Guide to Fostering Change to Scale up Effective Health Services
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chad's Breach of the International Covenant on Civil and Political Rights
Chad’s Breach of the International Covenant on Civil and Political Rights: Failure to Protect the Rights of Women and Girls ABECHE, CHAD – This girl just arrived in Abeche for another fistula surgery attempt. At only 13 years of age, she suffered 3 days of labor in a remote village near the Sudan. Her resulting fistula led her to have 6 surgeries. © Micah Albert Prepared and submitted by the International Human Rights Law Society of Indiana University School of Law at Indianapolis, Indiana with the endorsement of the Program in International Human Rights of Indiana University School of Law at Indianapolis, Indiana Respectfully submitted to the United Nations Human Rights Committee on the occasion of its consideration of the First Periodic Report of Chad pursuant to Article 40 of the International Covenant on Civil and Political Rights Hearings of the United Nations Human Rights Committee New York City, U.S.A., 18-19 March 2009 © Program in International Human Rights Law, Indiana University School of Law at Indianapolis, March 2008 [THIS PAGE LEFT INTENTIONALLY BLANK] Chad’s ICCPR Breaches: Failure to Protect the Rights of Women and Girls Page 2 of 40 Author and Endorser of this Shadow Report Submitted to the United Nations Human Rights Committee on Chad’s Non-Compliance with the International Covenant on Civil & Political Rights The International Human Rights Law Society (IHRLS) is a student organization at Indiana University School of Law at Indianapolis that was formed to promote global justice and basic fundamental freedoms. Each year the IHRLS sponsors speakers and events and presents shadow reports to the United Nations Human Rights Committee through its cooperation with the Program in International Human Rights Law. -

Annual Report 2013-2014
The Museum of Fine Arts, Houston Arts, Fine of Museum The μ˙ μ˙ μ˙ The Museum of Fine Arts, Houston annual report 2013–2014 THE MUSEUM OF FINE ARTS, HOUSTON, WARMLY THANKS THE 1,183 DOCENTS, VOLUNTEERS, AND MEMBERS OF THE MUSEUM’S GUILD FOR THEIR EXTRAORDINARY DEDICATION AND COMMITMENT. ANNUAL REPORT ANNUAL 2013–2014 Cover: GIUSEPPE PENONE Italian, born 1947 Albero folgorato (Thunderstuck Tree), 2012 Bronze with gold leaf 433 1/16 x 96 3/4 x 79 in. (1100 x 245.7 x 200.7 cm) Museum purchase funded by the Caroline Wiess Law Accessions Endowment Fund 2014.728 While arboreal imagery has dominated Giuseppe Penone’s sculptures across his career, monumental bronzes of storm- blasted trees have only recently appeared as major themes in his work. Albero folgorato (Thunderstuck Tree), 2012, is the culmination of this series. Cast in bronze from a willow that had been struck by lightning, it both captures a moment in time and stands fixed as a profoundly evocative and timeless monument. ALG Opposite: LYONEL FEININGER American, 1871–1956 Self-Portrait, 1915 Oil on canvas 39 1/2 x 31 1/2 in. (100.3 x 80 cm) Museum purchase funded by the Caroline Wiess Law Accessions Endowment Fund 2014.756 Lyonel Feininger’s 1915 self-portrait unites the psychological urgency of German Expressionism with the formal structures of Cubism to reveal the artist’s profound isolation as a man in self-imposed exile, an American of German descent, who found himself an alien enemy living in Germany at the outbreak of World War I. -
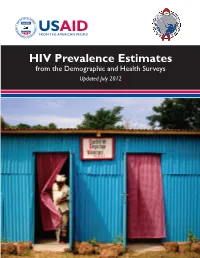
HIV Prevalence Estimates
HIV Prevalence Estimates from the Demographic and Health Surveys Updated July 2012 This report summarizes the HIV prevalence estimates provided by the MEASURE Demographic and Health Surveys (DHS) project. The MEASURE DHS project is implemented by ICF International and funded by the United States Agency for International Development (USAID). The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID. This report was prepared by Erica Nybro and Bernard Barrere, ICF International. Recommended citation: ICF International. 