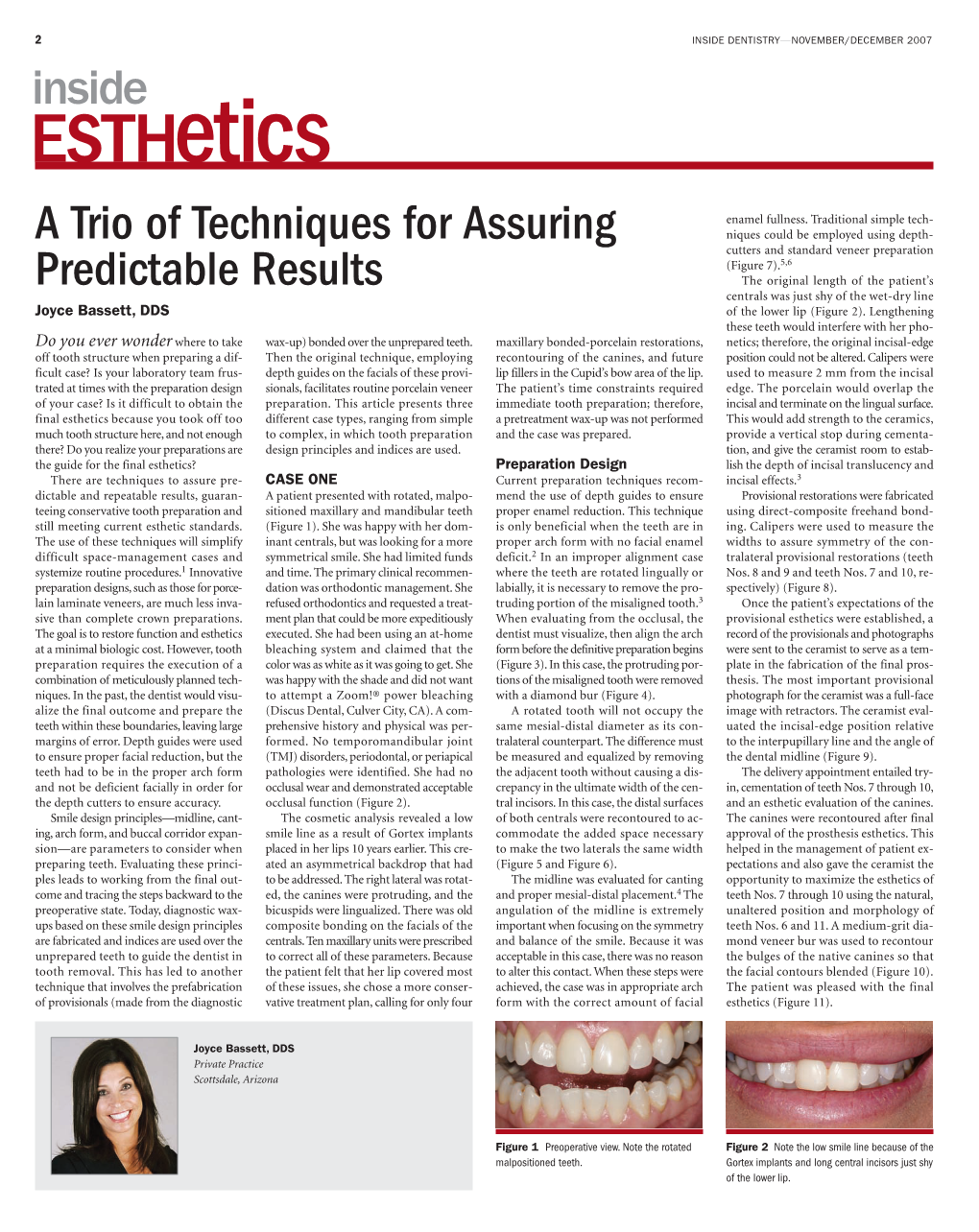
INSIDE DENTISTRY—NOVEMBER/DECEMBER 2007 Inside Esthetics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

