Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Penetrating Carotid Artery: Uncommon Complex and Lethal Injuries
Eur J Trauma Emerg Surg (2011) 37:429–437 DOI 10.1007/s00068-011-0132-3 REVIEW ARTICLE Penetrating carotid artery: uncommon complex and lethal injuries J. A. Asensio • T. Vu • F. N. Mazzini • F. Herrerias • G. D. Pust • J. Sciarretta • J. Chandler • J. M. Verde • P. Menendez • J. M. Sanchez • P. Petrone • C. Marini Received: 16 June 2011 / Accepted: 19 June 2011 / Published online: 15 July 2011 Ó Springer-Verlag 2011 Abstract Carotid arterial injuries are the most difficult or occasionally via surgical cricothyroidotomy. Establish- and certainly the most immediately life-threatening injuries ing a surgical airway can be a difficult procedure given the found in penetrating neck trauma. Their propensity to bleed distortion of anatomic landmarks caused by hemorrhage. It actively and potentially occludes the airway and makes is also fraught with danger, as the incision may release the surgical intervention very challenging. Their potential for contained hematoma, resulting in torrential bleeding that causing fatal neurological outcomes demands that trauma can obscure the operative site and place the patient at risk surgeons exercise excellent judgment in the approach to for aspiration. These injuries incur high morbidity and their definitive management. The purpose of this article is mortality. Their neurologic sequelae can be devastating. to review the diagnosis and management of these injuries. Fortunately they are not common. Keywords Vascular Á Trauma Historical perspective Introduction The first documented case of the treatment of a cervical vascular injury is attributed to the French surgeon Ambrose Carotid arterial injuries are the most difficult and certainly Pare (1510–1590) [1], who was able to ligate the lacerated the most immediate life-threatening injuries found in carotid artery and a jugular vein of a wounded soldier. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Cervical Arterial Collateral Network References Reply: Reference Age
Cervical Arterial Collateral Network Age and Gender Effects on Normal Regional Cerebral Purkayastha et al1 reported 3 cases of proatlantal intersegmental Blood Flow arteries of external carotid artery origin associated with Galen’s vein We read with great interest the article of Takahashi et al.1 The article malformation; however, because of their configuration, I believe that points out the use of 3D stereotactic surface projections (3D-SSP) to the 3 cases do not demonstrate this rare arterial variation, but rather study the age-effect on regional cerebral blood flow (rCBF). The show collateral blood flow from the occipital artery (OA) to the ver- greatest rCBF reduction observed was in the bilateral anterior cingu- tebral artery (VA). In patients with a vein of Galen malformation, the late. Although we generally agree with the conclusions, we would like intra-arterial blood pressure in the VA is lower than that in the OA to emphasize some methodologic issues that may have had an impact because of blood steal phenomenon at the malformation. It is well on the obtained results. known that there is a cervical arterial collateral network between OA, In the study, 31 healthy volunteers between 50 and 79 years were classified in 3 different age classes (50–59, 60–69, and 70–79 years). VA, and the deep cervical artery arising from the subclavian artery.2 If Statistical analysis was performed 2 by 2 by using unpaired Student t test. one of these arteries is occluded, the remaining arteries and their Rather than considering age as a discrete variable, the analysis would have branches are dilated and supply the distal segment of the occluded been strengthened by performing a multivariate analysis based on the artery. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -

Embolization for Hemoptysis—Angiographic Anatomy of Bronchial and Systemic Arteries