2012. HIV Prevalence Estimates from the Demographic and Health Surveys. Calverton, Maryland: ICF International. For more information about the MEASURE DHS project, contact: ICF International 11785 Beltsville Drive Calverton, Maryland, 20705 USA Telephone: 301-572-0200 Fax: 301-572-0999 www.measuredhs.com email: [email protected] Photos: Photos used in this report are not necessarily of individuals living with HIV/AIDS. For a full list of photo credits and captions, see inside back cover. Table of Contents Introduction 1 Summary of Surveys with HIV Prevalence 2 HIV Testing in MEASURE DHS Surveys 3 National HIV Prevalence 4 National HIV Prevalence (map) 6 Subnational HIV Prevalence (map) 7 HIV Prevalence by Sex 8 HIV Prevalence by Residence 10 HIV Prevalence by Age 12 HIV Prevalence among Children and Older Adults 13 HIV Prevalence among Youth 14 HIV Prevalence by Education 16 HIV Prevalence by Wealth 17 HIV Prevalence by Marital Status 18 HIV Prevalence by Number of Sexual Partners 19 HIV Prevalence among Couples 20 Understanding Trends in HIV Prevalence: Tanzania Case Study 21 Trends in HIV Prevalence 22 Trends in HIV Prevalence among Youth 24 Conclusions 25 Photo Credits 26 Data included in this report This report includes data from MEASURE MEASURE DHS began including HIV testing in DHS surveys. -

The IPU Resolution on Women's and Children's Health
The IPU Resolution on Women’s and Children’s Health: An Initial Framework for Accountability Reporting INTER-PARLIAMENTARY UNION Executive summary This report highlights the results from the first review of parliamentary efforts in implementing the IPU resolution of April 2012: ‘Access to health as a basic right: The role of parliaments in addressing key challenges to securing the health of women and children.’ It is based on the evidence shared by a small group of randomly selected parliaments and organizations to provide an overview of the type of actions being taken by parliaments, and to establish a process for future reporting on the implementation of the IPU resolution. Although the survey sample is small, it is representative of a significant group of parliaments and provides an indication of opinions and general trends. Participating parliaments were mostly drawn from Africa where maternal and child death rates are highest, but also from other regions, including those from two developed countries. They were Bangladesh, Canada, Ghana, Kenya, Namibia, Rwanda, South Africa, Sweden, Uganda, Zimbabwe, the East African Legislative Assembly and the Pan-African Parliament. The survey asked 40 questions about parliamentary activity on Maternal, Newborn & Child Health (MNCH) in key areas such as Political will, Awareness, Representation/Advocacy, Oversight, Legislation and Budget. The questions drilled down into topics such as determinants of health, gender equality, and accessibility and quality of health services. The efforts of participating parliaments were considered in relation to Photo: © UNICEF/RWAA2011-00386/Shehzad Noorani the commitments detailed in the IPU resolution. The survey also A female health worker performs antenatal draws on the contributions of non-parliamentary organizations, check up of a pregnant woman at a UNICEF including the Partnership for Maternal, Newborn & Child Health, supported MCH clinic (Maternal and Child) in UNFPA, WHO and World Vision International. -

Environmental Justice in Kenya: a Critical Analysis
ENVIRONMENTAL JUSTICE IN KENYA: A CRITICAL ANALYSIS by MAUREEN K NDETHIU Submitted in partial fulfilment of the degree of MASTER OF LAWS at the UNIVERSITY OF SOUTH AFRICA SUPERVISOR: PROFESSOR M BEUKES FEBRUARY 2018 DECLARATION Student Number: 3508-052-3 I, MAUREEN K NDETHIU, declare that ‘ENVIRONMENTAL JUSTICE IN KENYA: A CRITICAL ANALYSIS’ is my own work and that all the sources I have used or quoted have been indicated and acknowledged by means of complete references. 2018-02-27 Signature……………………………… Date..................................... Ndethiu M K i ABSTRACT Title of Dissertation: ENVIRONMENTAL JUSTICE IN KENYA: A CRITICAL ANALYSIS Environmental justice, a new but rapidly developing concept in international environmental law, arose in the United States of America during the Environmental Justice Movement of the late 1970s and 1980s. It starkly highlighted injustices faced by people of colour and low-income communities as regards racially skewed environmental legal protection and allocation of environmental risks. The movement radically changed the meaning of ‘environment’ from its conventional green overtones to include issues of social justice at the core of environmental thinking. I critically examine the concept of environmental justice in the Kenyan context by highlighting the injustices, and