Vedrop, INN-Tocofersolan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

London, 29 May 2009 Doc.Ref
European Medicines Agency Pre-Authorisation Evaluation of Medicines for Human Use London, 29 May 2009 Doc.Ref. EMEA/CHMP/282149/2009 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE SUMMARY OF POSITIVE OPINION* for VEDROP International Nonproprietary Name (INN): tocofersolan On 29 May 2009 the Committee for Medicinal Products for Human Use (CHMP) adopted a positive opinion, recommending to grant a marketing authorisation under exceptional circumstances for the medicinal product Vedrop, 50 mg/ml, oral solution indicated in vitamin E deficiency due to digestive malabsorption in paediatric patients suffering from congenital chronic cholestasis or hereditary chronic cholestasis. The applicant for this medicinal product is Orphan Europe S.A.R.L. The active substance of Vedrop is tocofersolan, an alimentary tract and metabolism medicinal product (ATC code A11 HA08, other plain vitamin preparations). Tocofersolan, is vitamin E that has been made water-soluble by attaching it to polyethylene glycol 1000, and thereby can be absorbed from the gut in patients who have difficulty absorbing fats and vitamin E from the diet due congenital chronic or hereditary chronic cholestasis. The use of vitamin E preparations in this population helps to prevent neurological deterioration due to vitamin E deficiency. The benefits with Vedrop are improvement or stabilisation of neurological abnormalities due to vitamin E deficiency in patients with congenital chronic or hereditary chronic cholestasis. The most common side effect is diarrhoea. A pharmacovigilance plan for Vedrop, as for all medicinal products, will be implemented as part of the marketing authorisation. The approved indication is: “Vedrop is indicated in vitamin E deficiency due to digestive malabsorption in paediatric patients suffering from congenital chronic cholestasis or hereditary chronic cholestasis, from birth (in term newborns) to 16 or 18 years of age, depending on the region”. -

Annexes to the EMA Annual Report 2009
Annual report 2009 Annexes The main body of this annual report is available on the website of the European Medicines Agency (EMA) at: http://www.ema.europa.eu/htms/general/direct/ar.htm 7 Westferry Circus ● Canary Wharf ● London E14 4HB ● United Kingdom Telephone +44 (0)20 7418 8400 Facsimile +44 (0)20 7418 8416 E-mail [email protected] Website www.ema.europa.eu An agency of the European Union © European Medicines Agency, 2010. Reproduction is authorised provided the source is acknowledged. Contents Annex 1 Members of the Management Board..................................................... 3 Annex 2 Members of the Committee for Medicinal Products for Human Use .......... 5 Annex 3 Members of the Committee for Medicinal Products for Veterinary Use ....... 8 Annex 4 Members of the Committee on Orphan Medicinal Products .................... 10 Annex 5 Members of the Committee on Herbal Medicinal Products ..................... 12 Annex 6 Members of the Paediatric Committee................................................ 14 Annex 7 National competent authority partners ............................................... 16 Annex 8 Budget summaries 2008–2009 ......................................................... 27 Annex 9 European Medicines Agency Establishment Plan .................................. 28 Annex 10 CHMP opinions in 2009 on medicinal products for human use .............. 29 Annex 11 CVMP opinions in 2009 on medicinal products for veterinary use.......... 53 Annex 12 COMP opinions in 2009 on designation of orphan medicinal products -

