Departmental Syllabus Form
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Respiratory Therapy Program
UNIVERSITY OF THE DISTRICT OF COLUMBIA RESPIRATORY THERAPY PROGRAM The University offers the A.A.S. Degree in Respiratory ASSOCIATE IN APPLIED SCIENCE DEGREE IN Therapy. The curriculum reflects high standards of RESPIRATORY THERAPY professional practice and incorporates guidelines from practice trends, professional organizations and accrediting Total Credit Hours of College-Level Courses Required agencies. Students develop the knowledge base and For Graduation: 70 clinical competencies required to meet the health care needs of patients with cardiopulmonary disorders. The program offers both a day and an evening option. Respiratory Therapists treat patients along the age and health-care continuums – from premature infants to the PROGRAM OF STUDY aged in critical care, acute care, rehabilitation, and home care settings. PREREQUISITES 1535-101 General College Math I 3 ACCREDITATION & CREDENTIALING 1133-111 English Composition I 3 1401-112 Anatomy and Physiology II – Lecture 3 The UDC Respiratory Therapy Program is accredited by 1401-114 Anatomy and Physiology II – Lab 1 the Commission on Accreditation of Allied Health Total 10 Credits Education Programs (CAAHEP), in collaboration with the FIRST YEAR – FALL SEMESTER Committee on Accreditation for Respiratory Care 1431-170 Introduction to Health Sciences 2 1431-171 Principles and Practice of Resp Therapy I 4 (CoARC). Graduates are eligible for both the entry-level licensure/ CRT examination (required by the District of 1401-112 Anatomy and Physiology II – Lecture 3 Columbia, Maryland and Virginia) and the advanced 1401-114 Anatomy and Physiology II – Lab 1 1133-112 or 1535-102 English Composition II or practice RRT examinations, both offered by the National Board for Respiratory Care (NBRC). -

Table of Contents 1
GENERAL THORACIC SURGERY DATABASE v.2.3 TRAINING MANUAL August 2017 Table of Contents 1. Demographics ................................................................................................................................................................. 2 2. Follow Up ........................................................................................................................................................................ 9 3. Admission ..................................................................................................................................................................... 10 4. Pre-Operative Evaluation ............................................................................................................................................. 14 5. Diagnosis (Category of Disease) ................................................................................................................................... 48 6. Procedure ..................................................................................................................................................................... 70 7. Post-Operative Events ................................................................................................................................................ 111 8. Discharge .................................................................................................................................................................... 135 9. Quality Measures ...................................................................................................................................................... -

Respiratory Therapy Handbook
WASHINGTON STATE COMMUNITY COLLEGE RESPIRATORY THERAPY STUDENT HANDBOOK 2020-2021 Written: July, 1996 Revised: December, 2020 TABLE OF CONTENTS Statement of Non-Discrimination…………………………………………………………………………….. 2 Introduction……………………………………………………………………………………………………………..3 Goal………………………………………………………………………………………………………………………5-6 Accreditation……………………………………………………………………………………………………………6 Program Organization………………………………………………………………………………………………7 Plan for Consistency of Clinical Instruction & Evaluation of Clinical courses, Preceptors & Clinical Sites…………………………………………………………………………………………………………9 STUDENT POLICIES Course of Study………………………………………………………………………………………………………11 Student Schedule/Class sessions……………………………………………………………………………..11 Clinical Experiences…………………………………………………………………………………………..11-12 Tardiness……………………………………………………………………………………………………………….12 Absenteeism, Clinical…………………………………………………………………………………………12-13 Absenteeism, Classroom………………………………………………………………………………………….13 Absenteeism, Lab……………………………………………………………………………………………….13-14 Clinical Evaluations……………………………………………………………………………………………15-16 Clinical Competency…………………………………………………………………………………………..17-20 ACADEMIC POLICIES Clinical Evaluation Forms…………………………………………………………………………………..15-16 Clinical Competency Evaluation………………………………………………………………………….17-20 Promotion………………………………………………………………………………………………………………21 Evaluation………………………………………………………………………………………………………………21 Remediation …………………………………………………………………………………………………………..22 Probation/Dismissal……………………………………………………………………………………………….22 Leave of Absence…………………………………………………………………………………………………….22 -