the formulation and application of laws and policies that significantly impact on environmental regulation and equitable distribution of social services. ii KEY TERMS Modern environmentalism; international environmental law; environmental principles; anthropocentrism; sustainable development; environmental justice; United States of America (USA); vulnerable and marginalised persons; human rights. iii DEDICATION To Leon and Lynn, may the achievement in this work give you a headlight to see a world of possibilities in everything you set your hearts and minds to do and to the reformists, who place their lives and families on the line so that those on the margins of society can live in dignity, justice, and hope for brighter days. -

Standards of Prevention in HIV Prevention Trials Consultation Report and Recommendations
Standards of prevention in HIV prevention trials Consultation report and recommendations 27 to 29 March 2009 Speake Resort Munyonyo Kampala, Uganda Global Campaign for Microbicides c/o PATH 1800 K Street NW, Suite 800 Washington, DC 20006, USA www.global-campaign.org Support for this project is made possible by the generous support of the American people through the United States Agency for International Development (USAID) under the terms of the HealthTech IV Cooperative Agreement #GPH-A-00-01-00005-00. DISCLAIMER: The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development, the US Centers for Disease Control and Prevention, or the United States government. Additional financial support was provided by the Joint United Nations Programme on HIV/AIDS (UNAIDS). Suggested citation: McGrory E, Philpott S, Hankins C, Paxton L, Heise L. Standards of Prevention in HIV Prevention Trials: Consultation Report and Recommendations. Washington, DC: Global Campaign for Microbicides at PATH; 2010. © 2010 Program for Appropriate Technology in Health (PATH). All rights reserved. On the cover: Photo © 2008 Micah Albert, Courtesy of Photoshare. Photo © 2000 Liz Gilbert/David and Lucile Packard Foundation, Courtesy of Photoshare. B STANDARDS OF PREVENTION IN HIV PREVENTION TRIALS Standards of prevention in HIV prevention trials Consultation report and recommendations Speake Resort Munyonyo Kampala, Uganda 27 to 29 March 2009 Convened by the Global Campaign for Microbicides, the Joint United Nations Programme on HIV/AIDS, and the United States Centers for Disease Control and Prevention Acknowledgments The authors would like to thank the many people and organisations that helped make the consultation possible, particularly the consultation speakers and participants listed in the appendix for their thoughtfulness in engaging with the complex issues raised here and in developing the recommendations listed at the end of the report. -
Annual Report 2012 Pulitzer Center on Crisis Reporting
ANNUAL REPORT 2012 Pulitzer Center on Crisis Reporting PULITZER CENTER ON CRISIS REPORTING | ANNUAL REPORT 2011 | 1 We will illuminate “dark places and, with a deep sense of responsibility, interpret these troubled times. JOSEPH PULITZER III (1913-1993)” Founded in 2006, the Pulitzer Center on Crisis Reporting is a leader in sponsoring Pulitzer Center on the independent journalism that media organizations are increasingly less able to Crisis Reporting undertake on their own. The Pulitzer Center’s mission is to raise the standard of coverage of global affairs and to do so in a way that engages the broad public and 1779 Massachusetts Avenue, NW government policy-makers. Suite 615 Washington, DC 20036 The Pulitzer Center is a bold initiative, in keeping with its sponsorship by a family whose name for more than a century has been a watchword for journalistic 202-332-0982 independence, integrity and courage. The Center is a 501(c)(3) non-profit organization. www.pulitzercenter.org TABLE OF CONTENTS Letter from Board Chair and Executive Director 3 2012 Reporting Projects 6 Campus Consortium 12 Student Fellows 15 Global Gateway 17 Event Highlights 19 Social Media 20 E-Books 25 Awards and Honors 26 Staff, Board of Directors and Advisory 28 Council ” Donors 29 Contact Information and Credits 30 PULITZER CENTER ON CRISIS REPORTING | ANNUAL REPORT 2012 | 1 nuns for GlobalPost and National Catholic Reporter to Beenish Ahmed’s story-behind-the-story of the young Pakistani girl who symbolized that country’s struggle for gender equality—and was subsequently shot in the head LETTER FROM BOARD CHAIR by the Taliban. -