Estonian Statistics on Medicines 2016 1/41
Estonian Statistics on Medicines 2016 ATC code ATC group / Active substance (rout of admin.) Quantity sold Unit DDD Unit DDD/1000/ day A ALIMENTARY TRACT AND METABOLISM 167,8985 A01 STOMATOLOGICAL PREPARATIONS 0,0738 A01A STOMATOLOGICAL PREPARATIONS 0,0738 A01AB Antiinfectives and antiseptics for local oral treatment 0,0738 A01AB09 Miconazole (O) 7088 g 0,2 g 0,0738 A01AB12 Hexetidine (O) 1951200 ml A01AB81 Neomycin+ Benzocaine (dental) 30200 pieces A01AB82 Demeclocycline+ Triamcinolone (dental) 680 g A01AC Corticosteroids for local oral treatment A01AC81 Dexamethasone+ Thymol (dental) 3094 ml A01AD Other agents for local oral treatment A01AD80 Lidocaine+ Cetylpyridinium chloride (gingival) 227150 g A01AD81 Lidocaine+ Cetrimide (O) 30900 g A01AD82 Choline salicylate (O) 864720 pieces A01AD83 Lidocaine+ Chamomille extract (O) 370080 g A01AD90 Lidocaine+ Paraformaldehyde (dental) 405 g A02 DRUGS FOR ACID RELATED DISORDERS 47,1312 A02A ANTACIDS 1,0133 Combinations and complexes of aluminium, calcium and A02AD 1,0133 magnesium compounds A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 811120 pieces 10 pieces 0,1689 A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 3101974 ml 50 ml 0,1292 A02AD83 Calcium carbonate+ Magnesium carbonate (O) 3434232 pieces 10 pieces 0,7152 DRUGS FOR PEPTIC ULCER AND GASTRO- A02B 46,1179 OESOPHAGEAL REFLUX DISEASE (GORD) A02BA H2-receptor antagonists 2,3855 A02BA02 Ranitidine (O) 340327,5 g 0,3 g 2,3624 A02BA02 Ranitidine (P) 3318,25 g 0,3 g 0,0230 A02BC Proton pump inhibitors 43,7324 A02BC01 Omeprazole -

Patent Application Publication ( 10 ) Pub . No . : US 2019 / 0192440 A1
US 20190192440A1 (19 ) United States (12 ) Patent Application Publication ( 10) Pub . No. : US 2019 /0192440 A1 LI (43 ) Pub . Date : Jun . 27 , 2019 ( 54 ) ORAL DRUG DOSAGE FORM COMPRISING Publication Classification DRUG IN THE FORM OF NANOPARTICLES (51 ) Int . CI. A61K 9 / 20 (2006 .01 ) ( 71 ) Applicant: Triastek , Inc. , Nanjing ( CN ) A61K 9 /00 ( 2006 . 01) A61K 31/ 192 ( 2006 .01 ) (72 ) Inventor : Xiaoling LI , Dublin , CA (US ) A61K 9 / 24 ( 2006 .01 ) ( 52 ) U . S . CI. ( 21 ) Appl. No. : 16 /289 ,499 CPC . .. .. A61K 9 /2031 (2013 . 01 ) ; A61K 9 /0065 ( 22 ) Filed : Feb . 28 , 2019 (2013 .01 ) ; A61K 9 / 209 ( 2013 .01 ) ; A61K 9 /2027 ( 2013 .01 ) ; A61K 31/ 192 ( 2013. 01 ) ; Related U . S . Application Data A61K 9 /2072 ( 2013 .01 ) (63 ) Continuation of application No. 16 /028 ,305 , filed on Jul. 5 , 2018 , now Pat . No . 10 , 258 ,575 , which is a (57 ) ABSTRACT continuation of application No . 15 / 173 ,596 , filed on The present disclosure provides a stable solid pharmaceuti Jun . 3 , 2016 . cal dosage form for oral administration . The dosage form (60 ) Provisional application No . 62 /313 ,092 , filed on Mar. includes a substrate that forms at least one compartment and 24 , 2016 , provisional application No . 62 / 296 , 087 , a drug content loaded into the compartment. The dosage filed on Feb . 17 , 2016 , provisional application No . form is so designed that the active pharmaceutical ingredient 62 / 170, 645 , filed on Jun . 3 , 2015 . of the drug content is released in a controlled manner. Patent Application Publication Jun . 27 , 2019 Sheet 1 of 20 US 2019 /0192440 A1 FIG . -

