Penetrating Carotid Artery: Uncommon Complex and Lethal Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -
A RARE FINDING of THYROID IMA ARTERY ARISING from the AORTIC ARCH with IJCRR Section: Healthcare ABSENCE of LEFT INFERIOR THYROID ARTERY: a CASE REPORT
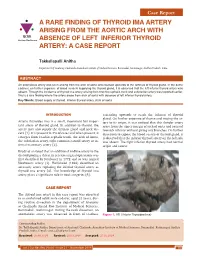
Case Report A RARE FINDING OF THYROID IMA ARTERY ARISING FROM THE AORTIC ARCH WITH IJCRR Section: Healthcare ABSENCE OF LEFT INFERIOR THYROID ARTERY: A CASE REPORT Takkallapalli Anitha Department of Anatomy, Chalmeda Anandrao Institute of Medical Sciences, Bommakal, Karimnagar, Andhra Pradesh, India. ABSTRACT An anomalous artery was seen arising from the arch of aorta and coursed upwards to the isthmus of thyroid gland. In the same cadaver, on further exposure of blood vessels supplying the thyroid gland, it is observed that the left inferior thyroid artery was absent. Though the incidence of thyroid ima artery arising from brachio cephalic trunk and subclavian artery was reported earlier, this is a rare finding where the artery arose from arch of aorta with absence of left inferior thyroid artery. Key Words: Blood supply of thyroid, Inferior thyroid artery, Arch of aorta INTRODUCTION ascending upwards to reach the isthmus of thyroid gland. On further exposure of thorax and tracing the ar- Arteria thyroidea ima is a small, inconstant but impor- tery to its origin, it was noticed that this slender artery tant artery of thyroid gland. In addition to thyroid, the arose from the upper margin of arch of aorta and coursed artery may also supply the thymus gland and neck vis- towards isthmus without giving any branches. On further cera [1]. It is present in 3% of cases and when present, it dissection to expose the blood vessels of thyroid gland, it emerges from brachio cephalic trunk, the arch of Aorta, is observed that the inferior thyroid artery on the left side the subclavian artery, right common carotid artery or in- was absent. -

Spontaneous Arteriovenous Malformations in the Cervical Area
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.3.303 on 1 June 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 303-309 Spontaneous arteriovenous malformations in the cervical area J. GREENBERG, M.D. From the Department of Neurology, Episcopal Hospital, Philadelphia, Pennsylvania 19125, U.S.A. SUMMARY Four patients with spontaneous arteriovenous malformations of cervical vessels have been presented. The embryology of these vessels has been discussed in order to suggest an ex- planation for the apparent difference in the incidence of arteriovenous malformations involving the internal carotid artery and those involving either the vertebral or the external carotid arteries. A fifth case (S.T.) is presented as a probable iatrogenic arteriovenous fistula and is to be added to the steadily growing reports of this phenomenon. Trauma is the most common cause of arteriovenous had sustained a minor injury to the posterior aspect communications between the blood vessels in of the right ear. Routine skull films at the time did not the cervical area (Aronson, 1961). Iatrogenic reveal a fracture, and there was no evidence of local Protected by copyright. deep tissue injury noted. fistulae occurring after carotid or vertebral angio- On the present admission, a slight prominence of the graphy are being reported with regularity in the right retroauricular region was noted and a thrill and recent literature (Sutton, 1962). Spontaneous mal- bruit were present. The bruit could be obliterated by formations in this area also occur. Thus far, eight local pressure. cases have been reported involving the vertebral The neurological examination was within normal vessels (Norman, Schmidt, and Grow, 1950; limits. -
Study on Branching Pattern of Aortic Arch in Indian
Original Article http://dx.doi.org/10.5115/acb.2012.45.3.203 pISSN 2093-3665 eISSN 2093-3673 Study on branching pattern of aortic arch in Indian Sumit Tulshidas Patil, Meena M. Meshram, Namdeo Y. Kamdi, Arun P. Kasote, Madhukar P. Parchand Department of Anatomy, Government Medical College, Nagpur, Maharashtra, India Abstract: Knowledge of the branching pattern of aortic arch is important during supra-aortic angiography, aortic instrumentation, thoracic and neck surgery. The purpose of this study is to describe different branching pattern of arch of aorta in Indian subjects, in order to offer useful data to anatomists, radiologists, vascular surgeons while relating it to the embryological basis. Seventy five arches of adult Indian cadavers were exposed and their branches examined during cadaveric dissection in the Department of Anatomy, Government Medical College, Nagpur. The usual three-branched aortic arch was found in 58 cadavers (77.3%); the 11 (14.66%) remaining aortic arch showed only two branches, out of which one was a common trunk, which incorporated the brachiocephalic trunk and left common carotid and other left subclavian artery and 6 (8%) aortic arches showed direct arch origin of the left vertebral artery. Although the variations are usually asymptomatic, they may cause dyspnoea, dysphasia, intermittent claudication, misinterpretation of radiological examinations and complications during neck and thorax surgery. Knowledge of different patterns of arch of aorta is critical when invading the arch of aorta and its branches by instruments, as all these areas are delicate. Key words: Thoracic aorta, Variations, Branches, Vascular surgery Received March 28, 2012; Revised July 5, 2012; Accepted August 23, 2012 Introduction between them. -

