Highlands & Islands Case Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

0131 656 3201 Chair
Westport 102 West Port Edinburgh EH3 9DN Telephone: 0131 656 3200 Fax: 0131 656 3201 www.nes.scot.nhs.uk st Date: 31 August 2016 Your Ref: 20/7/16 Our Ref: The Health and Sports Committee The Scottish Parliament Edinburgh EH99 1SP Dear Mr Findlay Recruitment and Retention Many thanks for your letter dated 20th July 2016 on behalf of the Health and Support Committee seeking a response from NHS Education for Scotland (NES) on issues relating to recruitment and retention, with a focus on remote and rural recruitment. We note your observations on the data published by Information Services Division (ISD) and that you are seeking to understand how the training and education system is coping and adapting to ensure there are sufficient numbers of graduates to fill medical posts and that they are then retained within the NHS. 1. Context In addition to our role in medical training, NES plays an increasing role in supporting recruitment and retention within other areas of the NHSScotland workforce. As the national training and education board for NHSScotland we have a key remit in supporting the whole service to deliver on all five strands of the Everyone Matters: 2020 Workforce Vision: Healthy Organisational Culture; Sustainable Workforce; Capable Workforce; Integrated Workforce; and Effective Leadership and Management. The principal role of NES is in the education and training of the NHS Scotland workforce. While we provide significant quantities of information on the workforce-in-training, decisions on the numbers in training (particularly in the so-called controlled subjects of medicine, nursing and dentistry) are for Scottish Ministers on the advice of officials. -

FUTURE FOREST the BLACK WOOD RANNOCH, SCOTLAND
Gunnar’s Tree with the community, Nov. 23, 2013 (Collins & Goto Studio, 2013). FUTURE FOREST The BLACK WOOD RANNOCH, SCOTLAND Tim Collins and Reiko Goto Collins & Goto Studio, Glasgow, Scotland Art, Design, Ecology and Planning in the Public Interest with David Edwards Forest Research, Roslin, Scotland The Research Agency of the Forestry Commission Developed with: The Rannoch Paths Group Anne Benson, Artist, Chair, Rannoch and Tummel Tourist Association, Loch Rannoch Conservation Association. Jane Dekker, Rannoch and Tummel Tourist Association. Jeannie Grant, Tourism Projects Coordinator, Rannoch Paths Group. Bid Strachan, Perth and Kinross Countryside Trust. The project partners Charles Taylor, Rob Coope, Peter Fullarton, Tay Forest District, Forestry Commission Scotland. David Edwards and Mike Smith, Forest Research, Roslin. Paul McLennan, Perth and Kinross Countryside Trust. Richard Polley, Mark Simmons, Arts and Heritage, Perth and Kinross Council. Mike Strachan, Perth and Argyll Conservancy, Forestry Commission Scotland. Funded by: Creative Scotland: Imagining Natural Scotland Programme. The National Lottery / The Year of Natural Scotland. The Landscape Research Group. Forestry Commission Scotland. Forest Research. Future Forest: The Black Wood, Rannoch, Scotland Tim Collins, Reiko Goto and David Edwards Foreword by Chris Quine The Landscape Research Group, a charity founded in 1967, aims to promote research and understanding of the landscape for public benefit. We strive to stimulate research, transfer knowledge, encourage the exchange of ideas and promote practices which engage with landscape and environment. First published in UK, 2014 Forest Research Landscape Research Group Ltd Northern Research Station PO Box 1482 Oxford OX4 9DN Roslin, Midlothian EH25 9SY www.landscaperesearchgroup.com www.forestry.gov.uk/forestresearch © Crown Copyright 2014 ISBN 978-0-9931220-0-2 Paperback ISBN 978-0-9931220-1-9 EBook-PDF Primary funding for this project was provided by Creative Scotland, Year of Natural Scotland. -

Health Impact Assessment of Rural Development: a Guide
Health Impact Assessment of Rural Development: a Guide SHIIAN ScotPHN May 2015 INTRODUCTION ................................................................................................................................. 3 RURAL SCOTLAND ............................................................................................................................ 4 Heterogeneity of rural areas ............................................................................................................ 7 Demography and health in rural Scotland ....................................................................................... 7 Determinants of health in rural communities ................................................................................... 9 Rural Policy .................................................................................................................................... 11 COMMON HEALTH IMPACTS OF RURAL DEVELOPMENT .......................................................... 14 Population movement .................................................................................................................... 14 Psychosocial impacts..................................................................................................................... 15 Social capital .................................................................................................................................. 15 Employment .................................................................................................................................. -