UNDERSTANDING PORTRAYALS of LAW ENFORCEMENT OFFICERS in HIP-HOP LYRICS SINCE 2009 By
ON THE BEAT: UNDERSTANDING PORTRAYALS OF LAW ENFORCEMENT OFFICERS IN HIP-HOP LYRICS SINCE 2009 by Francesca A. Keesee A Thesis Submitted to the Graduate Faculty of George Mason University in Partial Fulfillment of The Requirements for the Degrees of Master of Science Conflict Analysis and Resolution Master of Arts Conflict Resolution and Mediterranean Security Committee: ___________________________________________ Chair of Committee ___________________________________________ ___________________________________________ ___________________________________________ Graduate Program Director ___________________________________________ Dean, School for Conflict Analysis and Resolution Date: _____________________________________ Fall Semester 2017 George Mason University Fairfax, VA University of Malta Valletta, Malta On the Beat: Understanding Portrayals of Law Enforcement Officers in Hip-hop Lyrics Since 2009 A Thesis submitted in partial fulfillment of the requirements for the degrees of Master of Science at George Mason University and Master of Arts at the University of Malta by Francesca A. Keesee Bachelor of Arts University of Virginia, 2015 Director: Juliette Shedd, Professor School for Conflict Analysis and Resolution Fall Semester 2017 George Mason University Fairfax, Virginia University of Malta Valletta, Malta Copyright 2016 Francesca A. Keesee All Rights Reserved ii DEDICATION This is dedicated to all victims of police brutality. iii ACKNOWLEDGEMENTS I am forever grateful to my best friend, partner in crime, and husband, Patrick. -

The Catholic High School of Baltimore Canticles 2015 Cover Art by Mallory Olivier, ’18
The Catholic High School of Baltimore Canticles 2015 Cover Art by Mallory Olivier, ’18 To The Reader All images in this collection are either in the public domain or have been submitted by students. Chapter Selections are divided by author. The table of contents can be accessed by clicking the table of contents button in your iBooks reader: You can also access the table of contents with a two-finger pinch on your screen or track pad. This collection is designed to be viewed on iPads in the portrait orientation. i 1 Joanna Kouloheras ’18 Poetry Untitled Ally Lanasa ’16 I Heard... I heard a voice, strong and determined, as her lips moved. I heard words, that echoed in my ear with a familiar ring. I heard words, foreign to my tongue. I heard a voice triumphant and unwavering. I heard words of self-confidence and love. I heard words, articulated as clear as a flowering thought. I heard a voice as I looked into the mirror, a voice all my own. Karl Bryullov– Young Russian Girl 3 Finite Time, Infinite Dreams My eyes are open, but I am dreaming. I am awake, but drifting into the world of what will be. I remain in the same physical state, but mentally I am racing the clock. I run after it, the sensation in my heart extending to my legs. I watch the hand move rapidly from seconds to minutes. Tick-ambition roars within me. Tock-abruptly, I am brought back to reality. My heart rages with a burning passion. The dream-I cannot let it go. -

Top 200 Most Requested Songs
Top 200 Most Requested Songs Based on millions of requests made through the DJ Intelligence® music request system at weddings & parties in 2013 RANK ARTIST SONG 1 Journey Don't Stop Believin' 2 Cupid Cupid Shuffle 3 Black Eyed Peas I Gotta Feeling 4 Lmfao Sexy And I Know It 5 Bon Jovi Livin' On A Prayer 6 AC/DC You Shook Me All Night Long 7 Morrison, Van Brown Eyed Girl 8 Psy Gangnam Style 9 DJ Casper Cha Cha Slide 10 Diamond, Neil Sweet Caroline (Good Times Never Seemed So Good) 11 B-52's Love Shack 12 Beyonce Single Ladies (Put A Ring On It) 13 Maroon 5 Feat. Christina Aguilera Moves Like Jagger 14 Jepsen, Carly Rae Call Me Maybe 15 V.I.C. Wobble 16 Def Leppard Pour Some Sugar On Me 17 Beatles Twist And Shout 18 Usher Feat. Ludacris & Lil' Jon Yeah 19 Macklemore & Ryan Lewis Feat. Wanz Thrift Shop 20 Jackson, Michael Billie Jean 21 Rihanna Feat. Calvin Harris We Found Love 22 Lmfao Feat. Lauren Bennett And Goon Rock Party Rock Anthem 23 Pink Raise Your Glass 24 Outkast Hey Ya! 25 Isley Brothers Shout 26 Sir Mix-A-Lot Baby Got Back 27 Lynyrd Skynyrd Sweet Home Alabama 28 Mars, Bruno Marry You 29 Timberlake, Justin Sexyback 30 Brooks, Garth Friends In Low Places 31 Lumineers Ho Hey 32 Lady Gaga Feat. Colby O'donis Just Dance 33 Sinatra, Frank The Way You Look Tonight 34 Sister Sledge We Are Family 35 Clapton, Eric Wonderful Tonight 36 Temptations My Girl 37 Loggins, Kenny Footloose 38 Train Marry Me 39 Kool & The Gang Celebration 40 Daft Punk Feat. -