THIEME 184 Pictorial Essay Embolization for Hemoptysis—Angiographic Anatomy of Bronchial and Systemic Arteries Vikash Srinivasaiah Setty Chennur1 Kumar Kempegowda Shashi1 Stephen Edward Ryan1 1 1 Adnan Hadziomerovic Ashish Gupta 1Division of Angio-Interventional Radiology, Department of Medical Address for correspondence Ashish Gupta, MD, Division of Imaging, University of Ottawa, The Ottawa Hospital, Ottawa, Angio-Interventional Radiology, Department of Medical Imaging, Ontario, Canada University of Ottawa, The Ottawa Hospital, 501 Smyth Road, Ottawa, ON K1H 8L6, Canada (e-mail: [email protected]). J Clin Interv Radiol ISVIR 2018;2:184–190 Abstract Massive hemoptysis is a potentially fatal respiratory emergency. The majority of these patients are referred to interventional radiology for bronchial artery embolization (BAE). Immediate clinical success in stopping hemoptysis ranges from 70 to 99%. However, recurrent hemoptysis after BAE is seen in 10 to 55% patients. One of the main reasons for recurrence is incomplete embolization due to unidentified aberrant Keywords bronchial and/or non-bronchial systemic arterial supply. This pictorial essay aims to ► bronchial describe the normal and variant bronchial arterial anatomy and non-bronchial systemic ► embolization arterial feeders to the lungs on conventional angiography; the knowledge of which is ► hemoptysis critical for interventional radiologists involved in the care of patients with hemoptysis. Introduction Angiographic Anatomy of Bronchial Arteries Massive hemoptysis is a respiratory -

Intercostal Arteries a Single Posterior & Two Anterior Intercostal Arteries
Intercostal Arteries •Each intercostal space contains: . A single posterior & .Two anterior intercostal arteries •Each artery gives off branches to the muscles, skin, parietal pleura Posterior Intercostal Arteries In the upper two spaces, arise from the superior intercostal artery (a branch of costocervical trunk of the subclavian artery) In the lower nine spaces, arise from the branches of thoracic aorta The course and branching of the intercostal arteries follow the intercostal Posterior intercostal artery Course of intercostal vessels in the posterior thoracic wall Anterior Intercostal Arteries In the upper six spaces, arise from the internal thoracic artery In the lower three spaces arise from the musculophrenic artery (one of the terminal branch of internal thoracic) Form anastomosis with the posterior intercostal arteries Intercostal Veins Accompany intercostal arteries and nerves Each space has posterior & anterior intercostal veins Eleven posterior intercostal and one subcostal vein Lie deepest in the costal grooves Contain valves which direct the blood posteriorly Posterior Intercostal Veins On right side: • The first space drains into the right brachiocephalic vein • Rest of the intercostal spaces drain into the azygos vein On left side: • The upper three spaces drain into the left brachiocephalic vein. • Rest of the intercostal spaces drain into the hemiazygos and accessory hemiazygos veins, which drain into the azygos vein Anterior Intercostal Veins • The lower five spaces drain into the musculophrenic vein (one of the tributary of internal thoracic vein) • The upper six spaces drain into the internal thoracic vein • The internal thoracic vein drains into the subclavian vein. Lymphatics • Anteriorly drain into anterior intercostal nodes that lie along the internal thoracic artery • Posterioly drain into posterior intercostal nodes that lie in the posterior mediastinum . -

A Functional Perspective on the Embryology and Anatomy of the Cerebral Blood Supply
Journal of Stroke 2015;17(2):144-158 http://dx.doi.org/10.5853/jos.2015.17.2.144 Review A Functional Perspective on the Embryology and Anatomy of the Cerebral Blood Supply Khaled Menshawi,* Jay P Mohr, Jose Gutierrez Department of Neurology, Columbia University Medical Center, New York, NY, USA The anatomy of the arterial system supplying blood to the brain can influence the develop- Correspondence: Jose Gutierrez ment of arterial disease such as aneurysms, dolichoectasia and atherosclerosis. As the arteries Department of Neurology, Columbia University Medical Center, 710 W 168th supplying blood to the brain develop during embryogenesis, variation in their anatomy may Street, New York, NY, 10032, USA occur and this variation may influence the development of arterial disease. Angiogenesis, Tel: +1-212-305-1710 Fax: +1-212-305-3741 which occurs mainly by sprouting of parent arteries, is the first stage at which variations can E-mail: [email protected] occur. At day 24 of embryological life, the internal carotid artery is the first artery to form and it provides all the blood required by the primitive brain. As the occipital region, brain Received: December 18, 2014 Revised: February 26, 2015 stem and cerebellum enlarge; the internal carotid supply becomes insufficient, triggering the Accepted: February 27, 2015 development of the posterior circulation. At this stage, the posterior circulation consists of a primitive mesh of arterial networks that originate from projection of penetrators from the *This work was done while Mr. Menshawi was visiting research fellow at Columbia distal carotid artery and more proximally from carotid-vertebrobasilar anastomoses. -
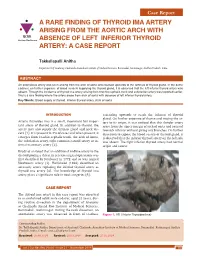
