Approach to Neonatal Hypotonia (Floppy Baby).” These Podcasts Are Designed to Give Medical Students an Overview of Key Topics in Pediatrics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Focusing on the Re-Emergence of Primitive Reflexes Following Acquired Brain Injuries
33 Focusing on The Re-Emergence of Primitive Reflexes Following Acquired Brain Injuries Resiliency Through Reconnections - Reflex Integration Following Brain Injury Alex Andrich, OD, FCOVD Scottsdale, Arizona Patti Andrich, MA, OTR/L, COVT, CINPP September 19, 2019 Alex Andrich, OD, FCOVD Patti Andrich, MA, OTR/L, COVT, CINPP © 2019 Sensory Focus No Pictures or Videos of Patients The contents of this presentation are the property of Sensory Focus / The VISION Development Team and may not be reproduced or shared in any format without express written permission. Disclosure: BINOVI The patients shown today have given us permission to use their pictures and videos for educational purposes only. They would not want their images/videos distributed or shared. We are not receiving any financial compensation for mentioning any other device, equipment, or services that are mentioned during this presentation. Objectives – Advanced Course Objectives Detail what primitive reflexes (PR) are Learn how to effectively screen for the presence of PRs Why they re-emerge following a brain injury Learn how to reintegrate these reflexes to improve patient How they affect sensory-motor integration outcomes How integration techniques can be used in the treatment Current research regarding PR integration and brain of brain injuries injuries will be highlighted Cases will be presented Pioneers to Present Day Leaders Getting Back to Life After Brain Injury (BI) Descartes (1596-1650) What is Vision? Neuro-Optometric Testing Vision writes spatial equations -

Retained Neonatal Reflexes | the Chiropractic Office of Dr
Retained Neonatal Reflexes | The Chiropractic Office of Dr. Bob Apol 12/24/16, 1:56 PM Temper tantrums Hypersensitive to touch, sound, change in visual field Moro Reflex The Moro Reflex is present at 9-12 weeks after conception and is normally fully developed at birth. It is the baby’s “danger signal”. The baby is ill-equipped to determine whether a signal is threatening or not, and will undergo instantaneous arousal. This may be due to sudden unexpected occurrences such as change in head position, noise, sudden movement or change of light or even pain or temperature change. This activates the stress response system of “fight or flight”. If the Moro Reflex is present after 6 months of age, the following signs may be present: Reaction to foods Poor regulation of blood sugar Fatigues easily, if adrenalin stores have been depleted Anxiety Mood swings, tense muscles and tone, inability to accept criticism Hyperactivity Low self-esteem and insecurity Juvenile Suck Reflex This is active together with the “Rooting Reflex” which allows the baby to feed and suck. If this reflex is not sufficiently integrated, the baby will continue to thrust their tongue forward, pushing on the upper jaw and causing an overbite. This by nature affects the jaw and bite position. This may affect: Chewing Difficulties with solid foods Dribbling Rooting Reflex Light touch around the mouth and cheek causes the baby’s head to turn to the stimulation, the mouth to open and tongue extended in preparation for feeding. It is present from birth usually to 4 months. -

Hypotonia and Lethargy in a Two-Day-Old Male Infant Adrienne H
Hypotonia and Lethargy in a Two-Day-Old Male Infant Adrienne H. Long, MD, PhD,a,b Jennifer G. Fiore, MD,a,b Riaz Gillani, MD,a,b Laurie M. Douglass, MD,c Alan M. Fujii, MD,d Jodi D. Hoffman, MDe A 2-day old term male infant was found to be hypotonic and minimally abstract reactive during routine nursing care in the newborn nursery. At 40 hours of life, he was hypoglycemic and had intermittent desaturations to 70%. His mother had an unremarkable pregnancy and spontaneous vaginal delivery. The mother’s prenatal serology results were negative for infectious risk factors. Apgar scores were 9 at 1 and 5 minutes of life. On day 1 of life, he fed, stooled, and voided well. Our expert panel discusses the differential diagnosis of hypotonia in a neonate, offers diagnostic and management recommendations, and discusses the final diagnosis. DRS LONG, FIORE, AND GILLANI, birth weight was 3.4 kg (56th PEDIATRIC RESIDENTS percentile), length was 52 cm (87th aDepartment of Medicine, Boston Children’s Hospital, d e percentile), and head circumference Boston, Massachusetts; and Neonatology Section, Medical A 2-day old male infant born at Genetics Section, cDivision of Child Neurology, and 38 weeks and 4 days was found to be was 33 cm (12th percentile). His bDepartment of Pediatrics, Boston Medical Center, Boston, limp and minimally reactive during physical examination at birth was Massachusetts routine care in the newborn nursery. normal for gestational age, with Drs Long, Fiore, and Gillani conceptualized, drafted, Just 5 hours before, he had an appropriate neurologic, cardiac, and and edited the manuscript; Drs Douglass, Fujii, and appropriate neurologic status when respiratory components. -