J Cole Can't Get Enough Free Mp3 Download Best of J
j cole can't get enough free mp3 download Best of J. Cole Mixtape (J. Cole Mp3 songs DJ Mix) Enjoy Best of J cole, Jermaine Lamarr Cole, known professionally as J. Cole is an American rapper, singer, songwriter, record producer, and record executive. Wikipedia Born: 28 January 1985 (age 35 years), Frankfurt, Germany. Best of J. Cole Mixtape is the compilation of Jcole mp3 rap songs. You will like this mix if your a fan of jcole. Download and share. J. Cole – A Tale of 2 Citiez J. Cole – High For Hours J. Cole – No Role Modelz J. Cole – Work Out J. Cole – Fire Squad J. Cole – Let Nas Down J. Cole – Love Yourz J. Cole – Deja Vu J. Cole – Lion King On Ice J. Cole – Neighbors J. Cole – Under The Sun J. Cole – 1985 J. Cole – G.O.M.D. J. Cole – Lights Please J. Cole – The Climb Back J. Cole – False Prophets J. Cole – Snow On Tha Bluff J. Cole – She Knows J. Cole – Kevin’s Heart J. Cole – In the Morning J. Cole – Apparently J. Cole – Change J. Cole – Power Trip J. Cole – January 28th J. Cole – MIDDLE CHILD J. Cole – Crooked Smile J. Cole – everybody dies J. Cole – Sacrifices J. Cole – Lost Ones J. Cole – ATM J. Cole – Wet Dreamz J. Cole – Shea Butter Baby. Download & Enjoy Best of J. Cole Mixtape (J. Cole DJ Mix) Tags: Best J. Cole Mixtape, jcole songs, j. cole mp3 songs Mix, best of j cole dj mix mp3 download, j cole best songs, best of j cole dj mix mp3 free download, best of j cole mixtape, j cole mix 2019, j cole mix, Year 2021 DJ Mix. -

Mediamonkey Filelist
MediaMonkey Filelist Track # Artist Title Length Album Year Genre Rating Bitrate Media # Local 1 Kirk Franklin Just For Me 5:11 2019 Gospel 182 Disk Local 2 Kanye West I Love It (Clean) 2:11 2019 Rap 4 128 Disk Closer To My Local 3 Drake 5:14 2014 Rap 3 128 Dreams (Clean) Disk Nellie Tager Local 4 If I Back It Up 3:49 2018 Soul 3 172 Travis Disk Local 5 Ariana Grande The Way 3:56 The Way 1 2013 RnB 2 190 Disk Drop City Yacht Crickets (Remix Local 6 5:16 T.I. Remix (Intro 2013 Rap 128 Club Intro - Clean) Disk In The Lonely I'm Not the Only Local 7 Sam Smith 3:59 Hour (Deluxe 5 2014 Pop 190 One Disk Version) Block Brochure: In This Thang Local 8 E40 3:09 Welcome to the 16 2012 Rap 128 Breh Disk Soil 1, 2 & 3 They Don't Local 9 Rico Love 4:55 1 2014 Rap 182 Know Disk Return Of The Local 10 Mann 3:34 Buzzin' 2011 Rap 3 128 Macc (Remix) Disk Local 11 Trey Songz Unusal 4:00 Chapter V 2012 RnB 128 Disk Sensual Local 12 Snoop Dogg Seduction 5:07 BlissMix 7 2012 Rap 0 201 Disk (BlissMix) Same Damn Local 13 Future Time (Clean 4:49 Pluto 11 2012 Rap 128 Disk Remix) Sun Come Up Local 14 Glasses Malone 3:20 Beach Cruiser 2011 Rap 128 (Clean) Disk I'm On One We the Best Local 15 DJ Khaled 4:59 2 2011 Rap 5 128 (Clean) Forever Disk Local 16 Tessellated Searchin' 2:29 2017 Jazz 2 173 Disk Rahsaan 6 AM (Clean Local 17 3:29 Bleuphoria 2813 2011 RnB 128 Patterson Remix) Disk I Luh Ya Papi Local 18 Jennifer Lopez 2:57 1 2014 Rap 193 (Remix) Disk Local 19 Mary Mary Go Get It 2:24 Go Get It 1 2012 Gospel 4 128 Disk LOVE? [The Local 20 Jennifer Lopez On the -