The Typological Study of the Structures of the Scottish Brochs Roger Martlew*
Proc Soc Antiq Scot, 112 (1982), 254-276 The typological study of the structures of the Scottish brochs Roger Martlew* SUMMARY brieA f revie f publishewo d work highlight varyine sth g qualit f informatioyo n available th n eo structural features of brochs, and suggests that the evidence is insufficient to support the current far- reaching theories of broch origins and evolution. The use of numerical data for classification is discussed, and a cluster analysis of broch dimensions is presented. The three groups suggested by this analysis are examined in relation to geographical location, and to duns and 'broch-like' structures in Argyll. While the method is concluded to be useful, an improve- qualit e mendate th th necessar s an f i i t y o improvyo t interpretationd ai resulte o et th d san . INTRODUCTION AND REVIEW OF PUBLISHED WORK The brochs of Scotland have attracted a considerable amount of attention over the years, from the antiquarians of the last century to archaeologists currently working on both rescue and research projects. Modern development principlee th n si techniqued san excavationf so , though, have been applie vero brochsdt w yfe . Severa excavatione th f o lpase decade w th fe tf o s s have indeed been more careful research-orientated projects tha indiscriminate nth e diggin lase th t f go century, when antiquarians seemed intent on clearing out the greatest number of brochs in the shortest possible time. The result, however, is that a considerable amount of material from brochs exists in museum collections, but much of it is from excavations carried out with slight regard for stratigraphy and is consequently of little use in answering the detailed questions set by modern hypotheses. -

Consultant Obstetrician and Gynaecologist
Consultant Obstetrician and Gynaecologist Candidate Information Pack Job ref: 064391 Closing date: Sunday 3RD October 2021 Interview date: Friday 22nd October 2021 1 Candidate Information Pack Candidate Information Pack ........................................................................................................... 2 Welcome ........................................................................................................................................ 3 Introduction to Orkney .................................................................................................................... 5 Introduction to the Appointment...................................................................................................... 7 Advert .......................................................................................................................................... 10 Job Description ............................................................................................................................ 11 Indicative Job Plan ....................................................................................................................... 17 Person Specification .................................................................................................................... 19 Terms and Conditions of Service ................................................................................................. 21 General Information for Candidates ............................................................................................ -

Candidate Information
Candidate Information Putting quality first to deliver better health, better care and better value http://www.nhshighland.scot.nhs.uk https://twitter.com/NHSHighland www.facebook.com/NHSHighland/ www.linkedin.com/company/nhs-highland https://nhshighland.medical.careers.global Contents Welcome from The Chief Executive. 3 Board Objectives 2019 / 2020 . 5 Highland Quality Approach Strategic Framework . 6 About NHS Highland . 7 NHS Highland Operational Units . 10 Delivering our Acute Services . 11 NHS Highland: at a glance . 14 Research, Development and Innovation . 15 Corporate highlights . 17 All NHS Highland Hospitals . 19 Breakdown of staff numbers . 20 Useful NHS Highland Websites . 21 Good to know . 22 Welcome from The Chief Executive T hank you for your interest in NHS Highland. I hope the information we have put together in this pack will encourage you to consider joining our team of health and care professionals who strive to deliver quality improvement and innovation from some of the most beautiful scenery in the world. Our diverse area includes In recent years, NHS Highland has Inverness, one of the fastest made significant strides to further growing cities in Western improve health and social care Europe as well as many provision across the region, often remote and rural communities. leading the way by introducing Because of our geography we new models and new methods of provide, with excellent clinical delivering care. In 2012, for example, outcomes, a far wider range we became the first health board in of services than expected the country to integrate health and for our size. The breadth and social care. depth of clinical expertise is significant. -
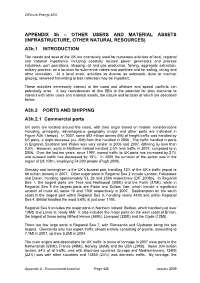
OTHER USERS and MATERIAL ASSETS (INFRASTRUCTURE, OTHER NATURAL RESOURCES) A3h.1 INTRODUCTION
Offshore Energy SEA APPENDIX 3h – OTHER USERS AND MATERIAL ASSETS (INFRASTRUCTURE, OTHER NATURAL RESOURCES) A3h.1 INTRODUCTION The coasts and seas of the UK are intensively used for numerous activities of local, regional and national importance including coastally located power generators and process industries, port operations, shipping, oil and gas production, fishing, aggregate extraction, military practice, as a location for submarine cables and pipelines and for sailing, racing and other recreation. At a local scale, activities as diverse as saltmarsh, dune or machair grazing, seaweed harvesting or bait collection may be important. These activities necessarily interact at the coast and offshore and spatial conflicts can potentially arise. A key consideration of this SEA is the potential for plan elements to interact with other users and material assets, the nature and location of which are described below. A3h.2 PORTS AND SHIPPING A3h.2.1 Commercial ports UK ports are located around the coast, with their origin based on historic considerations including, principally, advantageous geography (major and other ports are indicated in Figure A3h.1 below). In 2007, some 582 million tonnes (Mt) of freight traffic was handled by UK ports, a slight decrease (ca. 2Mt) from that handled in 2006. The traffic handled in ports in England, Scotland and Wales was very similar in 2006 and 2007, differing by less than 0.5%. However, ports in Northern Ireland handled 2.5% less traffic in 2007, compared to in 2006. Over the last ten years, since 1997, inward traffic to UK ports has increased by 21% and outward traffic has decreased by 15%. -
Infrastructure Investment Plan 2015 Progress Report for 2017
Infrastructure Investment Plan 2015 Progress Report for 2017 CONTENTS Foreword 1 Overview Report 2 Sector Reports Transport 8 Health 11 Schools 16 Early Learning and Childcare 17 Further and Higher Education 18 Culture, Heritage and Tourism 19 Justice 20 Digital 23 Energy 25 Water 29 Rural Economy and the Environment 31 Housing 33 Regeneration 36 Cities / Regions 38 April 2018 Foreword Infrastructure investment is at the heart of our economic strategy and this annual progress report on our Infrastructure Investment Plan outlines key achievements over the course of the last year and looks forward to developments during this year and beyond. Since 2007 we have delivered major infrastructure improvements for the people of Scotland and significant progress continues to be made as demonstrated by this report and by our accompanying published pipeline of project activity. In 2017 we delivered major infrastructure priorities such as the opening of the Queensferry Crossing, the largest bridge of its type and a complex engineering feat. We saw the completion of the so-called ‘missing link’ between Glasgow and Edinburgh with the opening of the M8 M73 M74 Motorway Improvements Project and the first section of A9 Dualling Programme was completed with the opening of the Kincraig to Dalraddy section. We saw one of the most advanced hospitals in the country completed with the opening of the new Dumfries & Galloway Royal Infirmary as well as the completion of the Scottish National Blood Transfusion Service’s new national centre at the Heriot-Watt Research Park in Edinburgh. Over the course of the last year we also saw no fewer than forty one school projects completed within the Scottish Government supported Schools for the Future building programme. -