Hypotonia Surestep Product Catalog Page 29 in Step with Pediatric Hypotonia
SPECIAL EDUCATIONAL SERIES DIAGNOSTIC INSIGHTS ANALYZING GAIT CHANGES GROSS MOTOR SKILLS ORTHOTIC MANAGEMENT CLI N I CAL CASE STUDIES Sponsored by an educational grant from: In Step With Pediatric Hypotonia SureStep Product Catalog Page 29 In Step With Pediatric Hypotonia Contents VIEWPOINT FROM THE EDITOR: An Unexpected Path, Mobility and More an Invaluable Perspective At the most basic level, mobility is about get- PAGE 3 ting from point A to point B. But, for many children with hypotonia, it’s about so much 4 more. FEATURES It’s about independence. It’s about con- fidence. It’s about maintaining strength, fit- ness, and healthy bones. It’s about not being Understanding Hypotonia excluded from activities enjoyed by their PAGE 4 typically developing peers. And improved mobility may have even Gait: The Cornerstone more benefits in those children whose hy- potonia is associated with social and behav- of Intervention ioral developmental delays. New research PAGE 8 has identified an association between motor skills and sociobehavioral milestones in chil- 8 The Importance of Gross dren with autism spectrum disorder, who often present with hypotonia (see “The Im- Motor Skills portance of Gross Motor Skills,” page 12). PAGE 12 This suggests that early intervention to improve gross motor skills—including or- thotic devices and physical therapy—may Orthotic Solutions for also help certain children interact more Children with Hypotonia comfortably with others. That won’t come as PAGE 16 a surprise to the clinicians and parents who 12 have personally seen it happen. This special issue is filled with evidence- Orthotic Success Stories: based information and personal success sto- Four Cases in a Series ries illustrating how effective interventions can enhance mobility in children with hy- PAGE 20 potonia. -

Newborn Reflexes
O C T O B E R 2 0 1 9 NEWBORN REFLEXES MORO Reflex: also known as the embracing or startle reflex. Moro reflex is mediated by the brain stem and becomes apparent at approximately 25 to 26 weeks' gestational age. It is an involuntary motor response meant to protect the infant from sudden changes in body displacements.In normal infants, the response is symmetrical and disappears by 3 to 4 months. The Moro reflex consists predominantly of abduction and extension of the arms with hands open, and the thumb and index finger semiflexed to form a “C”. Leg movements may occur, but they are not as uniform as the arm movements. With return of the arms toward the body, the infant either relaxes or cries. Absence of the reflex may indicate: intracranial lesions asymmetrical response may indicate birth injury involving the brachial plexus, clavicle, or humerus abnormal persistence of embrace gesture may indicate hypertonicity persistence of entire Moro reflex after 4 months may indicate delay in neurologic maturation. ROOTING Reflex: Indicates normal maturity and intact trigeminal nerve. When cheek is stroked, infant turns toward stroking and opens the lips to suck (if not fed recently). This reflex helps the newborn baby find food; when the mother hold the child and allows her breast to brush the newborns cheek, the reflex makes the baby turn toward the breast. The rooting reflex disappears around the sixth week of life. SUCKING Reflex: Indicates normal maturity and intact hypoglossal nerve. Offer non-latex gloved finger or nipple to test; Newborns suck even when sleeping (non-nutritive sucking) and it can have a quieting effect on the baby; This reflex doesn't start until about the 32nd week of pregnancy and is not fully developed until about 36 weeks. -

