Patterns of Orbital Disorders
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Turn-Over Orbital Septal Flap and Levator Recession for Upper-Eyelid
Eye (2013) 27, 1174–1179 & 2013 Macmillan Publishers Limited All rights reserved 0950-222X/13 www.nature.com/eye 1 2 3 1 CLINICAL STUDY Turn-over orbital A Watanabe , PN Shams , N Katori , S Kinoshita and D Selva2 septal flap and levator recession for upper-eyelid retraction secondary to thyroid eye disease Abstract Background A turn-over septal flap has been Keywords: upper-eyelid retraction; orbital reported as a spacer for levator lengthening septal flap; levator recession in a single case report. This study reports the preliminary outcomes of this technique in a series of patients with upper-lid retraction (ULR) associated with thyroid eye disease 1Department of Ophthalmology, Introduction Kyoto Prefectural University of (TED) causing symptomatic exposure Medicine, Kyoto, Japan keratopathy (EK). Achieving a predictable eyelid height and Methods Retrospective, multicenter study contour in the surgical correction of upper- 2 Department of Ophthalmology of 12 eyelids of 10 patients with TED eyelid retraction remains a challenge for and Visual Sciences, South Australian Institute of undergoing a transcutaneous levator- surgeons, as evidenced by the variety of Ophthalmology, Adelaide lengthening technique using the reflected procedures reported.1,2 These techniques are University, Adelaide, South orbital septum (OS) as a spacer. Change in based on weakening or lengthening the Australia, Australia palpebral aperture (PA) and contour, position upper-eyelid retractors and include anterior or 3Department of Oculoplastic of the skin crease (SC), symptoms of EK, and posterior approaches to graded recession and Orbital Surgery, Seirei complications were recorded. or resection of Mu¨ ller’s muscle,3–5 levator Hamamatsu Hospital, Results The average age was 47.5 years. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
The Orbit Is Composed Anteri
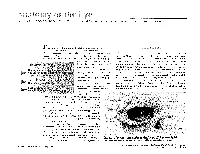
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Pediatric Orbital Tumors and Lacrimal Drainage System
Pediatric Orbital Tumors and Lacrimal Drainage System Peter MacIntosh, MD University of Illinois • No financial disclosures Dermoid Cyst • Congenital • Keratinized epidermis • Dermal appendage • Trapped during embryogenesis • 6% of lesions • 40-50% of orbital pediatric orbital lesion • Usually discovered in the first year of life • Painless/firm/subQ mass • Rarely presents as an acute inflammatory lesion (Rupture?) • Frontozygomatic (70%) • Maxillofrontal (20%) suture Imaging - CT • Erosion/remodeling of bone • Adjacent bony changes: “smooth fossa” (85%) • Dumbell dermoid: extraorbital and intraorbital components through bony defect Imaging - MRI • Encapsulated • Enhancement of wall but not lumen Treatment Options • Observation • Risk of anesthesia • Surgical Removal • Changes to bone • Rupture of cyst can lead to acute inflammation • Irrigation • Abx • Steroids Dermoid INFANTILE/Capillary Hemangioma • Common BENIGN orbital lesion of children • F>M • Prematurity • Appears in 1st or 2nd week of life • Soft, bluish mass deep to the eyelid • Superonasal orbit • Rapidly expands over 6-12 months • Increases with valsalva (crying) • Clinical findings • Proptosis Astigmatism • Strabismus Amblyopia INFANTILE/Capillary Hemangioma • May enlarge for 1-2 years then regress • 70-80% resolve before age 7 • HIGH flow on doppler • Kasabach-Merritt Syndrome • Multiple large visceral capillary hemangiomas • Sequestration of platelets into tumor • Consumptive thrombocytopenia • Supportive therapy and treat underlying tumor • Complications • DIC • death •Homogenous -