Medicintilskudsnævnet
Medicintilskudsnævnet Sundhedsstyrelsen Axel Heides Gade 1 2300 København S 20. juni 2014 Sagsnr: 2013111157 Revurdering af tilskudsstatus for lægemidler i ATC- gruppe A09- digestiva, inkl. enzy- mer, A11-vitaminer, A12- mineralpræparater og A16 - andre midler til fordøjelsesorganer og stofskifte Baggrund og indhold Vi har revurderet tilskudsstatus for lægemidler i ATC- gruppe A09- digestiva, inkl. enzymer, A11- vitaminer, A12- mineralpræparater og A16 - andre midler til fordøjelsesorganer og stofskifte. Bilag A er en grafisk oversigt over lægemiddelstofferne. I ATC-gruppe A16 er der en række lægemid- ler, som er begrænset til udlevering til sygehuse (udleveringsgruppe ”BEGR”). Disse lægemidler er ikke omfattet af indstillingen. Denne indstilling er en samlet indstilling for alle lægemidler i ATC-gruppe A09, A11, A12 og A16, der fremgår af bilag B, og som er godkendt til markedsføring i Danmark, og som per den 18. juni 2014 er eller har været markedsført i Danmark. Nedenfor følger først vores indstilling til lægemidlernes fremtidige tilskudsstatus, derefter en kort gen- nemgang af revurderingsforløbet samt vores begrundelser i relation til den anbefalede fremtidige til- skudsstatus. Bilag B er en oversigt over lægemiddelstofferne med angivelse af hvilke lægemidler, der er omfattet af denne revurdering, de godkendte indikationer for de pågældende lægemidler, udleveringsgruppe, gæl- dende tilskudsstatus, årligt forbrug i årene 2009-2013 samt antal ansøgninger om enkelttilskud, hvor dette er relevant. Indstilling til fremtidig tilskudsstatus Vi indstiller følgende til Sundhedsstyrelsen: 1. Lægemidler i ATC-gruppe A09 (digestiva, inkl. enzymer) med indhold af pancreatin (amylase, lipase, protease) (A09AA02) bevarer gældende tilskudsstatus: ikke generelt tilskud. Medicintilskudsnævnet 1 Sekretariatet - Axel Heides Gade 1 – 2300 København S Medicintilskudsnævnet 2. -

Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DIX to the HTSUS—Continued
20558 Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DEPARMENT OF THE TREASURY Services, U.S. Customs Service, 1301 TABLE 1.ÐPHARMACEUTICAL APPEN- Constitution Avenue NW, Washington, DIX TO THE HTSUSÐContinued Customs Service D.C. 20229 at (202) 927±1060. CAS No. Pharmaceutical [T.D. 95±33] Dated: April 14, 1995. 52±78±8 ..................... NORETHANDROLONE. A. W. Tennant, 52±86±8 ..................... HALOPERIDOL. Pharmaceutical Tables 1 and 3 of the Director, Office of Laboratories and Scientific 52±88±0 ..................... ATROPINE METHONITRATE. HTSUS 52±90±4 ..................... CYSTEINE. Services. 53±03±2 ..................... PREDNISONE. 53±06±5 ..................... CORTISONE. AGENCY: Customs Service, Department TABLE 1.ÐPHARMACEUTICAL 53±10±1 ..................... HYDROXYDIONE SODIUM SUCCI- of the Treasury. NATE. APPENDIX TO THE HTSUS 53±16±7 ..................... ESTRONE. ACTION: Listing of the products found in 53±18±9 ..................... BIETASERPINE. Table 1 and Table 3 of the CAS No. Pharmaceutical 53±19±0 ..................... MITOTANE. 53±31±6 ..................... MEDIBAZINE. Pharmaceutical Appendix to the N/A ............................. ACTAGARDIN. 53±33±8 ..................... PARAMETHASONE. Harmonized Tariff Schedule of the N/A ............................. ARDACIN. 53±34±9 ..................... FLUPREDNISOLONE. N/A ............................. BICIROMAB. 53±39±4 ..................... OXANDROLONE. United States of America in Chemical N/A ............................. CELUCLORAL. 53±43±0 -