Oxygen Policy 2018
Oxygen Policy Document Control Title Oxygen Policy (Prescribing & Administration of Oxygen to Adults in Hospital Policy) Author Author’s job title Consultant Physician, Respiratory Medicine Clinical Development Facilitator Directorate Department Division of Medicine, A&E and Comm. Respiratory Hospitals Date Version Status Comment / Changes / Approval Issued June 0.1 Draft Draft presented to Medical Gases Committee. 2010 1.0 Jun Final Approved at Clinical Services Executive Committee 2010 (CSEC) in 14th June 2010. Approved by Drugs and Therapeutics Committee on July 1st 2010. 1.1 Dec Revision Minor amendments by Corporate Affairs to document 2010 control report, filename, header and footer, formatting for document map navigation. Hyperlinks to appendices and Trust procedural documents. Update to document control report. Amendments to section 8 and 24.1. 1.2 Dec Revision Appendix F added 2017 Re wording/re-ordering of most sections Minor alteration to section 5.2 Sepsis 6 added to section 5.2 Addition of endoscopy and ED to 5.8 1.3 June Revision Appendix G added 2018 Minor alteration to section 5.4 2.0 June Final Approved by all members of the Medical Gas Committee 2018 Main Contact Consultant Physician Tel: Direct Dial – 01271 349589 Level 5 Tel: Internal – Ext No. 3375 North Devon District Hospital Raleigh Park Barnstaple, EX31 4JB Lead Director Medical Director Superseded Documents Issue Date Review Date Review Cycle June 2018 June 2021 3 years Respiratory Team Oxygen Policy Page 1 of 39 Oxygen Policy Consulted with the following stakeholders: -
Oxygen Therapy and Oxygen Delivery (Pediatric) - CE
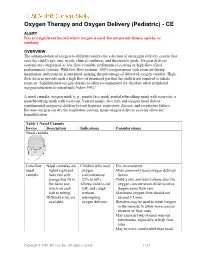
Oxygen Therapy and Oxygen Delivery (Pediatric) - CE ALERT Fire is a significant hazard where oxygen is used. Do not permit flames, sparks, or smoking. OVERVIEW The administration of oxygen to children requires the selection of an oxygen delivery system that suits the child’s age, size, needs, clinical condition, and therapeutic goals. Oxygen delivery systems are categorized as low-flow (variable performance) systems or high-flow (fixed performance) systems. With low-flow systems, 100% oxygen mixes with room air during inspiration, and room air is entrained, making the percentage of delivered oxygen variable. High- flow devices provide such a high flow of premixed gas that the child is not required to inhale room air. Supplemental oxygen therapy is often recommended for children when peripheral oxygen saturation is consistently below 94%.1 A nasal cannula, oxygen mask (e.g., simple face mask, partial rebreathing mask with reservoir, a nonrebreathing mask with reservoir, Venturi mask), face tent, and oxygen hood deliver supplemental oxygen to children to treat hypoxia, respiratory distress, and respiratory failure. Because oxygen can dry the respiratory system, many oxygen delivery systems allow for humidification. Table 1 Nasal Cannula Device Description Indications Considerations Nasal cannula Low-flow Nasal cannulas are Children who need FIO2 inconsistent. nasal lightweight and oxygen Most commonly used oxygen delivery cannula have two soft concentrations device. prongs that fit in 22% to 60%. Child’s size and tidal volume alter the the nares and Allows child to eat, oxygen concentration child receives attach on each talk, and cough despite same flow rate. side to tubing. without Maximum oxygen flow should not Different sizes are interrupting exceed 4 L/min. -