Stage Surgery on Inverted Papilloma Which Invaded Lacrimal Sac, Periorbita, Ethmoid and Frontal Sinus
臨床耳鼻:第 27 卷 第 1 號 2016 ••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••• J Clinical Otolaryngol 2016;27:143-147 증 례 Stage Surgery on Inverted Papilloma which Invaded Lacrimal Sac, Periorbita, Ethmoid and Frontal Sinus Jae-hwan Jung, MD, Minsic Kim, MD, Sue Jean Mun, MD and Hwan-Jung Roh, MD, PhD Department of Otorhinolaryngology-Head & Neck Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea - ABSTRACT - Inverted papilloma of the nasal cavity and the paranasal sinuses is a benign epithelial tumor with a high rate of recurrence, local aggressiveness, and malignant transformation. For these reasons, inverted papilloma has been treated like malignant tumors with extensive surgical resection. With the help of endoscopic sinus surgery tech- nique, it is now available to treat inverted papilloma with stage surgery without severe complications which usu- ally resulted from extensive one stage resection. We report a case of stage surgery on inverted papilloma which invaded lacrimal sac, periorbita, ethmoid and frontal sinus. (J Clinical Otolaryngol 2016;27:143-147) KEY WORDS:Inverted papillomaㆍLacrimal sacㆍPeriorbitaㆍSurgery. Authors present a successful endoscopic stage sur- Introduction gery on IP which invaded lacrimal sac, periorbita, ethmoid and frontal sinus with the literature review. Inverted papilloma (IP) of the nasal cavity and the paranasal sinuses is a benign epithelial tumor with a Case Report high rate of recurrence, local aggressiveness, and ma- lignant transformation.1,2) For these reasons, IP has A 41-year-old female presented in outpatient clinic been treated like malignant tumors with extensive sur- with a complaint of tender swelling mass on the in- gical resection. ner side of her right eye for 5 years which suddenly IP of lacrimal sac and periorbita is rarely reported aggravated 2 months ago. -

Eyelash Inversion in Epiblepharon: Is It Caused by Redundant Skin?
ORIGINAL RESEARCH Eyelash inversion in epiblepharon: Is it caused by redundant skin? Hirohiko Kakizaki1 Purpose: To evaluate the effect of redundant lower eyelid skin on the eyelash direction in Igal Leibovitch2 epiblepharon. Yasuhiro Takahashi3 Materials and methods: Asian patients with epiblepharon participated in this study. The Dinesh Selva4 lower eyelid skin was pulled downward in the upright position with the extent just to detach from eyelash roots, and the direction of the eyelashes was examined. These evaluations were 1Department of Ophthalmology, Aichi Medical University, Nagakute, repeated before surgery while the patients were lying supine under general anesthesia. Aichi 480-1195, Japan; 2Division of Results: The study included 41 lower eyelids of 25 patients (17 females, 8 males, average age; Oculoplastic and Orbital Surgery, 5.6 years, 16 cases bilateral, 9 unilateral). In the upright position, without downward traction Department of Ophthalmology, Tel-Aviv Medical Center, of the skin, the eyelashes were vertically positioned and touching the cornea. The redundant Tel-Aviv University, Tel-Aviv, Israel; skin touched only the eyelash roots and had minimal contribution to eyelash inversion. With 3 Department of Ophthalmology downward skin traction, there was no signifi cant change in the eyelash direction. In the spine and Visual Sciences, Osaka City University Graduate School position, the eyelashes were touching the cornea, and there was marked redundant skin that was of Medicine, Osaka 545-8585, Japan; pushing the eyelashes inward. With downward skin traction, there was no signifi cant change. 4 South Australian Institute Conclusions: The direction of lower eyelashes in patients with epiblepharon was less infl uenced of Ophthalmology and Discipline For personal use only. -

Results Description of the SKULLS. the Overall Size of Both Skulls Was Considered to Be Within Normal Limits for Their Ethnic
Ossification Defects and Craniofacial Morphology In Incomplete Forms of Mandibulofacial Dysostosis A Description of Two Dry Skulls ERIK DAHL, D.D.S., DR. ODONT. ARNE BJORK, D.D.S., ODONT. DR. Copenhagen, Denmark The morphology of two East Indian dry skulls exhibiting anomalies which were suggested to represent incomplete forms of mandibulofacial dysostosis is described. Obvious although minor ossification anomalies were found localized to the temporal, sphenoid, the zygomatic, the maxillary and the mandibular bones. The observations substantiate the concept of the regional and bilateral nature of this malformation syndrome. Bilateral orbital deviations, hypoplasia of the malar bones, and incomplete zygomatic arches appear to be hard tissue aberrations which may be helpful in exami- nation for subclinical carrier status. Changes in mandibular morphology seem to be less distinguishing features in incomplete or abortive types of mandibulofacial dysostosis. KEY WORDS craniofacial problems, mandible, mandibulofacial dysostosis, maxilla, sphenoid bone, temporal bone, zygomatic bone Mandibulofacial dysostosis (MFD) often roentgencephalometric examinations were results in the development of a characteristic made of the skulls, and tomograms were ob- facial disfigurement with considerable simi- tained of the internal and middle ear. Com- larity between affected individuals. However, parisons were made with normal adult skulls the symptoms may vary highly in respect to and with an adult skull exhibiting the char- type and degree, and both incomplete and acteristics of MFD. All of the skulls were from abortive forms of the syndrome have been the same ethnic group. ' reported in the literature (Franceschetti and Klein, 1949; Moss et al., 1964; Rogers, 1964). Results In previous papers, we have shown the DEsCRIPTION OF THE SKULLS. -