A RARE FINDING of THYROID IMA ARTERY ARISING from the AORTIC ARCH with IJCRR Section: Healthcare ABSENCE of LEFT INFERIOR THYROID ARTERY: a CASE REPORT
Case Report A RARE FINDING OF THYROID IMA ARTERY ARISING FROM THE AORTIC ARCH WITH IJCRR Section: Healthcare ABSENCE OF LEFT INFERIOR THYROID ARTERY: A CASE REPORT Takkallapalli Anitha Department of Anatomy, Chalmeda Anandrao Institute of Medical Sciences, Bommakal, Karimnagar, Andhra Pradesh, India. ABSTRACT An anomalous artery was seen arising from the arch of aorta and coursed upwards to the isthmus of thyroid gland. In the same cadaver, on further exposure of blood vessels supplying the thyroid gland, it is observed that the left inferior thyroid artery was absent. Though the incidence of thyroid ima artery arising from brachio cephalic trunk and subclavian artery was reported earlier, this is a rare finding where the artery arose from arch of aorta with absence of left inferior thyroid artery. Key Words: Blood supply of thyroid, Inferior thyroid artery, Arch of aorta INTRODUCTION ascending upwards to reach the isthmus of thyroid gland. On further exposure of thorax and tracing the ar- Arteria thyroidea ima is a small, inconstant but impor- tery to its origin, it was noticed that this slender artery tant artery of thyroid gland. In addition to thyroid, the arose from the upper margin of arch of aorta and coursed artery may also supply the thymus gland and neck vis- towards isthmus without giving any branches. On further cera [1]. It is present in 3% of cases and when present, it dissection to expose the blood vessels of thyroid gland, it emerges from brachio cephalic trunk, the arch of Aorta, is observed that the inferior thyroid artery on the left side the subclavian artery, right common carotid artery or in- was absent. -

Spontaneous Arteriovenous Malformations in the Cervical Area
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.3.303 on 1 June 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 303-309 Spontaneous arteriovenous malformations in the cervical area J. GREENBERG, M.D. From the Department of Neurology, Episcopal Hospital, Philadelphia, Pennsylvania 19125, U.S.A. SUMMARY Four patients with spontaneous arteriovenous malformations of cervical vessels have been presented. The embryology of these vessels has been discussed in order to suggest an ex- planation for the apparent difference in the incidence of arteriovenous malformations involving the internal carotid artery and those involving either the vertebral or the external carotid arteries. A fifth case (S.T.) is presented as a probable iatrogenic arteriovenous fistula and is to be added to the steadily growing reports of this phenomenon. Trauma is the most common cause of arteriovenous had sustained a minor injury to the posterior aspect communications between the blood vessels in of the right ear. Routine skull films at the time did not the cervical area (Aronson, 1961). Iatrogenic reveal a fracture, and there was no evidence of local Protected by copyright. deep tissue injury noted. fistulae occurring after carotid or vertebral angio- On the present admission, a slight prominence of the graphy are being reported with regularity in the right retroauricular region was noted and a thrill and recent literature (Sutton, 1962). Spontaneous mal- bruit were present. The bruit could be obliterated by formations in this area also occur. Thus far, eight local pressure. cases have been reported involving the vertebral The neurological examination was within normal vessels (Norman, Schmidt, and Grow, 1950; limits. -
Study on Branching Pattern of Aortic Arch in Indian
Original Article http://dx.doi.org/10.5115/acb.2012.45.3.203 pISSN 2093-3665 eISSN 2093-3673 Study on branching pattern of aortic arch in Indian Sumit Tulshidas Patil, Meena M. Meshram, Namdeo Y. Kamdi, Arun P. Kasote, Madhukar P. Parchand Department of Anatomy, Government Medical College, Nagpur, Maharashtra, India Abstract: Knowledge of the branching pattern of aortic arch is important during supra-aortic angiography, aortic instrumentation, thoracic and neck surgery. The purpose of this study is to describe different branching pattern of arch of aorta in Indian subjects, in order to offer useful data to anatomists, radiologists, vascular surgeons while relating it to the embryological basis. Seventy five arches of adult Indian cadavers were exposed and their branches examined during cadaveric dissection in the Department of Anatomy, Government Medical College, Nagpur. The usual three-branched aortic arch was found in 58 cadavers (77.3%); the 11 (14.66%) remaining aortic arch showed only two branches, out