Spontaneous Arteriovenous Malformations in the Cervical Area
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ipsilateral Subclavian Steal in Association with Aberrant Origin of the Left Vertebral Artery from the Aortic Arch
411 Ipsilateral Subclavian Steal in Association with Aberrant Origin of the Left Vertebral Artery from the Aortic Arch John Holder1 Five cases are reported of left subclavian steal syndrome associated with anomalous Eugene F. Binet2 origin of the left vertebral artery from the aortic arch. In all five instances blood flow at Bernard Thompson3 the origin of the left vertebral artery was in an antegrade direction contrary to that usually reported in this condition. The distal subclavian artery was supplied via an extensive collateral network of vessels connecting the vertebral artery to the thyro cervical trunk. If a significant stenosis or occlusion is present within the left subc lavi an artery proximal to the origin of the left vertebral artery, the direction of the bl ood fl ow within the vertebral artery will reverse toward the parent vessel (retrograde flow). This phenomenon occurs when a negative pressure gradient of 20-40 torr exists between the vertebral-basilar artery junction and th e vertebral-subc lavian artery junction [1-3]. We describe five cases of subclavian steal confirmed by angiography where a significant stenosis or occlusion of the left subclavian artery was demonstrated in association with anomalous origin of th e left vertebral artery directly from the aortic arch. In all five cases blood flow at the origin of the left vertebral artery was in an antegrade direction contrary to that more commonly reported in the subclavian steal syndrome. Materials and Methods The five patients were all 44- 58-year-old men. Three sought medical attention for symptoms specificall y related to th e left arm . -