State of School Feeding Worldwide 2013 II
Fighting Hunger Worldwide State of School Feeding Worldwide 2013 Published in 2013 by the World Food Programme Via C.G. Viola, 68-70, Rome 00148, Italy This publication is the product of the staff of the World Food Programme (WFP). The views expressed in the book do not necessarily reflect the official position of WFP, its Executive Director or its Executive Board or its partners. The mention of specific companies or products in this publication does not imply that these have been endorsed or recommended by WFP. Maps The designations employed and the presentation of the material in this publication, including in maps, do not imply the expression of any opinion whatsoever on the part of the World Food Programme concerning the legal status of any country, territory, city or area, or concerning the delimitation of its frontiers and boundaries. In the following specific cases: * the Line of Control in Jammu and Kashmir agreed on by India and Pakistan is represented approximately by a dotted line as the final status has not yet been agreed on by the parties; ** a dispute exists between the governments of Argentina and the United Kingdom concerning sovereignty over the Falkland Islands (Malvinas); *** the final boundary between the Republic of Sudan and the Republic of South Sudan has not yet been determined. Rights and Permissions All rights reserved. Reproduction and dissemination of material in this publication for educational or other non-commercial purposes is authorized without any prior written permission from the copyright holder, provided the source is fully acknowledged. Reproduction of material in this publication for resale or other commercial purposes is prohibited without the prior written permission of the copyright holder. -
The Pulitzer Center's Roots
The Pulitzer Center: Filling the Gap in International Journalism By James O’Shea October 2014 Table of Contents Overview Pages 1-5 Genesis of Report Page 5 The State of International Reporting Pages 5-11 The Pulitzer Center’s Roots Pages 11-15 The Pulitzer Mission Pages 15-17 The Pulitzer Model Pages 18-28 The Center’s Finances Pages 28-33 Pulitzer’s Brand of Non-profit Journalism Pages 33-41 Pulitzer’s Education Arm Pages 41-49 The Pulitzer Center’s Impact Pages 49-56 Conclusions Pages 56-62 About the Author Page 62 Overview When it launched in 2006, the Pulitzer Center on Crisis Reporting seemed like a journalistic rowboat plying the treacherous seas of global news coverage. Today it’s a lifeboat for intrepid journalists determined to navigate those waters. Operating with modest resources and a relatively small crew, the Center, in the past nine years, has assembled an impressive log of journalistic and educational achievements despite the declining number of news organizations with dedicated foreign news staffs. A non-profit started with a small grant from the family whose name is synonymous with quality journalism, the Pulitzer Center solicits donations from foundations and generous individuals and converts the money into small grants for journalists working exclusively on international stories across a variety of media platforms. David Boardman, dean of the School of Media and Communications at Temple University and former editor of the Seattle Times, thinks Pulitzer’s impact equals that of major foundations such as the John L. and James Knight Foundation, one of the nation’s largest funders of journalism projects. -

A 3UNFPA Annual Report 2008 CC.Indd
ANNUAL REPORT 2008 Resources and Management 1 Photos: Cover: A young Guatemalan girl raising her hand during class. The girl, a student at a school in El Llano, is participating in a UNFPA-supported programme that aims to increase opportunities for adolescent indigenous girls. © Mark Tuschman Foreword: Ban Ki-moon, Secretary-General of the United Nations. © Mark Garten/United Nations From the Executive Director: Thoraya Ahmed Obaid, Executive Director of UNFPA. © Eskinder Debebe/United Nations Reproductive Health and Safe Motherhood: Clients waiting at a UNFPA-supported clinic in Panama. The clinic serves the indigenous Ngöbe-Buglé people, who are among the poorest in Latin America. © Carina Wint for UNFPA Culture, Gender and Human Rights: A Bolivian father carrying his son. © Tom Weller Helping in Emergencies: A young girl getting water at a UNFPA-assisted