Practice Resource: CARE of the NEWBORN EXPOSED to SUBSTANCES DURING PREGNANCY
Care of the Newborn Exposed to Substances During Pregnancy Practice Resource for Health Care Providers November 2020 Practice Resource: CARE OF THE NEWBORN EXPOSED TO SUBSTANCES DURING PREGNANCY © 2020 Perinatal Services BC Suggested Citation: Perinatal Services BC. (November 2020). Care of the Newborn Exposed to Substances During Pregnancy: Instructional Manual. Vancouver, BC. All rights reserved. No part of this publication may be reproduced for commercial purposes without prior written permission from Perinatal Services BC. Requests for permission should be directed to: Perinatal Services BC Suite 260 1770 West 7th Avenue Vancouver, BC V6J 4Y6 T: 604-877-2121 F: 604-872-1987 [email protected] www.perinatalservicesbc.ca This manual was designed in partnership by UBC Faculty of Medicine’s Division of Continuing Professional Development (UBC CPD), Perinatal Services BC (PSBC), BC Women’s Hospital & Health Centre (BCW) and Fraser Health. Content in this manual was derived from module 3: Care of the newborn exposed to substances during pregnancy in the online module series, Perinatal Substance Use, available from https://ubccpd.ca/course/perinatal-substance-use Perinatal Services BC Care of the Newborn Exposed to Substances During Pregnancy ii Limitations of Scope Iatrogenic opioid withdrawal: Infants recovering from serious illness who received opioids and sedatives in the hospital may experience symptoms of withdrawal once the drug is discontinued or tapered too quickly. While these infants may benefit from the management strategies discussed in this module, the ESC Care Tool is intended for newborns with prenatal substance exposure. Language A note about gender and sexual orientation terminology: In this module, the terms pregnant women and pregnant individual are used. -

Electromyography and Nerve Conduction Studies in Patients With
ogy & N ol eu ur e ro N p h f y o s l Ziegler MS, J Neurol Neurophysiol 2014, 5:3 i o a l n o r g u y o DOI: 10.4172/2155-9562.1000203 J Journal of Neurology & Neurophysiology ISSN: 2155-9562 Research Article Open Access Electromyography and Nerve Conduction Studies in Patients with Lumbar Spinal Stenosis: Is Neurophysiological Examination an Important Tool? Marcus Sofia Ziegler1, Renata Siciliani Scalco2, Erasmo de Abreu Zardo1, Jefferson Becker2 and Irenio Gomes2* 1Department of Orthopaedics & Spine Surgery, Hospital São Lucas Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, Brazil 2Department of Neurology, Hospital São Lucas Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, Brazil *Corresponding author: Irenio Gomes, Hospital Sao Lucas, and Avenida Ipiranga 6690 - 3 ºandar - IGG Porto Alegre - RS – Brasil, CEP 90610-000, Tel: +55 (51) 3336.8153 / 3320.3000; E-mail: [email protected] Received Date: Jan 21, 2014 Accepted Date: Apr 25, 2014 Published Date: Apr 30, 2014 Copyright: © 2014 Ziegler MS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Background: There is no single test that defines properly lumbar spinal stenosis (LSS) diagnosis, and diagnosis of the syndrome continues to rely on clinical judgment. LSS symptoms may be broad and may be seen in multiple disorders in elderly. Hypothesis: To identify the role of electromyography and nerve-conduction studies on LSS diagnosis. -
IUGR: Intrauterine Growth Restriction
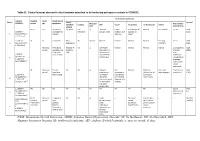
Table S1. Clinical features observed in the 6 patients described so far harboring pathogenic variants in FOXRED1. Evolutionary symptoms Variants Prenatal Onset Onset clinical Patient Lactic/ Survival FOXRED1 period age symptoms Muscular Psychomotor Metabolic Epilepsy MRI Visual Respiratory Cardiovascular Others tone development acidosis IUGR 2m Hypotonia Yes (+++) Yes ↓ Normal Latent Bronchospasm Normal AEP normal IQ: 48 Alive c.920G>A Development refractary (2m,4y,7y3m) strabismus of episodes in (15y) 1 (p.Gly307Glu) / al delay right eye infant c.733+1G>A c.920G>A NI 4y Clumsiness With No Normal Normal Normal Normal Normal Learning IQ: 99 Alive 2 (p.Gly307Glu) / exercise (+) disorders (19y) c.733+1G>A - Neonatal Premature; No (only ↑ Yes ↓ Decreased Normal Normal Normal Normal Gradually loss Alive period Hypoglycemia lactate in attenuation in of motor (22y)) Congenital LCR) the putamen skills; c.694C>T lactic acidosis and cerebellar wheelchair; (p.Gln232X) / 3 atrophy (6y) no expressive c.1289A>G language; 18 (p.Asn430Ser) understands simple commands NI Neonatal Truncal Yes Yes ↓ Delayed Eye Normal Mild non- Persistent Psychomotor Alive period hypotonia myelination movements obstructive left hepatomegaly retardation (10y) c.1054 C>T Poor feeding ventricular have always ventricular (p.Arg352Trp) / dilatation; been roving hypertrophy 4 c.1054 C>T abnormal signal bilateral optic (p.Arg352Trp) 19 in the thalami atrophy and basal ganglia (8m) c.1308G>A ND ND ND ND Yes NA NA NA NA NA NA Severe Alive (p.Val421Met) / psychomotor (¿) 5 c.1308G>A retardation (p.Val421Met)20 IUGR; Neonatal Congenital Yes Yes ↓ Large -- Persistent Dilated right - - Death (3 c.612_615dupA Cerebral period lactic periventricular severe ventricle and months) CTG intraventric acidosis. -