NHS Highland CONSULTANT ANAESTHETIST
NHS Highland CONSULTANT ANAESTHETIST Lorn & Islands Hospital VACANCY Consultant in Anaesthesia Lorn & Islands Hospital 40 hours per week £80,653 (GBP) to £107,170 (GBP) per annum Tenure: Permanent Applications are invited to join our Anaesthetics team at Lorn & Islands Hospital, Oban on the beautiful West Coast of Scotland. This vacancy is offered on the basis of 10 Programmed Activities per week. The department of Anaesthetics is based at Lorn & Islands Hospital, Oban. The Hospital is located on the southern outskirts of Oban and forms a hub for both acute and community services within the area. Purpose built in 1995, the Hospital houses a full range of facilities expected in a rural general hospital including a full 24 hour medical, surgical and anaesthetic service. Duties are based at Lorn and the Islands Hospital with some sessions at the Argyll and Bute Mental Health Hospital in Lochgilphead. There is the possibility of further clinic sessions at community hospitals throughout Argyll. The area is of one of outstanding natural beauty, the town of Oban is a tourist and commercial centre for the West of Scotland and the Isles. The port town has ferry links to the islands of Mull, Iona, Islay, Coll, Tiree, Colonsay and Lismore. There is plenty of opportunity for enjoying leisure pursuits including yachting, canoeing, walking, climbing, cycling and fishing. It’s a great place to bring up a family with good local schools and reasonable property prices. Oban provides the advantage of a high quality of life in a rural setting with access to the main centres of Glasgow, Stirling and Perth all within 2½ hours travel time. -