Blood Vessels and Circulation
19 Blood Vessels and Circulation Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Functional Anatomy of Blood Vessels Learning Outcomes 19.1 Distinguish between the pulmonary and systemic circuits, and identify afferent and efferent blood vessels. 19.2 Distinguish among the types of blood vessels on the basis of their structure and function. 19.3 Describe the structures of capillaries and their functions in the exchange of dissolved materials between blood and interstitial fluid. 19.4 Describe the venous system, and indicate the distribution of blood within the cardiovascular system. © 2018 Pearson Education, Inc. Module 19.1: The heart pumps blood, in sequence, through the arteries, capillaries, and veins of the pulmonary and systemic circuits Blood vessels . Blood vessels conduct blood between the heart and peripheral tissues . Arteries (carry blood away from the heart) • Also called efferent vessels . Veins (carry blood to the heart) • Also called afferent vessels . Capillaries (exchange substances between blood and tissues) • Interconnect smallest arteries and smallest veins © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Two circuits 1. Pulmonary circuit • To and from gas exchange surfaces in the lungs 2. Systemic circuit • To and from rest of body © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Circulation pathway through circuits 1. Right atrium (entry chamber) • Collects blood from systemic circuit • To right ventricle to pulmonary circuit 2. Pulmonary circuit • Pulmonary arteries to pulmonary capillaries to pulmonary veins © 2018 Pearson Education, Inc. Module 19.1: Blood vessels and circuits Circulation pathway through circuits (continued) 3. Left atrium • Receives blood from pulmonary circuit • To left ventricle to systemic circuit 4. -

An Unusual Origin and Course of the Thyroidea Ima Artery, with Absence of Inferior Thyroid Artery Bilaterally
Surgical and Radiologic Anatomy (2019) 41:235–237 https://doi.org/10.1007/s00276-018-2122-1 ANATOMIC VARIATIONS An unusual origin and course of the thyroidea ima artery, with absence of inferior thyroid artery bilaterally Doris George Yohannan1 · Rajeev Rajan1 · Akhil Bhuvanendran Chandran1 · Renuka Krishnapillai1 Received: 31 May 2018 / Accepted: 21 October 2018 / Published online: 25 October 2018 © Springer-Verlag France SAS, part of Springer Nature 2018 Abstract We report an unusual origin and course of the thyroidea ima artery in a male cadaver. The ima artery originated from the right subclavian artery very close to origin of the right vertebral artery. The artery coursed anteriorly between the common carotid artery medially and internal jugular vein laterally. It then coursed obliquely, from below upwards, from lateral to medial superficial to common carotid artery, to reach the inferior pole of the right lobe of thyroid and branched repeatedly to supply the anteroinferior and posteroinferior aspects of both the thyroid lobes and isthmus. The superior thyroid arteries were normal. Both the inferior thyroid arteries were absent. The unusual feature of this thyroidea ima artery is its origin from the subclavian artery close to vertebral artery origin, the location being remarkably far-off from the usual near midline position, and the oblique and relatively superficial course. This report is a caveat to neck surgeons to consider such a superficially running vessel to be a thyroidea ima artery. Keywords Thyroid vascular anatomy · Thyroidea ima artery · Artery of Neubauer · Blood supply of thyroid · Variations Introduction (1.1%), transverse scapular (1.1%), or pericardiophrenic or thyrocervical trunk [8, 10]. -

Left Common Carotid Artery Arising from Brachiocephalic Trunk and Their Aberrant Course Displacing Trachea
International Journal of Research in Medical Sciences Yadav P et al. Int J Res Med Sci. 2016 Sep;4(9):4220-4222 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20162965 Case Report Left common carotid artery arising from brachiocephalic trunk and their aberrant course displacing trachea Pratiksha Yadav*, Rajul Bhargava, S. G. Gandage Department of Radio-diagnosis, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, Maharashtra, India Received: 17 July 2016 Accepted: 12 August 2016 *Correspondence: Dr. Pratiksha Yadav, E-mail: yadavpratiksha@hotmail. Com Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Bovine arch commonly refer a group of congenital variations in the branches of arch of aorta, in which there is aberrant origin of left common carotid artery. These are usually detected incidentally, however rarely they can cause dysphagia lusoria. We report a case of bovine arch and aberrant left common carotid artery in a 62 years old female who had come with complaint of mild dyspnea. On radiograph there was superior mediastinal widening and shift of trachea to right side. CT scan was advised for further evaluation. On CECT there was only two main branches arised from arch of aorta, brachiocephalic trunk and right subclavian artery. There was aberrant origin of left common carotid artery seen from brachiocephalic trunk. -

Head and Neck CT Angiography to Assess the Internal Carotid Artery
Wang et al. BMC Neurology (2020) 20:334 https://doi.org/10.1186/s12883-020-01915-w RESEARCH ARTICLE Open Access Head and neck CT angiography to assess the internal carotid artery stealing pathway Dongxu Wang1 , Zheng Li1, Xiaoyang Zheng1, Houyi Cong1, Tianyu Zhang1, Zhenghua Wang2, Yuguang Wang1* and Jun He3 Abstract Background: Common carotid artery occlusive disease (CCAOD) could form internal carotid artery steal pathways. Based on the diagnostic results of digital subtraction angiography (DSA), head and neck computed tomography angiography (CTA) was used to find the internal carotid artery stealing pathway after CCAOD. Methods: The clinical and imaging data of 18 patients with CCAOD were retrospectively analyzed. DSA and CTA was used to evaluate internal carotid artery steal pathways. Results: Of the 18 patients with CCAOD, 10 patients found internal carotid artery steal pathways. There were 7 males and 3 females. Vascular ultrasound examination of all patients: The affected side had no blood flow in common carotid artery (CCA), and had retrograde blood flow in the external carotid artery (ECA). The blood flow of the affected side was decreased in the internal carotid artery (ICA), but it was antegrade. DSA diagnosed 10 cases of CCA occlusion and CTA diagnosed 10 cases of CCA occlusion. DSA and CTA found 6 internal carotid artery blood stealing pathways: ① Vertebral artery → occipital artery → external carotid artery → internal carotid artery (6 cases); ② Thyrocervical trunk → ascending cervical artery → occipital artery → external -

Thyroidea Ima Artery: a Report of Two Cases 1Sagaya Raj, 2Azeem Mohiyuddin, 3Shuaib Merchant, 4Rijo M Jayaraju, 5Beauty Sasidharan
IJHNS Thyroidea10.5005/jp-journals-10001-1188 Ima Artery: A report of Two Cases CASE REPORT Thyroidea Ima Artery: A Report of Two Cases 1Sagaya Raj, 2Azeem Mohiyuddin, 3Shuaib Merchant, 4Rijo M Jayaraju, 5Beauty Sasidharan ABSTRACT MATERIALS AND METHODS Thyroidea ima is a rare anomalous artery supplying the thyroid We routinely dissect and expose the common carotid artery gland apart from the superior and inferior thyroid arteries. It is of surgical importance in thyroid, parathyroid and tracheal before mobilizing the thyroid gland (lateral to medial surgeries. approach). By this approach, a good vascular control is Our study aims to highlight two cases of thyroidea ima artery achieved and inadvertent injury to blood vessels is avoided found during thyroidectomy: even if the thyroid gland is large and extending retrosternal. • Case 1: Thyroidea ima artery was seen arising from the medial surface of the right common carotid artery in a female patient, The three structures of significance between common carotid who underwent total thyroidectomy. and trachea are the recurrent laryngeal nerve, inferior thyroid • Case 2: Thyroidea ima artery was seen arising from the ante- artery and middle thyroid vein. Any anomalous vessel in this rior surface of the right innominate artery, in a female patient, who underwent right hemithyroidectomy. location can be easily identified and dissected to its origin thereby avoiding injury. Conclusion: Thyroidea ima artery, although a rare arterial varia- tion, a thorough regional anatomic knowledge and meticulous In our experience in the two cases mentioned, the thy- dissection will not only help us in identifying such a vascular roidea ima artery was found to be arising from right common variation, also help us in preventing an accidental injury. -