Respiratory Therapy (RTH) 1
Respiratory Therapy (RTH) 1 RTH-205. Cardiopulmonary Pathophysiology. 2 Credits. Respiratory Therapy LECT 2 hrs An overview of the pathophysiology of diseases of the (RTH) cardiopulmonary system with an emphasis on pathophysiologic processes such as hypoxemia, hypoventilation, diffusion defects and ventilation perfusion mismatch; a survey of diseases encountered Courses by the respiratory therapist, including pathophysiology, diagnostic RTH-199. Respiratory Therapeutics. 5 Credits. methods and findings, clinical manifestations, treatment and LECT 4 hrs, LAB 3 hrs prognosis. An introduction to respiratory care, including history of the Prerequisites: RTH-203 and permission of program director. profession, ethical and legal responsibilities of the respiratory RTH-206. Mechanical Ventilation. 4 Credits. therapist; medical terminology, basic respiratory care procedures LECT 3 hrs, LAB 3 hrs including the physics, physiology and administration of medical Techniques of airway management and the provision of mechanical gas therapy, basic patient communication and assessment skills. ventilation; includes types of airways and appropriate uses; the Basic respiratory care procedures, humidity and aerosol therapy, physics and physiology of mechanical ventilation; classification hyperinflation therapy, chest physiotherapy and bronchial hygiene; of mechanical ventilators; indications for clinical application an overview of microbiology as applied to respiratory care; infection and complications of mechanical ventilation; management control; and equipment sterilization procedures. Course requires and monitoring of the patient requiring ventilatory support; and that students have completed the pre-professional phase of the appropriate methods of withdrawing ventilatory support. Respiratory Therapy program and have permission of the program Prerequisites: RTH-199, RTH-202, RTH-203, RTH-210 and director to enroll. permission of program director Prerequisites: Permission of Program Director Corequisites: RTH-204, RTH-205 and RTH-211 Additional Fees: Course fee applies. -

ICD-9-CM Procedures (FY10)
2 PREFACE This sixth edition of the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) is being published by the United States Government in recognition of its responsibility to promulgate this classification throughout the United States for morbidity coding. The International Classification of Diseases, 9th Revision, published by the World Health Organization (WHO) is the foundation of the ICD-9-CM and continues to be the classification employed in cause-of-death coding in the United States. The ICD-9-CM is completely comparable with the ICD-9. The WHO Collaborating Center for Classification of Diseases in North America serves as liaison between the international obligations for comparable classifications and the national health data needs of the United States. The ICD-9-CM is recommended for use in all clinical settings but is required for reporting diagnoses and diseases to all U.S. Public Health Service and the Centers for Medicare & Medicaid Services (formerly the Health Care Financing Administration) programs. Guidance in the use of this classification can be found in the section "Guidance in the Use of ICD-9-CM." ICD-9-CM extensions, interpretations, modifications, addenda, or errata other than those approved by the U.S. Public Health Service and the Centers for Medicare & Medicaid Services are not to be considered official and should not be utilized. Continuous maintenance of the ICD-9- CM is the responsibility of the Federal Government. However, because the ICD-9-CM represents the best in contemporary thinking of clinicians, nosologists, epidemiologists, and statisticians from both public and private sectors, no future modifications will be considered without extensive advice from the appropriate representatives of all major users. -