Price Thresholds Apply
Maximum Local Threshold Prices LIFT Open Market Shared Equity Scheme – WEST What is an apartment? 1 bedroom + 1 living room = 2 apartments. 1 bedroom + 1 living room + 1 dining room = 3 apartments. 2 bedrooms + 1 living room = 3 apartments, and so on. Updated December 2020 These prices will be subject to review Area Number of Apartments* Maximum price Argyll and Bute 2 £70,000 Argyll and Bute 3 £105,000 Argyll and Bute 4 £135,000 Argyll and Bute 5 £180,000 Argyll and Bute 6 £240,000 Dumfries and Galloway 2 £70,000 Dumfries and Galloway 3 £90,000 Dumfries and Galloway 4 £115,000 Dumfries and Galloway 5 £155,000 Dumfries and Galloway 6 £210,000 Glasgow 2 £70,000 Glasgow 3 £85,000 Glasgow 4 £95,000 Glasgow 5 £160,000 Glasgow 6 £230,000 East Renfrewshire 2 £70,000 East Renfrewshire 3 £110,000 East Renfrewshire 4 £145,000 East Renfrewshire 5 £205,000 East Renfrewshire 6 £305,000 East Dunbartonshire 2 £85,000 East Dunbartonshire 3 £110,000 East Dunbartonshire 4 £155,000 East Dunbartonshire 5 £200,000 East Dunbartonshire 6 £305,000 Inverclyde 2 £40,000 Inverclyde 3 £55,000 Inverclyde 4 £65,000 Inverclyde 5 £80,000 Inverclyde 6 £175,000 Renfrewshire 2 £55,000 Renfrewshire 3 £70,000 Renfrewshire 4 £90,000 Renfrewshire 5 £115,000 Renfrewshire 6 £205,000 North Ayrshire 2 £45,000 North Ayrshire 3 £55,000 North Ayrshire 4 £65,000 North Ayrshire 5 £80,000 Area Number of Apartments* Maximum price North Ayrshire 6 £165,000 East Ayrshire 2 £50,000 East Ayrshire 3 £70,000 East Ayrshire 4 £90,000 East Ayrshire 5 £125,000 East Ayrshire 6 £190,000 North Lanarkshire -

Ministerial Strategic Group for Health and Community Care
MINISTERIAL STRATEGIC GROUP FOR HEALTH AND COMMUNITY CARE Paper no: MSGHCC/127/2020 Meeting date: 22 January 2020 Agenda item: 5 Purpose: For action / note Title: Overview of Integration Authority Strategic Commissioning Plans 2019 - 2022 Key This paper provides an overview of Integration Authority Strategic Issues: Commissioning Plans 2019 – 2022. The overview identifies key messages and covers key elements including: Scope of plans; Reach and quality of engagement; Strategic needs assessment, strategic priorities and financial planning. Action The MSG is invited to agree: Required: In conjunction with the progress update on the integration review and in particular proposals at 3 (iv) and 3 (v) to note this overview. That the key messages are widely shared in order to promote learning and continuous improvement in strategic commissioning processes and practice. Author: Eilidh Love Christina Naismith Date: January 2020 January 2020 1 MINISTERIAL STRATEGIC GROUP FOR HEALTH AND COMMUNITY CARE Introduction 1. All Integration Authorities have now revised their strategic commissioning plan, maintaining, realigning or setting their vision for the next 3 years, as required by the Public Bodies (Joint Working) (Scotland) Act 2014. 2. Integration Authorities are responsible for planning, designing and commissioning services in an integrated way from a single budget in order to take a joined up approach, more easily shifting resources to best meet need. They have a duty to publish a strategic commissioning plan for integrated functions and budgets under their control. Collectively, Integration Authorities manage almost £9 billion of resources that Health Boards and Local Authorities previously managed separately, and have the power and authority to drive real change. -

Health in a Changing Scotland
Health IN A CHANGING SCOTLAND The ball’s in our court CALL FOR ABSTRACTS ANNUAL PUBLIC HEALTH CONFERENCE Thursday 6 & Friday 7 November 2014 Macdonald Aviemore Resort Faculty of Public Health Committee of the Faculty of Public Health in Scotland www.fphscotconf.co.uk Announcement of Conference and Call for Abstracts Conference registration Further information regarding registration and accommodation costs will be available in the conference registration brochure which will be circulated in July/August. Please note that acceptance of an abstract Health in a Changing Scotland or shorter presentation application does not provide a free place at the conference. All abstract presenters, including those selected to make oral presentations, are The ball’s in our court required to register in the usual way. A limited number of reduced fee places will be available for delegates unable to secure The title and cover picture for this year’s conference are full funding to attend the conference. The conference plenary sessions will be made intended to reflect 2 key events in 2014 which could have available for those who would like to join the significant implications for Public Health in Scotland – the conference by video-conferencing. Independence Referendum and the Commonwealth Games (although not on the 2014 programme, tennis has long been Conference organisation on the list of approved optional Commonwealth Games sports). By the time of the conference both of these will have This year’s annual Scottish Public Health Conference is being organised by the taken place, and this provides an ideal time to discuss how Faculty of Public Health in partnership with we can proactively use the opportunities that the Games and the North of Scotland Health Boards and Referendum provide to shape the health of our population and comprises the following planning group the structures that support this.