An Investigation of Virgin Variation of Branching Pattern of ECA and CCA: a Case Report
Case report http://dx.doi.org/10.4322/jms.096715 An investigation of virgin variation of branching pattern of ECA and CCA: a case report RAJANI, S.* Department of Anatomy, All India Institute of Medical Sciences, Rishikesh, Uttrakhand, India *E-mail: [email protected] Abstract Introduction: Common carotid and its two major branches, external and internal carotid arteries form arterial network for blood supply in the head and neck region. Variations in configuration and branching pattern of these arteries change the irrigation pattern and complicate the identification of specific arteries during surgical intervention coupled with imagery interpretation for diagnosis. Though handful variations have been documented yet there is strong need to report unusual, new and virgin organization of configuration and branching pattern in these arteries. Case Report: During dissection of head and neck region, anomalous branching pattern consisting of bilateral trifurcation/quadrification of common and external carotid arteries and abnormal trifurcation of distal external carotid artery was observed. Conclusion: Lack of knowledge of these variants in branching configuration may lead to unfortunate differential diagnosis and iatrogenic complications. Keywords: common carotid, external carotid artery, quadrification, trifurcation, branching pattern. 1 Introduction The common carotid artery (CCA) bifurcating into CCA bifurcated into ECA, ICA and also gave off superior external and internal carotid arteries at the level of superior thyroid artery bilaterally in this cadaver at 2 cm above thyroid border of thyroid cartilage in carotid triangle (STANDRING, cartilage in right (Figure 1R) and just below the level of angle 2008) plays major role for blood supply to the head and neck of mandible at 2.5 cm above the upper border of thyroid region. -

Blood Cell Models
BLOOD CELL MODELS Erythrocyte Platelet BLOOD CELL MODELS Neutrophil Eosinophil BLOOD CELL MODELS Basophil Monocyte BLOOD CELL MODELS Lymphocyte BLOOD CELL MODELS BLOOD CELL MODELS BLOOD CELL MODELS BLOOD CELL MODELS BLOOD SMEAR SLIDES Erythrocyt es Platelets Neutrophi l Eosinophil Lymphocyt e Monocyt e Basophil BLOOD SMEAR SLIDES HEART MODEL Brachiocephalic Artery Left Common Carotid Artery ANTERIOR VIEW LEFT VIEW Left Subclavian Superior Artery Vena Aortic Arch Cava Pulmonary Ligamentum Arteriosus Right Trunk Aortic Aorta Atrium Arch Pulmonary Arteries Pulmonary Coronary Veins Arteries Left Atrium Left Ventricle Right Ventricle Interventricular Sulcus (groove between ventricles) ANTERIOR VIEW Brachiocephalic Artery HEART MODEL ANTERIOR VIEW Left Common Carotid Artery Aortic Pulmonary Superior Left Subclavian Artery Arch Arteries Vena Cava Pulmonary Aortic Trunk Arch Right Pulmonary Semilunar Atrium Bicuspid Valve Aorta Valve Aortic Semilunar Valve Interventricular Septum (Separates ventricles) Tricuspid Valve Left Ventricle Chordae Pulmonary Tendineae Veins Right Left Ventricle Atrium Endocardium (inner layer) Left Myocardium (muscle layer) Papillary Muscles Ventricle Epicardium (outer layer) HEART MODEL Superior Superior Vena Vena Cava Cava RIGHT VIEW Pulmonary Trunk Aorta Right Aorta Atrium Right Right Ventricle Ventricle Fossa Ovalis Tricuspid Valve Right Inferior Atrium Vena Cava HEART MODEL Brachiocephalic Artery Brachiocephalic Left POSTERIOR VIEW Artery Subclavian Left Artery Common Left Carotid Common Artery Carotid Left Artery