Cerebral Hypotonia by Mihee Bay MD (Dr
Cerebral hypotonia By Mihee Bay MD (Dr. Bay of Kennedy Krieger Institute and Johns Hopkins School of Medicine has no relevant financial relationships to disclose.) Originally released July 12, 2006; last updated February 1, 2016; expires February 1, 2019 Introduction This article includes discussion of cerebral hypotonia, central hypotonia, essential hypotonia, benign congenital hypotonia, and floppy infant. The foregoing terms may include synonyms, similar disorders, variations in usage, and abbreviations. Overview Hypotonia is a clinical manifestation of numerous diseases affecting the central and/or peripheral motor nervous system. The key to accurate diagnosis involves integral steps of evaluation that include a detailed history, examination, and diagnostic tests. “Cerebral” (or central) hypotonia implies pathogenesis from abnormalities from the central nervous system, and related causal disorders include cerebral dysgenesis and genetic or metabolic disorders. Patients with central hypotonia generally have hypotonia without associated weakness, in contrast to the peripheral (lower motor neuron) causes, which typically produce both hypotonia and muscle weakness. Hypotonia is a clinical manifestation of over 500 genetic disorders; thus, a logical, stepwise approach to diagnosis is essential. With recent advances in the field of genetic testing, diagnostic yield will undoubtedly improve. There is no cure, but treatment includes supportive therapies, such as physical and occupational therapy, and diagnosis-specific management. Key points • Hypotonia is reduced tension or resistance of passive range of motion. • The first step in the evaluation of a child with hypotonia is localization to the central (“cerebral”) or peripheral nervous system, or both. • Central hypotonia is more likely to be noted axially with normal strength and hyperactive to normal deep tendon reflexes. -

Mean Platelet Volume in Asymptomatic Chorioamnionitis-Exposed Infants
www.jpnim.com Open Access eISSN: 2281-0692 Journal of Pediatric and Neonatal Individualized Medicine 2021;10(1):e100132 doi: 10.7363/100132 Received: 2019 Aug 22; revised: 2020 Jan 26; accepted: 2020 Feb 02; published online: 2020 Dec 28 Original article Mean platelet volume in asymptomatic chorioamnionitis- exposed infants. A retrospective case-control study Atef Alshafei, Moustafa Hassan, Yaser El saba, Anwar Khan, Mahmoud Ahmed Neonatology Section, Pediatric Department, Dubai Hospital, Dubai, UAE Abstract Introduction: Maternal chorioamnionitis (CA) is a serious condition causing several neonatal morbidities and long-term neurodevelopmental sequelae in exposed infants. Current guidelines still recommend admission, laboratory evaluation, and antibiotic administration to all CA-exposed infants. The incidence of early-onset neonatal sepsis (EOS) is currently low, owing to the routine intrapartum antibiotic administration to mothers identified to be at risk of developing CA. New diagnostic tools for early diagnosis of sepsis in apparently healthy infants exposed to maternal CA are needed. Previous studies showed that mean platelet volume (MPV) is evolving as a potential inflammatory marker of neonatal sepsis. We aimed to study whether MPV can be used as an adjuvant diagnostic tool for EOS in asymptomatic CA-exposed infants. Objective: To evaluate the role of MPV as an adjuvant biomarker of EOS in cases of asymptomatic CA-exposed infants. Design: Retrospective case-control study. Setting: A tertiary care Neonatal Intensive Care Unit (NICU). Patients: Asymptomatic CA-exposed infants 37-40 weeks of gestation admitted between May 2016 and April 2019 to the NICU of Dubai Hospital, UAE. Results: A total of 1,300 infants were admitted to NICU during the study period. -