Penetrating Carotid Artery: Uncommon Complex and Lethal Injuries
Eur J Trauma Emerg Surg (2011) 37:429–437 DOI 10.1007/s00068-011-0132-3 REVIEW ARTICLE Penetrating carotid artery: uncommon complex and lethal injuries J. A. Asensio • T. Vu • F. N. Mazzini • F. Herrerias • G. D. Pust • J. Sciarretta • J. Chandler • J. M. Verde • P. Menendez • J. M. Sanchez • P. Petrone • C. Marini Received: 16 June 2011 / Accepted: 19 June 2011 / Published online: 15 July 2011 Ó Springer-Verlag 2011 Abstract Carotid arterial injuries are the most difficult or occasionally via surgical cricothyroidotomy. Establish- and certainly the most immediately life-threatening injuries ing a surgical airway can be a difficult procedure given the found in penetrating neck trauma. Their propensity to bleed distortion of anatomic landmarks caused by hemorrhage. It actively and potentially occludes the airway and makes is also fraught with danger, as the incision may release the surgical intervention very challenging. Their potential for contained hematoma, resulting in torrential bleeding that causing fatal neurological outcomes demands that trauma can obscure the operative site and place the patient at risk surgeons exercise excellent judgment in the approach to for aspiration. These injuries incur high morbidity and their definitive management. The purpose of this article is mortality. Their neurologic sequelae can be devastating. to review the diagnosis and management of these injuries. Fortunately they are not common. Keywords Vascular Á Trauma Historical perspective Introduction The first documented case of the treatment of a cervical vascular injury is attributed to the French surgeon Ambrose Carotid arterial injuries are the most difficult and certainly Pare (1510–1590) [1], who was able to ligate the lacerated the most immediate life-threatening injuries found in carotid artery and a jugular vein of a wounded soldier. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -
A RARE FINDING of THYROID IMA ARTERY ARISING from the AORTIC ARCH with IJCRR Section: Healthcare ABSENCE of LEFT INFERIOR THYROID ARTERY: a CASE REPORT
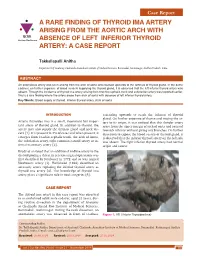
Case Report A RARE FINDING OF THYROID IMA ARTERY ARISING FROM THE AORTIC ARCH WITH IJCRR Section: Healthcare ABSENCE OF LEFT INFERIOR THYROID ARTERY: A CASE REPORT Takkallapalli Anitha Department of Anatomy, Chalmeda Anandrao Institute of Medical Sciences, Bommakal, Karimnagar, Andhra Pradesh, India. ABSTRACT An anomalous artery was seen arising from the arch of aorta and coursed upwards to the isthmus of thyroid gland. In the same cadaver, on further exposure of blood vessels supplying the thyroid gland, it is observed that the left inferior thyroid artery was absent. Though the incidence of thyroid ima artery arising from brachio cephalic trunk and subclavian artery was reported earlier, this is a rare finding where the artery arose from arch of aorta with absence of left inferior thyroid artery. Key Words: Blood supply of thyroid, Inferior thyroid artery, Arch of aorta INTRODUCTION ascending upwards to reach the isthmus of thyroid gland. On further exposure of thorax and tracing the ar- Arteria thyroidea ima is a small, inconstant but impor- tery to its origin, it was noticed that this slender artery tant artery of thyroid gland. In addition to thyroid, the arose from the upper margin of arch of aorta and coursed artery may also supply the thymus gland and neck vis- towards isthmus without giving any branches. On further cera [1]. It is present in 3% of cases and when present, it dissection to expose the blood vessels of thyroid gland, it emerges from brachio cephalic trunk, the arch of Aorta, is observed that the inferior thyroid artery on the left side the subclavian artery, right common carotid artery or in- was absent. -
Study on Branching Pattern of Aortic Arch in Indian
Original Article http://dx.doi.org/10.5115/acb.2012.45.3.203 pISSN 2093-3665 eISSN 2093-3673 Study on branching pattern of aortic arch in Indian Sumit Tulshidas Patil, Meena M. Meshram, Namdeo Y. Kamdi, Arun P. Kasote, Madhukar P. Parchand Department of Anatomy, Government Medical College, Nagpur, Maharashtra, India Abstract: Knowledge of the branching pattern of aortic arch is important during supra-aortic angiography, aortic instrumentation, thoracic and neck surgery. The purpose of this study is to describe different branching pattern of arch of aorta in Indian subjects, in order to offer useful data to anatomists, radiologists, vascular surgeons while relating it to the embryological basis. Seventy five arches of adult Indian cadavers were exposed and their branches examined during cadaveric dissection in the Department of Anatomy, Government Medical College, Nagpur. The usual three-branched aortic arch was found in 58 cadavers (77.3%); the 11 (14.66%) remaining aortic arch showed only two branches, out of which one was a common trunk, which incorporated the brachiocephalic trunk and left common carotid and other left subclavian artery and 6 (8%) aortic arches showed direct arch origin of the left vertebral artery. Although the variations are usually asymptomatic, they may cause dyspnoea, dysphasia, intermittent claudication, misinterpretation of radiological examinations and complications during neck and thorax surgery. Knowledge of different patterns of arch of aorta is critical when invading the arch of aorta and its branches by instruments, as all these areas are delicate. Key words: Thoracic aorta, Variations, Branches, Vascular surgery Received March 28, 2012; Revised July 5, 2012; Accepted August 23, 2012 Introduction between them. -

Ascending and Descending Thoracic Vertebral Arteries
CLINICAL REPORT EXTRACRANIAL VASCULAR Ascending and Descending Thoracic Vertebral Arteries X P. Gailloud, X L. Gregg, X M.S. Pearl, and X D. San Millan ABSTRACT SUMMARY: Thoracic vertebral arteries are anastomotic chains similar to cervical vertebral arteries but found at the thoracic level. Descending thoracic vertebral arteries originate from the pretransverse segment of the cervical vertebral artery and curve caudally to pass into the last transverse foramen or the first costotransverse space. Ascending thoracic vertebral arteries originate from the aorta, pass through at least 1 costotransverse space, and continue cranially as the cervical vertebral artery. This report describes the angiographic anatomy and clinical significance of 9 cases of descending and 2 cases of ascending thoracic vertebral arteries. Being located within the upper costotransverse spaces, ascending and descending thoracic vertebral arteries can have important implications during spine inter- ventional or surgical procedures. Because they frequently provide radiculomedullary or bronchial branches, they can also be involved in spinal cord ischemia, supply vascular malformations, or be an elusive source of hemoptysis. ABBREVIATIONS: ISA ϭ intersegmental artery; SIA ϭ supreme intercostal artery; VA ϭ vertebral artery he cervical portion of the vertebral artery (VA) is formed by a bral arteria lusoria8-13 or persistent left seventh cervical ISA of Tseries of anastomoses established between the first 6 cervical aortic origin.14 intersegmental arteries (ISAs) and one of the carotid-vertebral This report discusses 9 angiographic observations of descend- anastomoses, the proatlantal artery.1-3 The VA is labeled a “post- ing thoracic VAs and 2 cases of ascending thoracic VAs. costal” anastomotic chain (ie, located behind the costal process of cervical vertebrae or dorsal to the rib itself at the thoracic level) to CASE SERIES emphasize its location within the transverse foramina. -