camp for internally displaced persons in Chad. © Micah Albert Poverty, Population and Development: A fi sherman casts his net in the water along Wataboo beach in Baucau, Timor-Leste. © Martine Perret/United Nations Building Support: UNFPA Goodwill Ambassador Geri Halliwell in front of the United States Capitol building, where she met with members of Congress in February. The singer spoke with legislators about the serious health issues facing women and mothers worldwide. © MJ Kim Resources and Management: A student couple receiving counselling on safe sex and family planning at a youth-friendly service centre located at the University Hospital in Ankara, Turkey. UNFPA provides equipment -

Employment Promotion in Contexts of Conflict, Fragility and Violence
Employment Promotion in Contexts of Conflict, Fragility and Violence Opportunities and Challenges for Peacebuilding Published by 02 Crisis areas worldwide Acronyms and Abbreviations AfDB African Development Bank 03 BMZ Federal Ministry for Economic Cooperation and Development CFV Conflict, fragility and violence CHF Common Humanitarian Fund CIMIC Civil-Military Cooperation CSR Corporate Social Responsibility DCED Donor Committee for Enterprise Development DFID Department for International Development DRC Democratic Republic of Congo ELMA Employment and Labour Market Analysis GIZ Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH GTZ Deutsche Gesellschaft für Technische Zusammenarbeit (GTZ) GmbH IDEA Integrated Development of Entrepreneurial Activities IDPs Internally Displaced Persons IEG Independent Evaluation Group IFC International Finance Corporation ILO International Labour Organization IRC International Rescue Committee LEAP Liberian Employment Action Plan M&E Monitoring and Evaluation NGO Non-Governmental Organisation ODA Official Development Assistance OECD Organisation for Economic Cooperation and Development PPD Public-Private Dialogue PPP Public-Private Partnership PSD Private Sector Development SEED Sustainable Employment and Economic Development SMEs Small and medium-sized Enterprises SNV Stichting Nederlandse Vrijwilligers UN United Nations UNDP United Nations Development Programme UNHCR United Nations High Commissioner for Refugees UNIDO United Nations Industrial Development Organization USAID United States -

Futurethe Impacts of Climate Change on Food Security and Nutrition in the Middle East and North Africa
Food in an uncertain The impacts of climate change on food security and nutrition in the future Middle East and North Africa Food in an uncertain future 1 World Food Programme Regional Bureau for Middle East, North Africa, Eastern Europe and Central Asia, Contents Nile Gardenia Building, Intersection of Roads 108 & 161, Hadaek El Maadi, Cairo, Egypt. http://www.wfp.org 3 Acknowledgments 4 Overseas Development Institute Executive Summary 203 Blackfriars Road 6 London Introduction SE1 8NJ 10 Tel. +44 (0) 20 7922 0300 Current food security in the Middle East and North Africa Fax. +44 (0) 20 7922 0399 The macro-picture: challenges in national food systems and strategies E-mail: [email protected] The status of household food security and nutrition www.odi.org The geography of food insecurity www.odi.org/facebook 22 www.odi.org/twitter The future climate of the Middle East and North Africa A hotter, drier future: long term trends The views presented in this paper are those of the More frequent, more intense extremes authors and do not necessarily represent the views 28 of ODI or the World Food Programme. The impacts of climate change on food security How will food producers be affected? © World Food Programme 2015. All rights reserved. How will climate change affect food production? Which food producers will be most vulnerable? All ODI Reports are available from www.odi.org How will food consumers be affected? Climate is not only the only change: intersections with other trends 42 Options for building resilience and reducing risk Strengthen food systems and economic development for all Improve the yields, income, and choices of poor food producers 48 Conclusions 50 References 2 Food in an uncertain future Food in an uncertain future 1 Acknowledgements Authors: Guy Jobbins and Giles Henley, The authors would like to thank Oscar Ekdahl and Overseas Development Institute Carlo Scaramella at the World Food Programme for their oversight of, and contributions to, the report.