The Ukrainian Weekly 1939, No.33
www.ukrweekly.com vm Supplement to the 8V0B3DA, Ukrainian Dally •яя липні in ***&*** No. 33 JERSEY СГГЖ; N, J., SATURDAY AUOUSfrlS, 193» VDb, VII я POLISH PERSECUTION OF A COMMON PROPAGANDA UKRAINIANS TRICK CAUSES OF- DIS-H-AR-M-ON During the month of June Po Where in. formes times. Poland Д NYONE who. is really interested. in Ще development of lish- authorities tried thirty-six jailed Ukrainian patriots for what, Ukrainian priests for so-called Uk- they were, now. she is taking ad- •**• Ukrainian-American liter must be truly dismayed by rainization of names and, passed-a vantage> of. the current, feeling the scarcity,, of harmonious. relations. and good will among total sentence, of - 231- months' im among. Western. Powers against a good portion of: our active young; people. Tftere. appears prisonment. Most of the" sentences the Nazis by. charging Ulwunian. were suspended, from two^to five patriots whom she arrests with to be tendency among them to split up into factions. To be years. being Nazi spies. Previously Uk- sure, this tendency is as yet incipient.. Perhaps.it is.only In this connection-the court sen ? rainians alone were held responsi- a passing phase, something that will soon disappear as more tenced a peasant from the-village ble for every outbreak of anti-Po-" of Mykhnivtsi to-six months' im- lish feeling resulting from Polish of our younger: generation perceive the-dangers, of factional . prisonment, because he.- insisted excesses. Now>- in the words-of a- strife and how much damage it did *t& -their elders. In any that his- new born baby-should New York Times dispatch fronv case, this-tendency must be immediately checked, before it have its name recorded wifh-^&HpP? Warsaw, dated-August 1?Щь Po rainian ending, thgfete^rr^nstefld lish political"- circles Germany fcv seriously impairs the effectiveness of our. -

Considering the Worthy Sacrifice Hip Hop Artists May Need to Make to Reclaim the Heart of Hip Hop, Its People
It’s Not Me, It’s You: Considering the Worthy Sacrifice Hip Hop Artists May Need to Make to Reclaim the Heart of Hip Hop, its People by Sharieka Shontae Botex April, 2019 Director of Thesis: Dr. Wendy Sharer Major Department: English The origins of Hip Hop evidence that the art form was intended to provide more than music to listen to, but instead offer art that delivers messages on behalf of people who were not always listened to. My thesis offers an analysis of Jay-Z and J. Cole’s lyrical content and adds to an ongoing discussion of the potential Hip Hop artists have to be effective leaders for the Black community, whose lyrical content can be used to make positive change in society, and how this ability at times can be compromised by creating content that doesn’t evidence this potential or undermines it. Along with this, my work highlights how some of Jay-Z and J. Cole’s lyrical content exhibits their use of some rhetorical strategies and techniques used in social movements and their use of some African American rhetorical practices and strategies. In addition to this, I acknowledge and discuss points in scholarship that connect with my discussion of their lyrical content, or that aided me in proposing what they could consider for future lyrical content. I analyzed six Jay-Z songs and six J. Cole songs, including one song from their earliest released studio album and one from their most recently released studio album. I examined their lyrical content to document responses to the following questions: What issues and topics are discussed in the lyrics; Is money referenced? If so, how; Is there a message of uplift or unity?; What does the artist speak out against?; What lifestyles and habits are promoted?; What guidance is provided?; What problems are mentioned? and What solutions are offered? In my thesis, I explored Jay-Z and J. -