Vitamin C 09/07/2007 10:34 AM
Vitamin C 09/07/2007 10:34 AM Vitamin C BOTTOM LINE MONOGRAPH A concise evidence-based review, designed for use by patients or professionals. Based on systematic aggregation and analysis of scientific literature, historic/folkloric precedent, and expert consultation. Edited and peer-reviewed blindly by Natural Standard editorial contributors. Includes information on effectiveness, side effects, interactions, dosing, pregnancy and breastfeeding. English | Spanish FLASHCARD Quick look-up or patient handout. Easy reading level for consumers. Adapted from a Natural Standard comprehensive professional evidence-based systematic review. Concise information includes brief summary, uses, safety, side effects, interactions and dosing. Click Here NEWS ITEMS August 2007--Omega-3 and Vitamins for Bed Sore Prevention: Omega-3 acid and vitamin supplementation may help prevent bed sores in hospitalized patients, a new study reports.... August 2007--Antioxidants for Bone Health: A diet rich in antioxidants, such as vitamins C and E, may help improve bone health reducing the risk of osteoarthritis, a new study suggests.... July 2007--Vitamin C for the Common Cold: How Effective is it?: Vitamin C supplementation may not reduce the risk of the common cold in the normal population, contrary to popular belief and use, a new review reports.... July 2007--FDA: Tomatoes and Cancer: The U.S. Food and Drug Administration (FDA) has released a review that found only limited evidence for a correlation between eating tomatoes, rich in lycopene, and a decreased risk of certain cancers.... July 2007--Pomegranate Juice for Erectile Dysfunction: Pomegranate juice may help treat erectile dysfunction, a new study suggests. However, evidence remains inconclusive at this time... -

Estonian Statistics on Medicines 2013 1/44
Estonian Statistics on Medicines 2013 DDD/1000/ ATC code ATC group / INN (rout of admin.) Quantity sold Unit DDD Unit day A ALIMENTARY TRACT AND METABOLISM 146,8152 A01 STOMATOLOGICAL PREPARATIONS 0,0760 A01A STOMATOLOGICAL PREPARATIONS 0,0760 A01AB Antiinfectives and antiseptics for local oral treatment 0,0760 A01AB09 Miconazole(O) 7139,2 g 0,2 g 0,0760 A01AB12 Hexetidine(O) 1541120 ml A01AB81 Neomycin+Benzocaine(C) 23900 pieces A01AC Corticosteroids for local oral treatment A01AC81 Dexamethasone+Thymol(dental) 2639 ml A01AD Other agents for local oral treatment A01AD80 Lidocaine+Cetylpyridinium chloride(gingival) 179340 g A01AD81 Lidocaine+Cetrimide(O) 23565 g A01AD82 Choline salicylate(O) 824240 pieces A01AD83 Lidocaine+Chamomille extract(O) 317140 g A01AD86 Lidocaine+Eugenol(gingival) 1128 g A02 DRUGS FOR ACID RELATED DISORDERS 35,6598 A02A ANTACIDS 0,9596 Combinations and complexes of aluminium, calcium and A02AD 0,9596 magnesium compounds A02AD81 Aluminium hydroxide+Magnesium hydroxide(O) 591680 pieces 10 pieces 0,1261 A02AD81 Aluminium hydroxide+Magnesium hydroxide(O) 1998558 ml 50 ml 0,0852 A02AD82 Aluminium aminoacetate+Magnesium oxide(O) 463540 pieces 10 pieces 0,0988 A02AD83 Calcium carbonate+Magnesium carbonate(O) 3049560 pieces 10 pieces 0,6497 A02AF Antacids with antiflatulents Aluminium hydroxide+Magnesium A02AF80 1000790 ml hydroxide+Simeticone(O) DRUGS FOR PEPTIC ULCER AND GASTRO- A02B 34,7001 OESOPHAGEAL REFLUX DISEASE (GORD) A02BA H2-receptor antagonists 3,5364 A02BA02 Ranitidine(O) 494352,3 g 0,3 g 3,5106 A02BA02 Ranitidine(P) -

