coursed obliquely, from below upwards, from lateral to medial superficial to common carotid artery, to reach the inferior pole of the right lobe of thyroid and branched repeatedly to supply the anteroinferior and posteroinferior aspects of both the thyroid lobes and isthmus. The superior thyroid arteries were normal. Both the inferior thyroid arteries were absent. The unusual feature of this thyroidea ima artery is its origin from the subclavian artery close to vertebral artery origin, the location being remarkably far-off from the usual near midline position, and the oblique and relatively superficial course. This report is a caveat to neck surgeons to consider such a superficially running vessel to be a thyroidea ima artery. Keywords Thyroid vascular anatomy · Thyroidea ima artery · Artery of Neubauer · Blood supply of thyroid · Variations Introduction (1.1%), transverse scapular (1.1%), or pericardiophrenic or thyrocervical trunk [8, 10].