of which one was a common trunk, which incorporated the brachiocephalic trunk and left common carotid and other left subclavian artery and 6 (8%) aortic arches showed direct arch origin of the left vertebral artery. Although the variations are usually asymptomatic, they may cause dyspnoea, dysphasia, intermittent claudication, misinterpretation of radiological examinations and complications during neck and thorax surgery. Knowledge of different patterns of arch of aorta is critical when invading the arch of aorta and its branches by instruments, as all these areas are delicate. Key words: Thoracic aorta, Variations, Branches, Vascular surgery Received March 28, 2012; Revised July 5, 2012; Accepted August 23, 2012 Introduction between them. -

Comparing the Organs and Vasculature of the Head and Neck
in vivo 31 : 861-871 (2017) doi:10.21873/invivo.11140 Comparing the Organs and Vasculature of the Head and Neck in Five Murine Species MIN JAE KIM 1* , YOO YEON KIM 2* , JANET REN CHAO 3, HAE SANG PARK 1,4 , JIWON CHANG 1,4 , DAWOON OH 5, JAE JUN LEE 4,6 , TAE CHUN KANG 7, JUN-GYO SUH 2 and JUN HO LEE 1,4 1Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Hallym University, Chuncheon, Republic of Korea; 2Department of Medical Genetics, College of Medicine, Hallym University, Chuncheon, Republic of Korea; 3School of Medicine, George Washington University, Washington, DC, U.S.A.; 4Institute of New Frontier Research, Hallym University College of Medicine, Chuncheon, Republic of Korea; 5Department of Anesthesiology and Pain Medicine, Dongtan Sacred Heart Hospital, Hallym University, Dongtan, Republic of Korea; 6Department of Anesthesiology and Pain Medicine, College of Medicine, Hallym University, Chuncheon, Republic of Korea; 7Department of Anatomy and Neurobiology, College of Medicine, Hallym University, Chuncheon, Republic of Korea Abstract. Background/Aim: The purpose of the present Unique morphological characteristics were demonstrated by study was to delineate the cervical and facial vascular and comparing the five species, including symmetry of the associated anatomy in five murine species, and compare common carotid origin bilaterally in the Mongolian Gerbil, them for optimal use in research studies focused on a large submandibular gland in the hamster and an enlarged understanding the pathology and treatment of diseases in buccal branch in the Guinea Pig. In reviewing the humans. Materials and Methods: The specific adult male anatomical details, this staining technique proves superior animals examined were mice (C57BL/6J), rats (F344), for direct surgical visualization and identification. -

Ascending and Descending Thoracic Vertebral Arteries
CLINICAL REPORT EXTRACRANIAL VASCULAR Ascending and Descending Thoracic Vertebral Arteries X P. Gailloud, X L. Gregg, X M.S. Pearl, and X D. San Millan ABSTRACT SUMMARY: Thoracic vertebral arteries are anastomotic chains similar to cervical vertebral arteries but found at the thoracic level. Descending thoracic vertebral arteries originate from the pretransverse segment of the cervical vertebral artery and curve caudally to pass into the last transverse foramen or the first costotransverse space. Ascending thoracic vertebral arteries originate from the aorta, pass through at least 1 costotransverse space, and continue cranially as the cervical vertebral artery. This report describes the angiographic anatomy and clinical significance of 9 cases of descending and 2 cases of ascending thoracic vertebral arteries. Being located within the upper costotransverse spaces, ascending and descending thoracic vertebral arteries can have important implications during spine inter- ventional or surgical procedures. Because they frequently provide radiculomedullary or bronchial branches, they can also be involved in spinal cord ischemia, supply vascular malformations, or be an elusive source of hemoptysis. ABBREVIATIONS: ISA ϭ intersegmental artery; SIA ϭ supreme intercostal artery; VA ϭ vertebral artery he cervical portion of the vertebral artery (VA) is formed by a bral arteria lusoria8-13 or persistent left seventh cervical ISA of Tseries of anastomoses established between the first 6 cervical aortic origin.14 intersegmental arteries (ISAs) and one of the carotid-vertebral This report discusses 9 angiographic observations of descend- anastomoses, the proatlantal artery.1-3 The VA is labeled a “post- ing thoracic VAs and 2 cases of ascending thoracic VAs. costal” anastomotic chain (ie, located behind the costal process of cervical vertebrae or dorsal to the rib itself at the thoracic level) to CASE SERIES emphasize its location within the transverse foramina.