RSP-241 Neonatal and Pediatric Respiratory Care
Bergen Community College Division of Health Professions Department of Respiratory Care RSP-241 NEONATAL/PEDIATRIC RESPIRATORY CARE COURSE SYLLABUS Semester and Year: Course and Section Number: RSP-241 Lab sections 001-004 Meeting Times and Locations: Lecture Tuesday 8:20-10:15AM, Room HP-302. Labs: Monday 08:20-10:15, Monday 10:30-12:30PM, Tuesday 10:30-12:30, Wednesday 12:00-2:00PM. All labs are held in room HP-230. Instructor: Office Location: Phone: Departmental Secretary: Office Hours: Tuesday Email Address: Course Description List lecture hours, laboratory hours, and credits: 2.0 lectures, 2.0 labs, 3.0 credits List prerequisites and co-requisites: Prerequisites: RSP 110,119,121, 210,220, 222,225,226,231,240,250 Co-requisites: RSP 235, 260. Course Description: This course provides a comprehensive overview of pediatric and neonatal respiratory care. Special considerations of respiratory care practice unique to pediatrics and neonatology are discussed. Topics include pediatric anatomy and physiology, fetal development, clinical assessment, oxygen therapy, airway management, mechanical ventilation, resuscitation, cardiopulmonary pathophysiology and disorders specific to this specialty profession within respiratory care. Course Content 1 This course is intended to introduce students to the basic fundamental concepts of neonatal-pediatric respiratory therapy. The course begins with the foundations of respiratory care such as patient assessment skills of the neonate and pediatric patient. The course then covers basic therapeutics including infant and child CPR, airway management, medical gas therapy and delivery, aerosol and humidity therapy, aerosol drug therapy, lung expansion therapy and bronchial hygiene therapy. The course culminates to provide an in depth understanding of all aspects of fetal development, circulation, neonatal and pediatric airway diseases, mechanical ventilation, nasal CPAP management and homecare of the neonatal/pediatric patient. -

Anesthesia for Video-Assisted Thoracoscopic Surgery
23 Anesthesia for Video-Assisted Thoracoscopic Surgery Edmond Cohen Historical Considerations of Video-Assisted Thoracoscopy ....................................... 331 Medical Thoracoscopy ................................................................................................. 332 Surgical Thoracoscopy ................................................................................................. 332 Anesthetic Management ............................................................................................... 334 Postoperative Pain Management .................................................................................. 338 Clinical Case Discussion .............................................................................................. 339 Key Points Jacobaeus Thoracoscopy, the introduction of an illuminated tube through a small incision made between the ribs, was • Limited options to treat hypoxemia during one-lung venti- first used in 1910 for the treatment of tuberculosis. In 1882 lation (OLV) compared to open thoracotomy. Continuous the tubercle bacillus was discovered by Koch, and Forlanini positive airway pressure (CPAP) interferes with surgi- observed that tuberculous cavities collapsed and healed after cal exposure during video-assisted thoracoscopic surgery patients developed a spontaneous pneumothorax. The tech- (VATS). nique of injecting approximately 200 cc of air under pressure • Priority on rapid and complete lung collapse. to create an artificial pneumothorax became a widely used • Possibility -

2017-2018 Respiratory Therapy
2017-2018 General Catalog 1 RET - Respiratory Therapy RET 1004, Introduction to Science I 1 hr., 1 cr., This one credit course will introduce fundamental principles, theories, and laws of chemistry relevant to the respiratory therapy practitioner. RET 1005, Respiratory Microbiology 1 hr., 1 cr., A review of microbiology as it relates to the profession of respiratory care. Topics include microbiological identification, surveillance, and equipment processing. RET 1024, Respiratory Therapy I 3 hrs., 3 crs., Prerequisite: Program acceptance. Corequisite: *RET1024L, *RET1832. This introductory course will cover the practice and basic concepts of respiratory vital signs, patient assessment, medical gas therapy, oxygen therapy, humidity, aerosol, and hyperinflation therapies. RET 1024L, Respiratory Therapy I Lab 4 hrs., 2 crs., $55.00 lab fee Corequisite: *RET1024, *RET1832. This lab complements the lecture in RET 1024. This course will introduce the student to the practice and basic concepts of respiratory therapy. Topics will include professional ethics, diversity, licensure and credentialing, infection control, vital signs, patient assessment, medical gas therapy, oxygen therapy, humidity, aerosol, and hyperinflation therapies. RET 1264, Respiratory Therapy II 3 hrs., 3 crs., Prerequisites: *RET1024, *RET1024L, *RET1832. Corequisites: RET1264L/1272L, RET1833. This course will cover the theory, practice and mastery of equipment used in hyperinflation therapy, pulmonary mechanics, bronchial hygiene therapies, medication nebulizer therapy, airway care, and arterial blood gas analysis. RET 1264L, Respiratory Therapy II Lab 4 hrs., 2 crs., $121.00 lab fee Prerequisites: *RET1024, *RET1024L, *RET1832. Corequisites: RET1264, RET1833. This lab complements the lecture in RET 1264. Through practice and performance tests the student will demonstrate the mastery of equipment used in Hyperinflation Therapy, Pulmonary Mechanics, Bronchial Hygiene Therapies, Medication Nebulizer Therapy, Airway Care, and Arterial Blood Gas Analysis. -