Lists of Medicinal Products for Rare Diseases in Europe*
March 2021 Lists of medicinal products for rare diseases in Europe* the www.orpha.net www.orphadata.org General Table of contents PART 1: List of orphan medicinal products in Europe with European orphan designation and European marketing authorization 3 Table of contents 3 Methodology 3 Classification by tradename 5 Annex 1: Orphan medicinal products withdrawn from the European Community Register of orphan medicinal products 22 Annex 2: Orphan medicinal products withdrawn from use in the European Union 31 Classification by date of MA in descending order 33 Classification by ATC category 34 Classification by MA holder 35 PART 2 : 37 List of medicinal products intended for rare diseases in Europe with European marketing authorization without an orphan designation in Europe 37 Table of contents 37 Methodology 37 Classification by tradename 38 Classification by date of MA in descending order 104 Classification by ATC category 106 Classification by MA holder 108 For any questions or comments, please contact us: [email protected] Orphanet Report Series - Lists of medicinal products for rare diseases in Europe. March 2021 http://www.orpha.net/orphacom/cahiers/docs/GB/list_of_orphan_drugs_in_europe.pdf 2 PART 1: List of orphan medicinal products in Europe with European orphan designation and European marketing authorization* Table of contents List of orphan medicinal products in Europe with European orphan designation and European marketing authorisation* 3 Methodology 3 Classification by tradename 5 Annex 1: Orphan medicinal products removed or withdrawn from the European Community Register of orphan medicinal products 22 Annex 2: Orphan medicinal products withdrawn from use in the European Union 31 Classification by date of MA in descending order 33 Classification by ATC category 34 Classification by MA holder 35 Methodology This part of the document provides the list of all orphan with the list of medicinal products that have been granted a medicinal products that have received a European Marketing marketing authorization (http://ec.europa. -

Tocophersolan Cite This Record
NIH U.S. National Library of Medicine National Center for Biotechnology Information O P E N CHEMISTRY Search PubChem D A T A B A S E Compound Summary for CID 71406 Tocophersolan Cite this Record STRUCTURE VENDORS DRUG INFO PHARMACOLOGY LITERATURE PATENTS BIOACTIVITIES PubChem CID: 71406 Chemical Names: Tocophersolan; TPGS; Vitamin E TPGS; Tocophersolan [USAN]; Tocofersolano; Tocofersolanum More... Molecular Formula: C35H58O6 Molecular Weight: 574.843 g/mol InChI Key: AOBORMOPSGHCAX-UHFFFAOYSA-N Drug Information: Clinical Trials Tocophersolan is a water-soluble amphipathic formulation of d-alpha-tocopherol succinate coupled, through a succinate linker, to polyethylene glycol (PEG) 1000. Due to its amphipathic property in which it forms its own micelles, tocophersolan is easily taken up into enterocytes, even in the absence of bile salts; fat soluble d-alpha-tocopherol is then released after hydrolysis. This formulation enhances the absorption of d- alpha-tocopherol compared to the administration of free d-alpha-tocopherol. In addition, tocophersolan may enhance the absorption of water-insoluble agents and other fat-soluble vitamins. Pharmacology from NCIt Vitamin E supplement, antioxidant Tocofersolan (INN) or tocophersolan is a synthetic water-soluble version of vitamin E. Natural forms of vitamin E are fat soluble, but not water-soluble. Tocofersolan is polyethylene glycol derivative of -tocopherol that enables water solubility Metabolite Description from Human Metabolome Database (HMDB) PUBCHEM COMPOUND TOCOPHERSOLAN Modify -
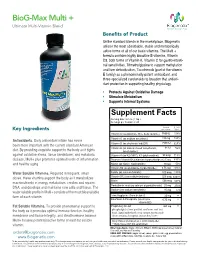
Biog-Max Multi +
BioG-Max Multi + Ultimate Multi-Vitamin Blend Benefits of Product Unlike standard blends in the marketplace, Biogenetix utilizes the most absorbable, stable and metabolically active forms of all of our basic vitamins. The Multi + formula contains highly bioactive B vitamins, Vitamin D3, both forms of Vitamin K, Vitamin C for gastro-intesti- nal sensitivities, Trimethylglycine to support methylation and liver detoxification, Tocotrienols (part of the vitamin E family) as a phenomenally potent antioxidant, and three specialized carotenoids to broaden that antioxi- dant protection in supporting healthy physiology. • Protects Against Oxidative Damage • Stimulate Metabolism • Supports Internal Systems Supplement Facts Serving Size: 5.0 mL (1 tsp.) Servings per Container: 20 Amount % Daily Key Ingredients per serving Value Vitamin A (as palmitate 86%, beta carotine) 7890 IU 158% 110 mg 183% Antioxidants. Daily antioxidant intake has never Vitamin C (as sodium ascorbate) 2500 IU been more important with the current standard American Vitamin D (as cholecalcified)(D3) 625% Vitamin E (as natural mixed tocopherols, 34 IU 56% diet. By providing exquisite support to the body as it fights tocofersolan) against oxidative stress, tissue breakdown, and metabolic Vitamin K (as K2 (MK7), K1 (phytonadine)) 90 mcg 113% disease, Multi+ plus promotes optimal levels of inflammation Thiamin (Vitamin B1)(thiamine hyrdochloride) 12.5 mg 833% and healthy aging Niacin (as niacin, niacinamide) 10 mg 50% Vitamin B6 (as pyridoxine hyrdochloride) 6.75 mg 375% 500 mcg Water Soluble Vitamins. Required in frequent, small Folate (as calcium folinate) 500 mcg 125% doses, these vitamins support the body as it metabolizes Vitamin B12 (as methylcobalamin) 500 mcg 8333% macronutrients in energy metabolism, creates and repairs Biotin 500 mcg 167% DNA, and develops and maintains new cells and tissue. -

Drug Tariff Part VIIIA August 2019.Pdf
08/2019 Part VIIIA BASIC PRICES OF DRUGS Drug Quantity Basic Price Category Part VIIIA - Basic Prices of Drugs Product List Part VIIIA products A Abacavir 600mg / Lamivudine 30 19000 C Lupin Healthcare 300mg tablets (UK) Ltd Abatacept 125mg/1ml solution for 4 120960 C Orencia ClickJect injection pre-filled disposable devices Abatacept 125mg/1ml solution for 4 120960 C Orencia injection pre-filled syringes Acacia spray dried powder 250 g 1632 C J M Loveridge Ltd Acamprosate 333mg gastro- 168 3377 L A resistant tablets Acarbose 100mg tablets 90 2515 L A Acarbose 50mg tablets 90 1436 L A Acebutolol 100mg capsules 84 1497 C Sectral Acebutolol 200mg capsules 56 1918 C Sectral Acebutolol 400mg tablets 28 1862 C Sectral Aceclofenac 100mg tablets 60 963 K A Acenocoumarol 1mg tablets 100 462 C Sinthrome Acetazolamide 250mg modified- 30 1666 C Diamox SR release capsules Acetazolamide 250mg tablets 112 1449 K M Acetic acid 2% ear spray S 5ml 410 C EarCalm Acetone liquid 50 ml 113 K A Acetylcysteine 200mg oral powder 30 11250 A sachets sugar free Acetylcysteine 2g/10ml solution for 10 2126 C Martindale infusion ampoules Pharmaceuticals Ltd Acetylcysteine 5% eye drops S 10 ml 1690 C Ilube Acetylcysteine 600mg capsules 30 3997 L A Acetylcysteine 600mg effervescent 30 550 C tablets sugar free Aciclovir 200mg dispersible tablets 25 149 K A Aciclovir 200mg tablets 25 120 K M Aciclovir 200mg/5ml oral 125 ml 3577 L A suspension sugar free Aciclovir 3% eye ointment S 4.5 g 934 C Zovirax Aciclovir 400mg dispersible tablets 56 1199 A Aciclovir 400mg tablets