The Rare Origin of the Suprascapular Artery Arising Off The
eISSN 1308-4038 International Journal of Anatomical Variations (2011) 4: 182–184 Case Report The rare origin of the suprascapular artery arising off the internal thoracic artery in the presence of the thyrocervical trunk: clinical and surgical implications Published online December 2nd, 2011 © http://www.ijav.org Stavros ATSAS ABSTRACT Jacob N. FOX During routine dissection of the subclavian artery and its branches, the suprascapular artery was found arising from H. Wayne LAMBERT the proximal end of the internal thoracic artery in only the left side of a 68-year-old Caucasian male, despite the presence of the thyrocervical trunk on the ipsilateral side. The suprascapular artery ran deep to the proximal one- third of the clavicle then continued its usual course, running parallel to the suprascapular nerve and passing over the superior transverse scapular ligament distally. Knowledge of this variant origin of the suprascapular artery is clinically Department of Neurobiology and Anatomy, West Virginia University School of Medicine, important because the internal thoracic artery is utilized for a majority of the 800,000 coronary artery bypass surgeries Robert C. Byrd Health Sciences Center, Morgantown, West Virginia, USA. performed worldwide each year. Its course deep to the clavicle is also significant due to clavicular fractures accounting for approximately 5-15% of adult bone fractures. © IJAV. 2011; 4: 182–184. Dr. H. Wayne Lambert, PhD Associate Professor West Virginia University School of Medicine Robert C. Byrd Health Sciences Center Department of Neurobiology and Anatomy HSN 4052; P.O. Box 9128 Morgantown, WV, 26506-9128, USA. +1 304 293-0610 [email protected] Key words [anatomical variant] [suprascapular artery] [internal thoracic artery] [branches of subclavian artery] [thyrocervical trunk] [coronary bypass Received June 21st, 2011; accepted October 12th, 2011 surgery] [radical and modified neck dissections] Introduction In 2005, Weiglein et al. -

Blood Vessels and Circulation
19 Blood Vessels and Circulation Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Functional Anatomy of Blood Vessels Learning Outcomes 19.1 Distinguish between the pulmonary and systemic circuits, and identify afferent and efferent blood vessels. 19.2 Distinguish among the types of blood vessels on the basis of their structure and function. 19.3 Describe the structures of capillaries and their functions in the exchange of dissolved materials between blood and interstitial fluid. 19.4 Describe the venous system, and indicate the distribution of blood within the cardiovascular system. © 2018 Pearson Education, Inc. Module 19.1: The heart pumps blood, in sequence, through the arteries, capillaries, and veins of the pulmonary and systemic circuits Blood vessels . Blood vessels conduct blood between the heart and peripheral tissues . Arteries (carry blood away from the heart) • Also called efferent vessels . Veins (carry blood to the heart) • Also called afferent vessels . Capillaries (exchange substances between blood and tissues) • Interconnect smallest arteries and smallest veins © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Two circuits 1. Pulmonary circuit • To and from gas exchange surfaces in the lungs 2. Systemic circuit • To and from rest of body © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Circulation pathway through circuits 1. Right atrium (entry chamber) • Collects blood from systemic circuit • To right ventricle to pulmonary circuit 2. Pulmonary circuit • Pulmonary arteries to pulmonary capillaries to pulmonary veins © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Circulation pathway through circuits (continued) 3. Left atrium • Receives blood from pulmonary circuit • To left ventricle to systemic circuit 4. -