Circulatory Collapse Due to Hyperinflation in a Patient with Tracheobronchomalacia: a Case Report and Brief Review
Hindawi Case Reports in Critical Care Volume 2019, Article ID 2921819, 5 pages https://doi.org/10.1155/2019/2921819 Case Report Circulatory Collapse due to Hyperinflation in a Patient with Tracheobronchomalacia: A Case Report and Brief Review Niclas Lundström ,1 Gert Henriksson,2 Ola Börjesson,3 Malin Jonsson Fagerlund,1 and Johan Petersson1 Function Perioperative Medicine and Intensive Care (PMI), Karolinska University Hospital, Sweden Department of ENT Surgery, Karolinska University Hospital, Sweden Department of Rheumatology, Karolinska University Hospital, Sweden Correspondence should be addressed to Niclas Lundstr¨om; [email protected] Received 13 December 2018; Accepted 13 January 2019; Published 29 January 2019 Academic Editor: Kenneth S. Waxman Copyright © 2019 Niclas Lundstr¨om et al. Tis is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. We present a case of repeated cardiac arrests derived from dynamic hyperinfation in a patient with severe tracheobronchomalacia. Mechanical ventilation led to auto-PEEP with hemodynamic impairment and pulseless electric activity. Adjusted ventilation settings, deep sedation, and muscle paralysis followed by acute stenting of the afected collapsing airways restored ventilation and prevented recurrent circulatory collapse. We briefy review the pathophysiology and treatment options in patients with dynamic hyperinfation. 1. Introduction tracheobronchial infammation had led to stenosis and sec- ondary tracheobronchomalacia, with the distal trachea and Patients with expiratory fow limitation are at risk of devel- main bronchi most afected on previous CT scans. At the oping dynamic hyperinfation and auto-PEEP, which in time of the reported events, he received treatment with extreme cases can cause circulatory collapse [1]. -

Tracheal and Bronchial Surgery
Tracheal and Bronchial Surgery 1A031 Honorary Editors: Douglas E. Wood, Douglas J. Mathisen, Erino Angelo Rendina Editors: Xiaofei Li, Federico Venuta, David C. van der Zee Associate Editors: Dirk Van Raemdonck, Federico Rea, Jinbo Zhao Xiaofei Li, Federico Venuta, David C. van der Zee Xiaofei Li, Federico Venuta, Editors: Tracheal and Bronchial Surgery Honorary Editors: Douglas E. Wood, Douglas J. Mathisen, Erino Angelo Rendina Editors: Xiaofei Li, Federico Venuta, David C. van der Zee Associate Editors: Dirk Van Raemdonck, Federico Rea, Jinbo Zhao AME Publishing Company Room C 16F, Kings Wing Plaza 1, NO. 3 on Kwan Street, Shatin, NT, Hong Kong Information on this title: www.amegroups.com For more information, contact [email protected] Copyright © AME Publishing Company. All rights reserved. This publication is in copyright. Subject to statutory exception and to the provisions of relevant collective licensing agreements, no reproduction of any part may take place without the written permission of AME Publishing Company. First published 2017 Printed in China by AME Publishing Company Editors: Xiaofei Li, Federico Venuta, David C. van der Zee Cover Image Illustrator: Zhijing Xu, Shanghai, China Tracheal and Bronchial Surgery Hardcover ISBN: 978-988-77841-8-0 AME Publishing Company, Hong Kong AME Publishing Company has no responsibility for the persistence or accuracy of URLs for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate. The advice and opinions expressed in this book are solely those of the author and do not necessarily represent the views or practices of AME Publishing Company.