Thyroidea Ima Artery: a Report of Two Cases 1Sagaya Raj, 2Azeem Mohiyuddin, 3Shuaib Merchant, 4Rijo M Jayaraju, 5Beauty Sasidharan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomy of the Thyroid, Parathyroid, Pituitary and Adrenal Glands, Surgery (2017), BASIC SCIENCE
BASIC SCIENCE The neuroendocrine parafollicular (C) cells from neural crest Anatomy of the thyroid, tissue develop separately in the ultimobranchial body, which develops from the 4th pharyngeal pouch. These cells migrate into parathyroid, pituitary and the thyroid tissue following fusion of the ultimobranchial body with the thyroid gland. adrenal glands Glandular development is controlled by thyroid-stimulating hormone (TSH) and the thyroid becomes functional during the Sarah Hillary third month of gestation. Saba P Balasubramanian Gross anatomy The thyroid gland lies anterior to the cricoid cartilage and tra- Abstract chea, and slightly inferior to the thyroid cartilages. It comprises A detailed understanding of anatomy is essential for several reasons: two lateral lobes joined together by an isthmus. The lateral lobes to enable accurate diagnosis and plan appropriate management; to can be traced from the lateral aspect of the thyroid cartilage perform surgery in a safe and effective manner avoiding damage to down to the level of the sixth tracheal ring. The isthmus overlies adjacent structures; and to anticipate and recognize variations in the second and third tracheal rings. The entire gland is enclosed normal anatomy. This article will cover the anatomy of four major within the pretracheal fascia, a layer of deep fascia that anchors endocrine glands (thyroid, parathyroid, pituitary and adrenal). Other the gland posteriorly with the trachea and the laryngopharynx, endocrine glands (such as the hypothalamus, pineal gland, thymus, causing it to move during swallowing. The gland has a fibrous endocrine pancreas and the gonads) are beyond the scope of this outer capsule, from which septae run into the gland to separate it article. -

Endocrine Block اللهم ال سهل اال ما جعلته سهل و أنت جتعل احلزن اذا شئت سهل
OSPE ENDOCRINE BLOCK اللهم ﻻ سهل اﻻ ما جعلته سهل و أنت جتعل احلزن اذا شئت سهل Important Points 1. Don’t forget to mention right and left. 2. Read the questions carefully. 3. Make sure your write the FULL name of the structures with the correct spelling. Example: IVC ✕ Inferior Vena Cava ✓ Aorta ✕ Abdominal aorta ✓ 4. There is NO guarantee whether or not the exam will go out of this file. ممكن يأشرون على أجزاء مو معلمه فراح نحط بيانات إضافية حاولوا تمرون عليها كلها Good luck! Pituitary gland Identify: 1. Anterior and posterior clinoidal process of sella turcica. 2. Hypophyseal fossa (sella turcica) Theory • The pituitary gland is located in middle cranial fossa and protected in sella turcica (hypophyseal fossa) of body of sphenoid. Relations Of Pituitary Gland hypothalamus Identify: 1. Mamillary body (posteriorly) 2. Optic chiasma (anteriorly) 3. Sphenoidal air sinuses (inferior) 4. Body of sphenoid 5. Pituitary gland Theory • If pituitary gland became enlarged (e.g adenoma) it will cause pressure on optic chiasma and lead to bilateral temporal eye field blindness (bilateral hemianopia) Relations Of Pituitary Gland Important! Identify: 1. Pituitary gland. 2. Diaphragma sellae (superior) 3. Sphenoidal air sinuses (inferior) 4. Cavernous sinuses (lateral) 5. Abducent nerve 6. Oculomotor nerve 7. Trochlear nerve 8. Ophthalmic nerve 9. Trigeminal (Maxillary) nerve Structures of lateral wall 10. Internal carotid artery Note: Ophthalmic and maxillary are both branches of the trigeminal nerve Divisions of Pituitary Gland Identify: 1. Anterior lobe (Adenohypophysis) 2. Optic chiasma 3. Infundibulum 4. Posterior lobe (Neurohypophysis) Theory Anterior Lobe Posterior Lobe • Adenohypophysis • Neurohypophysis • Secretes hormones • Stores hormones • Vascular connection to • Neural connection to hypothalamus by hypothalamus by Subdivisions hypophyseal portal hypothalamo-hypophyseal system (from superior tract from supraoptic and hypophyseal artery) paraventricular nuclei. -

Cervical Viscera and Root of Neck
Cervical viscera & Root of neck 頸部臟器 與 頸根部 解剖學科 馮琮涵 副教授 分機 3250 E-mail: [email protected] Outline: • Position and structure of cervical viscera • Blood supply and nerve innervation of cervical viscera • Contents in root of neck Viscera of the Neck Endocrine layer – thyroid and parathyroid glands Respiratory layer – larynx and trachea Alimentary layer – pharynx and esophagus Thyroid gland Position: deep to sterno-thyroid and sterno-hyoid ms. (the level of C5 to T1) coverd by pretracheal deep cervical fascia (loose sheath) and capsule (dense connective tissue) anterolateral to the trachea arteries: superior thyroid artery – ant. & post. branches inferior thyroid artery (br. of thyrocervical trunk) thyroid ima artery (10%) Veins: superior thyroid vein IJVs (internal jugular veins) middle thyroid vein IJVs inferior thyroid vein brachiocephalic vein Thyroid gland Lymphatic drainage: prelaryngeal, pretracheal and paratracheal • lymph nodes inferior deep cervical lymph nodes Nerves: superior, middle & inferior cervical sympathetic ganglia periarterial plexuses • # thyroglossal duct cysts, pyramidal lobe (50%) # Parathyroid glands Position: external to thyroid capsule, but inside its sheath superior parathyroid glands – 1 cm sup. to the point of inf. thyroid artery into thyroid inferior parathyroid glands – 1 cm inf. to inf. thyroid artery entry point (various position) Vessels: branches of inf. thyroid artery or sup. thyroid artery parathyroid veins venous plexuses of ant. surface of thyroid Nerves: thyroid branches of the cervical sympathetic ganglia Trachea Tracheal rings (C-shape cartilage) + trachealis (smooth m.) Position: C6 (inf. end of the larynx) – T4/T5 (sternal angle) # trache`ostomy – 1st and 2nd or 2nd through 4th tracheal rings # care: inf. thyroid veins, thyroid ima artery, brachiocephalic vein, thymus and trachea Esophagus Position: from the inf. -

Penetrating Carotid Artery: Uncommon Complex and Lethal Injuries
Eur J Trauma Emerg Surg (2011) 37:429–437 DOI 10.1007/s00068-011-0132-3 REVIEW ARTICLE Penetrating carotid artery: uncommon complex and lethal injuries J. A. Asensio • T. Vu • F. N. Mazzini • F. Herrerias • G. D. Pust • J. Sciarretta • J. Chandler • J. M. Verde • P. Menendez • J. M. Sanchez • P. Petrone • C. Marini Received: 16 June 2011 / Accepted: 19 June 2011 / Published online: 15 July 2011 Ó Springer-Verlag 2011 Abstract Carotid arterial injuries are the most difficult or occasionally via surgical cricothyroidotomy. Establish- and certainly the most immediately life-threatening injuries ing a surgical airway can be a difficult procedure given the found in penetrating neck trauma. Their propensity to bleed distortion of anatomic landmarks caused by hemorrhage. It actively and potentially occludes the airway and makes is also fraught with danger, as the incision may release the surgical intervention very challenging. Their potential for contained hematoma, resulting in torrential bleeding that causing fatal neurological outcomes demands that trauma can obscure the operative site and place the patient at risk surgeons exercise excellent judgment in the approach to for aspiration. These injuries incur high morbidity and their definitive management. The purpose of this article is mortality. Their neurologic sequelae can be devastating. to review the diagnosis and management of these injuries. Fortunately they are not common. Keywords Vascular Á Trauma Historical perspective Introduction The first documented case of the treatment of a cervical vascular injury is attributed to the French surgeon Ambrose Carotid arterial injuries are the most difficult and certainly Pare (1510–1590) [1], who was able to ligate the lacerated the most immediate life-threatening injuries found in carotid artery and a jugular vein of a wounded soldier. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -

Selective Venous Sampling for Primary Hyperparathyroidism: How to Perform an Examination and Interpret the Results with Reference to Thyroid Vein Anatomy
Jpn J Radiol DOI 10.1007/s11604-017-0658-3 INVITED REVIEW Selective venous sampling for primary hyperparathyroidism: how to perform an examination and interpret the results with reference to thyroid vein anatomy Takayuki Yamada1 · Masaya Ikuno1 · Yasumoto Shinjo1 · Atsushi Hiroishi1 · Shoichiro Matsushita1 · Tsuyoshi Morimoto1 · Reiko Kumano1 · Kunihiro Yagihashi1 · Takuyuki Katabami2 Received: 11 April 2017 / Accepted: 28 May 2017 © Japan Radiological Society 2017 Abstract Primary hyperparathyroidism (pHPT) causes and brachiocephalic veins for catheterization of the thyroid hypercalcemia. The treatment for pHPT is surgical dis- veins and venous anastomoses. section of the hyperfunctioning parathyroid gland. Lower rates of hypocalcemia and recurrent laryngeal nerve injury Keywords Primary hyperparathyroidism · Localization · imply that minimally invasive parathyroidectomy (MIP) is Thyroid vein · Venous sampling safer than bilateral neck resection. Current trends in MIP use can be inferred only by reference to preoperative locali- zation studies. Noninvasive imaging studies (typically pre- Introduction operative localization studies) show good detection rates of hyperfunctioning glands; however, there have also been Primary hyperparathyroidism (pHPT) is a common endocrine cases of nonlocalization or discordant results. Selective disease. Most patients have one adenoma, but double adeno- venous sampling (SVS) is an invasive localization method mas have been reported in up to 15% of cases [1]. Approxi- for detecting elevated intact parathyroid -
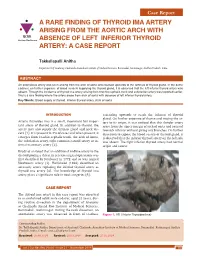
A RARE FINDING of THYROID IMA ARTERY ARISING from the AORTIC ARCH with IJCRR Section: Healthcare ABSENCE of LEFT INFERIOR THYROID ARTERY: a CASE REPORT
Case Report A RARE FINDING OF THYROID IMA ARTERY ARISING FROM THE AORTIC ARCH WITH IJCRR Section: Healthcare ABSENCE OF LEFT INFERIOR THYROID ARTERY: A CASE REPORT Takkallapalli Anitha Department of Anatomy, Chalmeda Anandrao Institute of Medical Sciences, Bommakal, Karimnagar, Andhra Pradesh, India. ABSTRACT An anomalous artery was seen arising from the arch of aorta and coursed upwards to the isthmus of thyroid gland. In the same cadaver, on further exposure of blood vessels supplying the thyroid gland, it is observed that the left inferior thyroid artery was absent. Though the incidence of thyroid ima artery arising from brachio cephalic trunk and subclavian artery was reported earlier, this is a rare finding where the artery arose from arch of aorta with absence of left inferior thyroid artery. Key Words: Blood supply of thyroid, Inferior thyroid artery, Arch of aorta INTRODUCTION ascending upwards to reach the isthmus of thyroid gland. On further exposure of thorax and tracing the ar- Arteria thyroidea ima is a small, inconstant but impor- tery to its origin, it was noticed that this slender artery tant artery of thyroid gland. In addition to thyroid, the arose from the upper margin of arch of aorta and coursed artery may also supply the thymus gland and neck vis- towards isthmus without giving any branches. On further cera [1]. It is present in 3% of cases and when present, it dissection to expose the blood vessels of thyroid gland, it emerges from brachio cephalic trunk, the arch of Aorta, is observed that the inferior thyroid artery on the left side the subclavian artery, right common carotid artery or in- was absent. -

Spontaneous Arteriovenous Malformations in the Cervical Area
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.3.303 on 1 June 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 303-309 Spontaneous arteriovenous malformations in the cervical area J. GREENBERG, M.D. From the Department of Neurology, Episcopal Hospital, Philadelphia, Pennsylvania 19125, U.S.A. SUMMARY Four patients with spontaneous arteriovenous malformations of cervical vessels have been presented. The embryology of these vessels has been discussed in order to suggest an ex- planation for the apparent difference in the incidence of arteriovenous malformations involving the internal carotid artery and those involving either the vertebral or the external carotid arteries. A fifth case (S.T.) is presented as a probable iatrogenic arteriovenous fistula and is to be added to the steadily growing reports of this phenomenon. Trauma is the most common cause of arteriovenous had sustained a minor injury to the posterior aspect communications between the blood vessels in of the right ear. Routine skull films at the time did not the cervical area (Aronson, 1961). Iatrogenic reveal a fracture, and there was no evidence of local Protected by copyright. deep tissue injury noted. fistulae occurring after carotid or vertebral angio- On the present admission, a slight prominence of the graphy are being reported with regularity in the right retroauricular region was noted and a thrill and recent literature (Sutton, 1962). Spontaneous mal- bruit were present. The bruit could be obliterated by formations in this area also occur. Thus far, eight local pressure. cases have been reported involving the vertebral The neurological examination was within normal vessels (Norman, Schmidt, and Grow, 1950; limits. -
Study on Branching Pattern of Aortic Arch in Indian
Original Article http://dx.doi.org/10.5115/acb.2012.45.3.203 pISSN 2093-3665 eISSN 2093-3673 Study on branching pattern of aortic arch in Indian Sumit Tulshidas Patil, Meena M. Meshram, Namdeo Y. Kamdi, Arun P. Kasote, Madhukar P. Parchand Department of Anatomy, Government Medical College, Nagpur, Maharashtra, India Abstract: Knowledge of the branching pattern of aortic arch is important during supra-aortic angiography, aortic instrumentation, thoracic and neck surgery. The purpose of this study is to describe different branching pattern of arch of aorta in Indian subjects, in order to offer useful data to anatomists, radiologists, vascular surgeons while relating it to the embryological basis. Seventy five arches of adult Indian cadavers were exposed and their branches examined during cadaveric dissection in the Department of Anatomy, Government Medical College, Nagpur. The usual three-branched aortic arch was found in 58 cadavers (77.3%); the 11 (14.66%) remaining aortic arch showed only two branches, out of which one was a common trunk, which incorporated the brachiocephalic trunk and left common carotid and other left subclavian artery and 6 (8%) aortic arches showed direct arch origin of the left vertebral artery. Although the variations are usually asymptomatic, they may cause dyspnoea, dysphasia, intermittent claudication, misinterpretation of radiological examinations and complications during neck and thorax surgery. Knowledge of different patterns of arch of aorta is critical when invading the arch of aorta and its branches by instruments, as all these areas are delicate. Key words: Thoracic aorta, Variations, Branches, Vascular surgery Received March 28, 2012; Revised July 5, 2012; Accepted August 23, 2012 Introduction between them. -