Original Article Anatomic Study of the Lacrimal Fossa and Lacrimal Pathway
Original Article Anatomic study of the lacrimal fossa and lacrimal pathway for bypass surgery with autogenous tissue grafting Hai Tao, Zhi‑zhong Ma1, Hai‑Yang Wu, Peng Wang, Cui Han Purpose: To study the microsurgical anatomy of the lacrimal drainage system and to provide anatomical Access this article online evidence for transnasal endoscopic lacrimal drainage system bypass surgery by autogenous tissue grafting. Website: Materials and Methods: A total of 20 Chinese adult cadaveric heads in 10% formaldehyde, comprising www.ijo.in 40 lacrimal ducts were used. The middle third section of the specimens were examined for the following DOI: features: the thickness of the lacrimal fossa at the anterior lacrimal crest, vertical middle line, and posterior 10.4103/0301-4738.121137 lacrimal crest; the cross section of the upper opening, middle part, and lower opening of the nasolacrimal PMID: canal; the horizontal, 30° oblique, and 45° oblique distances from the lacrimal caruncle to the nasal cavity; ***** the distance from the lacrimal caruncle to the upper opening of the nasolacrimal duct; and the included Quick Response Code: angle between the lacrimal caruncle–nasolacrimal duct upper opening junction and Aeby’s plane. Results: The middle third of the anterior lacrimal crest was significantly thicker than the vertical middle line and the posterior lacrimal crest (P > 0.05). The horizontal distance, 30° oblique distance, and 45° oblique distance from the lacrimal caruncle to the nasal cavity exhibited no significant differences (P > 0.05). The included angle between the lacrimal caruncle and the lateral wall middle point of the superior opening line of the nasolacrimal duct and Aeby’s plane was average (49.9° ± 1.8°). -

Surgical Anatamic of Paranasal Sinuses
SURGICAL ANATAMIC OF PARANASAL SINUSES DR. SEEMA MONGA ASSOCIATE PROFESSOR DEPARTMENT OF ENT-HNS HIMSR MIDDLE TURBINATE 1. Anterior attachment : vertically oriented, sup to the lateral border of cribriform plate. 2. Second attachment :Obliquely oriented- basal lamella/ ground lamella, Attached to the lamina papyracea ( medial wall of orbit anterior, posterior air cells, sphenopala‐ tine foramen 3. Posterior attachment :medial wall of maxillary sinus, horizontally oriented. , supreme turbinate 3. Occasionally 4. fourth turbinate, 5. supreme meatus, if present 6. drains posterior ethmoid drains inferior, middle, superior turbinates and, occasionally, the supreme turbinate, the fourth turbinate. e. Lateral to these turbinates are the corresponding meatuses divided per their drainage systems ANATOMICAL VARIATIONS OF THE TURBINATES 1. Concha bullosa, 24–55%, often bilateral, 2. Interlamellar cell of grunwald: pneumatization is limited to the vertical part of middle turbinate, usually not causing narrowing of the ostiomeatal unit 3. Paradoxic middle turbinate: 26%,. Occasionally, it can affect the patency of the ostiomeatal unit 4. Pneumatized basal lamella, falsely considered, posterior ethmoid air cell Missed basal lamella – attaches to lateral maxillary sinus wall Ostiomeatal unit Anterior ostiomeatal unit, maxillary, anterior ethmoid, frontal sinuses, (1) ethmoid infundibulum, (2) middle meatus, (3) hiatus semilunaris, (4) maxillaryOstium, (5) ethmoid bulla, (6) frontal recess, (7) uncinate process. , sphenoethmoidal recess Other draining osteomeatal unit, posterior in the nasal cavity, posterior ethmoid sinus, lateral to the superior turbinate, . sphenoid Sinus medial to the superior turbinate Uncinate Process Crescent‐shaped, thin individual bone inferiorly- ethmoidal process of inferior turbinate, anterior, lacrimal bone, posteriorly- hiatus Semilunaris, medial -ethmoid infundibulum, laterally, middle meatus superior attachment- variability, direct effect on frontal sinus drainage pathway. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina