Côte D'ivoire Country Operational Plan (COP/ROP)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cote D'ivoire Situation
SITUATIONAL EMERGENCY UPDATE Cote d’Ivoire Situation 12 November 2020 As of 11 November 2020, a total Nearly 92% of the new arrIvals who UNHCR has set up of 10,087 Ivorians have fled have fled Cote d’Ivoire are In LIberIa contingency plans in the Cote d’Ivoire, and the numbers where an airlIft of CRIs for 10,000 countrIes neIghbourIng Cote continue to rIse amid persIstent refugees is planned from DubaI. In the d’Ivoire and Is engaging wIth tensions despIte valIdation of the meantIme, locally purchased core- natIonal and local authorIties, electIon results by the relief items, food and cash-based sister UN agencies and other Constitutional Court. interventions are being delIvered. partners. POPULATION OF CONCERN Host Countries New arrivals LiberIa 9,255 Ghana 563 Guinea 249 Togo 20 Cote d’IvoIre (IDPs) 5,530 Total 15,617 * Data as of 11 November 2020 as reported by UNHCR Operations. New arrIvals at Bhai border, Grand Gedeh. CredIt @UNHCR www.unhcr.org 1 EMERGENCY UPDATE > Cote d’Ivoire Situation / November 2020 OperatIonal Context PolItIcal and securIty sItuatIon In Cote d’IvoIre Aftermath of the election ■ On 9 November, the ConstItutIonal CouncIl valIdated the electoral vIctory of PresIdent Alassane Ouattara as proclaimed by the Independent Electoral CommIssIon. The sItuatIon remaIns calm yet tense and the opposItIon, whIch announced the formatIon of a NatIonal TransItIonal CouncIl, has yet to recognIze the PresIdent’s vIctory. ■ FollowIng the valIdatIons of the electIon of PresIdent Ouattara, a Government spokesperson declared that a total of 85 people were kIlled, IncludIng 34 before the election, 20 on polling day, 31 after the election. -
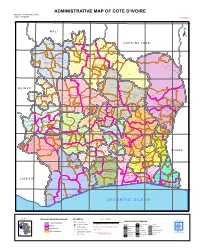
ADMINISTRATIVE MAP of COTE D'ivoire Map Nº: 01-000-June-2005 COTE D'ivoire 2Nd Edition
ADMINISTRATIVE MAP OF COTE D'IVOIRE Map Nº: 01-000-June-2005 COTE D'IVOIRE 2nd Edition 8°0'0"W 7°0'0"W 6°0'0"W 5°0'0"W 4°0'0"W 3°0'0"W 11°0'0"N 11°0'0"N M A L I Papara Débété ! !. Zanasso ! Diamankani ! TENGRELA [! ± San Koronani Kimbirila-Nord ! Toumoukoro Kanakono ! ! ! ! ! !. Ouelli Lomara Ouamélhoro Bolona ! ! Mahandiana-Sokourani Tienko ! ! B U R K I N A F A S O !. Kouban Bougou ! Blésségué ! Sokoro ! Niéllé Tahara Tiogo !. ! ! Katogo Mahalé ! ! ! Solognougo Ouara Diawala Tienny ! Tiorotiérié ! ! !. Kaouara Sananférédougou ! ! Sanhala Sandrégué Nambingué Goulia ! ! ! 10°0'0"N Tindara Minigan !. ! Kaloa !. ! M'Bengué N'dénou !. ! Ouangolodougou 10°0'0"N !. ! Tounvré Baya Fengolo ! ! Poungbé !. Kouto ! Samantiguila Kaniasso Monogo Nakélé ! ! Mamougoula ! !. !. ! Manadoun Kouroumba !.Gbon !.Kasséré Katiali ! ! ! !. Banankoro ! Landiougou Pitiengomon Doropo Dabadougou-Mafélé !. Kolia ! Tougbo Gogo ! Kimbirila Sud Nambonkaha ! ! ! ! Dembasso ! Tiasso DENGUELE REGION ! Samango ! SAVANES REGION ! ! Danoa Ngoloblasso Fononvogo ! Siansoba Taoura ! SODEFEL Varalé ! Nganon ! ! ! Madiani Niofouin Niofouin Gbéléban !. !. Village A Nyamoin !. Dabadougou Sinémentiali ! FERKESSEDOUGOU Téhini ! ! Koni ! Lafokpokaha !. Angai Tiémé ! ! [! Ouango-Fitini ! Lataha !. Village B ! !. Bodonon ! ! Seydougou ODIENNE BOUNDIALI Ponondougou Nangakaha ! ! Sokoro 1 Kokoun [! ! ! M'bengué-Bougou !. ! Séguétiélé ! Nangoukaha Balékaha /" Siempurgo ! ! Village C !. ! ! Koumbala Lingoho ! Bouko Koumbolokoro Nazinékaha Kounzié ! ! KORHOGO Nongotiénékaha Togoniéré ! Sirana -

Cote D'lvoire
Cote d’lvoire SIGNIFICANT ADVANCEMENT In 2014, Côte d’Ivoire made a significant advancement in efforts to eliminate the worst forms of child labor. The Government conducted a labor survey which included a subsurvey to determine the activities of working children; issued a decree to implement the Trafficking and Worst Forms of Child Labor Law that was adopted in 2010; and adopted a National Policy Document on Child Protection. The Government also established a National Committee for the Fight Against Trafficking in Persons; increased the budget of the Directorate for the Fight Against Child Labor by $800,000; continued to support social programs that address child labor in support of activities under the National Action Plan against Trafficking, Exploitation, and Child Labor (NAP); and completed the pilot phase of the child labor monitoring system known as SOSTECI. However, children in Côte d’Ivoire are engaged in the worst forms of child labor in domestic work and agriculture, particularly on cocoa farms, sometimes under conditions of forced labor. Gaps remain in enforcement efforts and in children’s access to education. I. PREVALENCE AND SECTORAL DISTRIBUTION OF CHILD LABOR Children in Côte d’Ivoire are engaged in the worst forms of child labor in domestic work and agriculture, particularly on cocoa farms, sometimes under conditions of forced labor.(1-9) According to a report by Tulane University that assessed data collected during the 2013–2014 harvest season, there were an estimated 1,203,473 child laborers ages 5 to 17 in the cocoa sector, of which 95.9 percent were engaged in hazardous work in cocoa production.(10) Table 1 provides key indicators on children’s work and education in Côte d’Ivoire. -

Côte D'ivoire
AFRICAN DEVELOPMENT FUND PROJECT COMPLETION REPORT HOSPITAL INFRASTRUCTURE REHABILITATION AND BASIC HEALTHCARE SUPPORT REPUBLIC OF COTE D’IVOIRE COUNTRY DEPARTMENT OCDW WEST REGION MARCH-APRIL 2000 SCCD : N.G. TABLE OF CONTENTS Page CURRENCY EQUIVALENTS, WEIGHTS AND MEASUREMENTS ACRONYMS AND ABBREVIATIONS, LIST OF ANNEXES, SUMMARY, CONCLUSION AND RECOMMENDATIONS BASIC DATA AND PROJECT MATRIX i to xii 1 INTRODUCTION 1 2 PROJECT OBJECTIVES AND DESIGN 1 2.1 Project Objectives 1 2.2 Project Description 2 2.3 Project Design 3 3. PROJECT IMPLEMENTATION 3 3.1 Entry into Force and Start-up 3 3.2 Modifications 3 3.3 Implementation Schedule 5 3.4 Quarterly Reports and Accounts Audit 5 3.5 Procurement of Goods and Services 5 3.6 Costs, Sources of Finance and Disbursements 6 4 PROJECT PERFORMANCE AND RESULTS 7 4.1 Operational Performance 7 4.2 Institutional Performance 9 4.3 Performance of Consultants, Contractors and Suppliers 10 5 SOCIAL AND ENVIRONMENTAL IMPACT 11 5.1 Social Impact 11 5.2 Environmental Impact 12 6. SUSTAINABILITY 12 6.1 Infrastructure 12 6.2 Equipment Maintenance 12 6.3 Cost Recovery 12 6.4 Health Staff 12 7. BANK’S AND BORROWER’S PERFORMANCE 13 7.1 Bank’s Performance 13 7.2 Borrower’s Performance 13 8. OVERALL PERFORMANCE AND RATING 13 9. CONCLUSIONS, LESSONS AND RECOMMENDATIONS 13 9.1 Conclusions 13 9.2 Lessons 14 9.3 Recommendations 14 Mrs. B. BA (Public Health Expert) and a Consulting Architect prepared this report following their project completion mission in the Republic of Cote d’Ivoire on March-April 2000. -

Évaluation Du Portefeuille De Projets Du Fonds De Consolidation De La Paix En Côte D'ivoire (2015-2019) Rapport Final
Évaluation du portefeuille de projets du Fonds de Consolidation de la Paix en Côte d’Ivoire (2015-2019) Rapport final 30 décembre 2019 Équipe d’évaluation : • Fernanda Faria (cheffe d’équipe) • Belén Díaz (spécialiste genre et consolidation de la paix) • Guy Oscar Toupko (consultant local) TABLE DES MATIÈRES Acronymes ................................................................................................................................. 4 Sommaire exécutif .................................................................................................................... 6 1 Introduction ...................................................................................................................... 1 2 Objectifs et portée de l’évaluation .................................................................................. 1 3 Méthodologie de l’évaluation .......................................................................................... 4 4 Contexte ............................................................................................................................. 9 4.1 Contexte politique ...................................................................................................... 9 4.2 Contexte socio-économique ..................................................................................... 10 4.3 Genre ........................................................................................................................ 11 4.4 Situation sécuritaire et réconciliation nationale ...................................................... -

Template May 29
12° er ig N 8° 7° 6° 5° 4° 3° The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance CÔTE D’IVOIRE by the United Nations. CÔTE BURKINABURKINA National capital D’IVOIRE Sikasso Provincial capital Bobo-Dioulasso e Leo BASOBASO r Town Diebougou i 11° o Major airport N Orodara a B t a International boundary l MALI g o o L e Regional boundary V e r Banfora a b Main road a Tingrela Track Gaoua San Sokoro Goueya Railroad kar ani Katoro Kaoura 10° Zinguinasso 10° Maniniam Korohara Ouangolodougou Samatiguila Bandam B SAVANES a l B Bobanie a DENGUELE l c a Moromoro k Madinani n Gbeleba c V o T Ferkessedougou l t i a e Korhogo I n Seguelo r Odienne b Boundiali i a n g o Bouna u GUINEA Bako Fasselemon Kiemou Tafire 9° Paatogo 9° B Gawi Siraodi Kineta ou Fadyadougou Lato M Kakpin a Koro r VALLE DU BANDAMA a a Sonozo Bandoli a/Bo Kani h Bo o u Kafine ZANZAN e Boudouyo Santa Touba WORODOUGOU Dabakala Tanbi BAFING Katiola Nandala Mankono Diaradougou Bondoukau 8° Foungesso 8° C Seguela a Toumbo v Glanle Tanda a Biankouma l l Bouake y Beoumi MONTAGNES Man Zuenoula Sakassou M'Bahiacro Koun Vavoua Ba Sunyani N ’ Z I C O M O E Danane HAUT Agnibilekrou Daoukro SASSANDRA Bouafle 7° Bangolo LACS MOYEN 7° COMOE Binhouye Daloa MARAHQUE Yamoussoukro Dimbokro Bougouanou Abengourou Duekoue Guiglo Sinfra Toumodi Toulepleu Issia MOYEN CAVALLY Oume Bebou GHANA FROMAGER a i o Zagne Gribouo Gagnoa AGNEBY B n Tchien a Adzope T Agboville 6° Tiassale 6° Tai Lakota Soubre Divo SUD Gueyo SUD BANDAMA COMOE B LIBERIA o u LAGUNES b Aboisso Niebe o Abidjan Fish Town BAS SASSANDRA Attoutou Braffedon Grand-Bassam 5° Gazeko 5° Grabo N o n Sassandra o GU L F O F GUINEA Barclayville Olodio Olodio San-Pedro 0 30 60 90 km Grand Béréby Tabou A T L A N T I C OC E A N 0 30 60 mi Harper 8° 7° 6° 5° 4° 3° Map No. -

2018 CLCCG Annual Report
CLCCG ANNUAL REPORT U.S. Representative Eliot Engel U.S. Department of Labor Government of Côte d’Ivoire Government of Ghana International Chocolate and Cocoa Industry The United States Department of Labor is responsible only for the content it provided for this report. The material provided by other signatories to the Declaration of Joint Action to Support Implementation of the Harkin-Engel Protocol does not necessarily reflect the views or policies of the United States Department of Labor, nor does mention of trade names, commercial products, or organizations imply endorsement by the United States Government. Photo Credit: World Cocoa Foundation ACRONYMS………………………………………………………………………………………………………………………………………….....ii CONGRESSIONAL QUOTE………………………………………………………………………………………………………………………...1 INTRODUCTION……………………………………………………………………………………………………………………………………….2 REPORT FOR THE GOVERNMENT OF CÔTE D’IVOIRE (FRENCH)….…………………………………………..………………..9 REPORT FOR THE GOVERNMENT OF GHANA…………………………………………………………………………………….…..17 REPORT FOR THE U.S. DEPARTMENT OF LABOR………………………………………………………………...……….………...34 REPORT FROM WORLD COCOA FOUNDATION ON COCOAACTION…………………………………………………………39 APPENDIX 1: DECLARATION………………………………………………………………………………….………………………..……..49 APPENDIX 2: FRAMEWORK…………………………………………………………………………………………………………………….50 APPENDIX 3: BY-LAWS……………………………………………………………………………………………………………….…………..57 i ACRONYMS ACE Action against Child Exploitation ANADER National Agency for Rural Development Support/l’Agence Nationale d’Appui au Développement Rural AHTU Anti-Trafficking Unit of -

Côte D'ivoire
Niger 8° 7° 6° 5° 4° 3° CÔTE D’IVOIRE The boundaries and names shown and CÔTE the designations used on this map do Sikasso BURKINA National capital D’IVOIRE not imply official endorsement or Regional capital acceptance by the United Nations Bobo-Dioulasso e FASO r Town i 11° Diebougou o 11° Orodara Major airport N B a t a International boundary l MALI g o o L e V e Regional boundary r Banfora a b Main road a Tingrela Railroad Gaoua Goueya San Sokoro kar ani Katoro Kaoura 10° Maniniam Zinguinasso Ouangolodougou 10° Korohara Samatiguila Banda B ma l SAVANES B Bobanie a DENGUELE l c a Moromoro k n Madinani c V Gbeleba o Odienne l Boundiali Ferkessedougou t a I T Seguelo Korhogo r i i e n n g b a Fasselemon o Bouna u GUINEA Bako Paatogo Kiemou Tafire 9° 9° B Gawi Siraodi ou Kineta Fadyadougou Lato M Kakpin a Bandoli Koro r Sonozo a a Kafine oa/Bo Kani h VALLEE DU B o ZANZAN u e Dabakala Boudouyo Santa Touba WORODOUGOU BANDAMA Tanbi BAFING Nandala Mankono Katiola Diaradougou Bondoukau 8° Foungesso 8° C Seguela a v Tanda a Glanle Biankouma Toumbo l l y Beoumi Bouake DIX-HUIT MONTAGNES Zuenoula Sakassou M'Bahiacro Koun Man Vavoua Ba Sunyani Danane N’ZI COMOE HAUT Agnibilekrou Bangolo Daoukro 7° SASSANDRA Bouafle LACS MOYEN 7° COMOE Binhouye Daloa MARAHOUE Yamoussoukro Duekoue Abengourou Dimbokro Sinfra Guiglo Bougouanou Toulepleu Issia Toumodi GHANA Oume MOYENCAVALLY Bebou FROMAGER a i o Zagne Gribouo Gagnoa AGNEBY B n a Tchien Adzope T 6° 6° Agboville Tai Lakota Divo Tiassale Soubre SUD Gueyo SUD BANDAMA COMOE B LIBERIA o u LAGUNES b Aboisso Niebe o Abidjan Grand-Lahou Fish Town BAS SASSANDRA Attoutou Grand-Bassam Braffedon 5° Gazeko 5° Grabo N o n Sassandra o GULF O F GUINEA Barclayville Olodio San-Pedro 0 30 60 90 km Grand Béréby Harper 0 30 60 mi Tabou ATLANTIC OCE A N 8° 7° 6° 5° 4° 3° Map No. -

Scaling up Programs to Reduce Human Rights- Related Barriers to HIV and TB Services
Baseline Assessment – Côte d'Ivoire Scaling up Programs to Reduce Human Rights- Related Barriers to HIV and TB Services 2018 Geneva, Switzerland DISCLAIMER Towards the operationalisation of Strategic Objective 3(a) of the Global Fund Strategy, Investing to End Epidemics, 2017-2022, this paper was commissioned by the Global Fund to Fight AIDS, TB and Malaria and presents, as a working document for reflection and discussion with country stakeholders and technical partners, findings of research rel- evant to reducing human rights-related barriers to HIV and TB services and implement- ing a comprehensive programmatic response to such barriers in Cote d’Ivoire. The views expressed in the paper do not necessarily reflect the views of the Global Fund. ACKNOWLEDGEMENTS With regard to the research and writing of this report, the Global Fund would like to acknowledge the work of the work of APMG Health (authors: Nadia Peerun, Kina Diop, Dave Burrows and Lou McCallum; and in-country team – Hervé Agbo, Stanislas Houndji, M'boukebiè M'Bouke, Julien Kassi, Dieudonné Kouadio, Albertine Kouakou, Claudine Gauly and Abou Dramane Traore), as well as country and technical partners and the many others who have inputted into the report. 1 ACRONYM LIST AFJCI Association des femmes juristes de la Côte d'Ivoire [Association of Women La- wyers of Côte d'Ivoire] ART Antiretroviral therapy ARV Antiretroviral ASC Community health agents BCC Behaviour change communication CAB Community advisory boards CAT Centre antituberculeux [Anti-tuberculosis centres] CBO Community -

Cote D'ivoire
1 Cote d’Ivoire Media and telecoms landscape guide August 2011 2 Index Page Introduction..................................................................................................... 3 Media overview................................................................................................ 8 Radio overview................................................................................................17 Radio stations..................................................................................................21 TV overview......................................................................................................52 TV stations.......................................................................................................54 Print media.......................................................................................................58 Main newspapers............................................................................................60 Internet news sites.........................................................................................66 Media resources..............................................................................................67 Traditional channels of communication.......................................................76 Telecoms overview.........................................................................................79 Telecoms companies......................................................................................82 Principal sources............................................................................................87 -

Côte D'ivoire
Côte d’Ivoire Risk-sensitive Budget Review UN Office for Disaster Risk Reduction UNDRR Country Reports on Public Investment Planning for Disaster Risk Reduction This series is designed to make available to a wider readership selected studies on public investment planning for disaster risk reduction (DRR) in cooperation with Member States. United Nations Office for Disaster Risk Reduction (UNDRR) Country Reports do not represent the official views of UNDRR or of its member countries. The opinions expressed and arguments employed are those of the author(s). Country Reports describe preliminary results or research in progress by the author(s) and are published to stimulate discussion on a broad range of issues on DRR. Funded by the European Union Front cover photo credit: Anouk Delafortrie, EC/ECHO. ECHO’s aid supports the improvement of food security and social cohesion in areas affected by the conflict. Page i Table of contents List of figures ....................................................................................................................................ii List of tables .....................................................................................................................................iii List of acronyms ...............................................................................................................................iv Acknowledgements ...........................................................................................................................v Executive summary ......................................................................................................................... -

Populated Printable COP 2009 Cote D'ivoire Generated 9/28/2009 12:01:26 AM
Populated Printable COP 2009 Cote d'Ivoire Generated 9/28/2009 12:01:26 AM ***pages: 518*** Cote d'Ivoire Page 1 Table 1: Overview Executive Summary File Name Content Type Date Uploaded Description Uploaded By COP09 Exec Summary- application/msword 11/14/2008 CI Executive Summary OTossou bh-bbs-bh-13nov08.doc Country Program Strategic Overview Will you be submitting changes to your country's 5-Year Strategy this year? If so, please briefly describe the changes you will be submitting. Yes X No Description: Ambassador Letter File Name Content Type Date Uploaded Description Uploaded By Ambassador letter-CI- application/pdf 11/14/2008 CI Ambassador Letter OTossou 14nov08.pdf Country Contacts Contact Type First Name Last Name Title Email PEPFAR Coordinator Brian Howard COP Manager (not Country [email protected] Coordinator) PEPFAR Coordinator James Allman Interim Coordinator [email protected] DOD In-Country Contact Patrick Doyle Defense Attaché [email protected] HHS/CDC In-Country Contact Bruce Struminger CDC Chief of Party [email protected] USAID In-Country Contact Toussaint Sibailly USAID Focal Point [email protected] U.S. Embassy In-Country Cynthia Akuetteh DCM [email protected] Contact Global Fund What is the planned funding for Global Fund Technical Assistance in FY 2009? $350000 Does the USG assist GFATM proposal writing? Yes Does the USG participate on the CCM? Yes Generated 9/28/2009 12:01:26 AM ***pages: 518*** Cote d'Ivoire Page 2 Table 2: Prevention, Care, and Treatment Targets 2.1 Targets for Reporting Period Ending