Long-Term Outcome After Neonatal Meconium Obstruction
Long-term Outcome After Neonatal Meconium Obstruction Julie R. Fuchs, MD, and Jacob C. Langer, MD ABSTRACT. Objective. It is unclear whether children meconium ileus and those undergoing resection or enter- with cystic fibrosis (CF) who present with neonatal ostomy. Patients with meconium obstruction who do not meconium ileus have a different long-term outcome from have CF have an excellent long-term prognosis. This those presenting later in childhood with pulmonary com- information will be useful in counseling the families of plications or failure to thrive. We examined a cohort of infants presenting with neonatal meconium obstruction. patients with meconium ileus, and compared their long- Pediatrics 1998;101(4). URL: http://www.pediatrics.org/ term outcome with children who had CF without meco- cgi/content/full/101/4/e7; cystic fibrosis, meconium ileus, nium ileus and neonates who had meconium obstruction meconium plug syndrome. without CF (meconium plug syndrome). Study Design. Comparative study using retrospective and follow-up interview data. ABBREVIATION. CF, cystic fibrosis. Patients. Group 1 consisted of 35 surviving CF pa- tients who presented with meconium ileus between 1966 econium obstruction in the neonate is a and 1992. Two control groups were also studied: 35 age- spectrum of disease that includes meco- and sex-matched CF patients without meconium ileus 1 (group 2), and 12 infants presenting with meconium plug Mnium ileus and meconium plug syndrome. syndrome during the same time period (group 3). Meconium ileus is characterized by extremely viscid, Outcome Measures. Pulmonary, gastrointestinal, nu- protein-rich inspissated meconium causing terminal tritional, and functional status were reviewed, and sur- ileal obstruction, and accounts for approximately gical complications were recorded. -
Common Anomalies Associated To
ISSN: 2643-3885 Muhsin. Int J Foot Ankle 2018, 2:013 Volume 2 | Issue 2 Open Access International Journal of Foot and Ankle RESEARCH ARTICLE Common Anomalies Associated To Congenital Vertical Talus: A Single Center Experience Elmas Muhsin* Check for Department of Medical Genetic, Afyon Kocatepe University, Turkey updates *Corresponding author: Elmas Muhsin, Department of Medical Genetic, Afyon Kocatepe University, Afyonkarahisar, Turkey vicular. The incidence is estimated to be one in 10,000. Abstract Approximately half of all cases (idiopathic) are associ- Background: Congenital vertical talus is defined as a foot deformity in which the calcaneus is in equinus, the talus is ated with deformity and 2-5 neuromuscular and genet- plantarflexed, and there is a rigid and irreducible dislocation ic disorders in the remaining cases. There is evidence of the talonavicular joint complex, with the navicular articu- that some isolated deformities are transmitted as an lating on the dorsolateral aspect of the talar neck. It is often autosomal dominant feature with incomplete pene- associated with systemic involvement. trance [1-4]. The deformity is also known by congenital Aims: To identify the most common anomalies accompany- “rocker-bottom” flatfoot because of its rigid deformity ing to CVT (Congenital Vertical Talus). No literature investi- gating similar clinical data was found in the literature review. with the forefoot dorsiflexed and the hindfoot plantar- Study design: CVT has a systemic effect and is accom- flexed. The term “congenital convex pes valgus” is also panied by many anomalies. At the same time as this study, frequently used. To make a definite diagnosis, it is im- anomalies were frequently found accompanying CVT.