Axis Scientific Human Circulatory System 1/2 Life Size A-105864
Axis Scientific Human Circulatory System 1/2 Life Size A-105864 05. Superior Vena Cava 13. Ascending Aorta 21. Hepatic Vein 28. Celiac Trunk II. Lung 09. Pulmonary Trunk 19. Common III. Spleen Hepatic Artery 10. Pulmonary 15. Pulmonary Artery 17. Splenic Artery (Semilunar) Valve 20. Portal Vein 03. Left Atrium 18. Splenic Vein 01. Right Atrium 16. Pulmonary Vein 26. Superior 24. Superior 02. Right Ventricle Mesenteric Vein Mesenteric Artery 11. Supraventricular Crest 07. Interatrial Septum 22. Renal Artery 27. Inferior 14. Aortic (Semilunar) Valve Mesenteric Vein 08. Tricuspid (Right 23. Renal Vein 12. Mitral (Left Atrioventricular) Valve VI. Large Intestine Atrioventricular) Valve 29. Testicular / 30. Common Iliac Artery Ovarian Artery 32. Internal Iliac Artery 25. Inferior 31. External Iliac Artery Mesenteric Artery 33. Median Sacral Artery 41. Posterior Auricular Artery 57. Deep Palmar Arch 40. Occipital Artery 43. Superficial Temporal Artery 58. Dorsal Venous Arch 36. External Carotid Artery 42. Maxillary Artery 56. Superficial Palmar Arch 35. Internal Carotid Artery 44. Internal Jugular Vein 39. Facial Artery 45. External Jugular Vein 38. Lingual Artery and Vein 63. Deep Femoral Artery 34. Common Carotid Artery 37. Superior Thyroid Artery 62. Femoral Artery 48. Thyrocervical Trunk 49. Inferior Thyroid Artery 47. Subclavian Artery 69. Great Saphenous Vein 46. Subclavian Vein I. Heart 51. Thoracoacromial II. Lung Artery 64. Popliteal Artery 50. Axillary Artery 03. Left Atrium 01. Right Atrium 04. Left Ventricle 02. Right Ventricle 65. Posterior Tibial Artery 52. Brachial Artery 66. Anterior Tibial Artery 53. Deep Brachial VII. Descending Artery Aorta 70. Small Saphenous Vein IV. Liver 59. -

Bilateral Variations in the Divisions of Common Carotid Artery – a Case Report
eISSN 1308-4038 International Journal of Anatomical Variations (2012) 5: 116–119 Case Report Bilateral variations in the divisions of common carotid artery – a case report Published online December 20th, 2012 © http://www.ijav.org Bheemshetty S. PATIL Abstract Shankarappa D. DESAI During routine dissection, we found bilateral variation in the division of common carotid artery in a 48-year-old male cadaver. The right carotid, originated from the brachiocephalic trunk Ishwar B. BAGOJI behind the right sternoclavicular joint. The left carotid, originated directly from the aortic arch. Gavishiddappa A. HADIMANI Division of common carotid artery occured at higher level; i.e., above the level of superior lamina of thyroid cartilage. On the right side 4.2 cm and on left side 3.5 cm above the superior lamina of thyroid cartilage and just behind the angle of mandible. The arteries did not have any branches; Department of Anatomy, Shri B. M. Patil Medical College, except on the right side the superior thyroidal artery arose from the 2.5 cm below the bifurcation. Blde University, Bijapur, Karnataka, INDIA. Knowledge of origin and bifurcation of common carotid artery is very important to the ENT surgeons, general surgeons, endocrinologist and vascular surgeons. Bheemshetty S. Patil © Int J Anat Var (IJAV). 2012; 5: 116–119. Lecturer Department of Anatomy Shri B. M. Patil Medical College Blde University Bijapur-586103 Karnataka, INDIA. +91 8352-262770/ext. 2211 [email protected] Received October 10th, 2011; accepted August 26th, 2012 Key words [common carotid artery] [thyroid cartilage] [angle of mandible] [bifurcation of common carotid artery] Introduction gives off no branches in the neck, whereas the external does The right common carotid artery arises from the [2].