An Unusual Origin and Course of the Thyroidea Ima Artery, with Absence of Inferior Thyroid Artery Bilaterally
Surgical and Radiologic Anatomy (2019) 41:235–237 https://doi.org/10.1007/s00276-018-2122-1 ANATOMIC VARIATIONS An unusual origin and course of the thyroidea ima artery, with absence of inferior thyroid artery bilaterally Doris George Yohannan1 · Rajeev Rajan1 · Akhil Bhuvanendran Chandran1 · Renuka Krishnapillai1 Received: 31 May 2018 / Accepted: 21 October 2018 / Published online: 25 October 2018 © Springer-Verlag France SAS, part of Springer Nature 2018 Abstract We report an unusual origin and course of the thyroidea ima artery in a male cadaver. The ima artery originated from the right subclavian artery very close to origin of the right vertebral artery. The artery coursed anteriorly between the common carotid artery medially and internal jugular vein laterally. It then coursed obliquely, from below upwards, from lateral to medial superficial to common carotid artery, to reach the inferior pole of the right lobe of thyroid and branched repeatedly to supply the anteroinferior and posteroinferior aspects of both the thyroid lobes and isthmus. The superior thyroid arteries were normal. Both the inferior thyroid arteries were absent. The unusual feature of this thyroidea ima artery is its origin from the subclavian artery close to vertebral artery origin, the location being remarkably far-off from the usual near midline position, and the oblique and relatively superficial course. This report is a caveat to neck surgeons to consider such a superficially running vessel to be a thyroidea ima artery. Keywords Thyroid vascular anatomy · Thyroidea ima artery · Artery of Neubauer · Blood supply of thyroid · Variations Introduction (1.1%), transverse scapular (1.1%), or pericardiophrenic or thyrocervical trunk [8, 10]. -

SAY: Welcome to Module 1: Anatomy & Physiology of the Brain. This
12/19/2018 11:00 AM FOUNDATIONAL LEARNING SYSTEM 092892-181219 © Johnson & Johnson Servicesv Inc. 2018 All rights reserved. 1 SAY: Welcome to Module 1: Anatomy & Physiology of the Brain. This module will strengthen your understanding of basic neuroanatomy, neurovasculature, and functional roles of specific brain regions. 1 12/19/2018 11:00 AM Lesson 1: Introduction to the Brain The brain is a dense organ with various functional units. Understanding the anatomy of the brain can be aided by looking at it from different organizational layers. In this lesson, we’ll discuss the principle brain regions, layers of the brain, and lobes of the brain, as well as common terms used to orient neuroanatomical discussions. 2 SAY: The brain is a dense organ with various functional units. Understanding the anatomy of the brain can be aided by looking at it from different organizational layers. (Purves 2012/p717/para1) In this lesson, we’ll explore these organizational layers by discussing the principle brain regions, layers of the brain, and lobes of the brain. We’ll also discuss the terms used by scientists and healthcare providers to orient neuroanatomical discussions. 2 12/19/2018 11:00 AM Lesson 1: Learning Objectives • Define terms used to specify neuroanatomical locations • Recall the 4 principle regions of the brain • Identify the 3 layers of the brain and their relative location • Match each of the 4 lobes of the brain with their respective functions 3 SAY: Please take a moment to review the learning objectives for this lesson. 3 12/19/2018 11:00 AM Directional Terms Used in Anatomy 4 SAY: Specific directional terms are used when specifying the location of a structure or area of the brain. -

Left Common Carotid Artery Arising from Brachiocephalic Trunk and Their Aberrant Course Displacing Trachea
International Journal of Research in Medical Sciences Yadav P et al. Int J Res Med Sci. 2016 Sep;4(9):4220-4222 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20162965 Case Report Left common carotid artery arising from brachiocephalic trunk and their aberrant course displacing trachea Pratiksha Yadav*, Rajul Bhargava, S. G. Gandage Department of Radio-diagnosis, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, Maharashtra, India Received: 17 July 2016 Accepted: 12 August 2016 *Correspondence: Dr. Pratiksha Yadav, E-mail: yadavpratiksha@hotmail. Com Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Bovine arch commonly refer a group of congenital variations in the branches of arch of aorta, in which there is aberrant origin of left common carotid artery. These are usually detected incidentally, however rarely they can cause dysphagia lusoria. We report a case of bovine arch and aberrant left common carotid artery in a 62 years old female who had come with complaint of mild dyspnea. On radiograph there was superior mediastinal widening and shift of trachea to right side. CT scan was advised for further evaluation. On CECT there was only two main branches arised from arch of aorta, brachiocephalic trunk and right subclavian artery. There was aberrant origin of left common carotid artery seen from brachiocephalic trunk.