Susan Mckeown Interview
Susan McKeown Celtic High Priestess Frank Goodman (Puremusic 8/2001) I was living in Heidelberg, Germany in the mid 90s, playing with my brother Billy in a duo called the Goodman Brothers. We’d had a hot review of a good simple record (Crooked Smile, Taxim Records) in the German Rolling Stone, and it was relatively easy to hunt up work and stay alive. We’d go down to Italy and play some great dates, got into Switzerland a little. Take the train to Amsterdam now and then, white knuckle the border crossing back into the Fatherland. It was an interesting time and place. My best friends Sergio and Ingrid lived around the corner, they were Argentineans. We’d jam all the time, Ingrid was a real natural, she could bang on the window and make it sound musical. My German didn’t get too good, but my Spanish sure picked up. After some time, I came back to Nashville, Billy stayed in Heidelberg, married Sabine. He still does a lot of playing over there, we do some dates together now and then. One of the most interesting nights I remember over there involved our feature artist this month. We had a regular gig in town at this Mexican restaurant owned by a good Irish songwriter from Galway named Frank Pyne, he called the place Gringo’s. They often had music at night in those days. It was mostly an expat crowd, a lot of Irish and American people, but a decent outreach into what we considered a hip local element. -

Week 26-2013 Soundscan Chartpack.Xlsx
AllSonyMusicEntertainmenttitlesareboldedandcolorͲcodedbylabelgroup. =ColumbiaRecords =RCARecords =EpicRecords =SonyMusicNashville =REDDistributedTitles =AllOtherSonyMusicLabels/Groups ClickonChartNametojumptothatchart: TheBillboard200 CurrentAlbums AlbumswTEA DigitalSongs DigitalTracks DigitalAlbums NewArtistAlbums CatalogAlbums MusicVideos IndieAlbums VinylAlbums PhysicalAlbums InternetAlbums TopSingles SonyAlbums AlbumsByStrata Billboard200ͲWeek26Ͳ2013SoundScanChartpack.xlsx CHART:TopAlbums:BillboardTop200 Weeks Label 2W LW TW Artist Title TW % LW RTD On Rank Rank Rank Sales CHG Sales Sales 1 ATL 1 WALE THEGIFTED 158,325 999 149 158,474 2 COL 2 2 COLE*J. BORNSINNER 84,425 Ͳ72 296,642 381,400 2 DEF 1 3 WEST*KANYE YEEZUS 64,501 Ͳ80 326,841 391,515 1 ATLG 4 SKILLET RISE 59,594 999 242 60,001 6 COL 2 6 5 DAFTPUNK RANDOMACCESSMEMORIES 30,988 Ͳ23 40,079 613,651 30 RͲRN 5 8 6 FLORIDAGEORGIALINE HERE'STOTHEGOODTIMES 30,805 Ͳ7 33,255 790,970 1 MOT 7 INDIA.ARIE SONGVERSATION 30,555 999 149 30,704 43 INT 11 10 8 IMAGINEDRAGONS NIGHTVISIONS 28,919 13 25,596 1,108,815 1 T&NR 9 AUGUSTBURNSRED RESCUE&RESTORE 25,661 999 164 25,858 3RͲRR 1 5 10 BLACKSABBATH 13 25,364 Ͳ44 45,523 226,938 2RͲRR 4 11 ROWLAND*KELLY TALKAGOODGAME 24,580 Ͳ64 67,886 92,703 38 MACK 17 15 12 MACKLEMORE&RYANLEWIS THEHEIST 23,404 3 22,783 866,795 29 ATLG 19 11 13 MARS*BRUNO UNORTHODOXJUKEBOX 22,849 Ͳ10 25,423 1,465,691 2 RTUM 3 14 MILLER*MAC WATCHINGMOVIESWITHTHESOUND 22,833 Ͳ78 101,600 124,541 14 WAR 7 12 15 SHELTON*BLAKE BASEDONATRUESTORY 22,322 Ͳ11 25,037 702,706 65 ATLG 80 7 -

Crooked Smile J Cole Mp3
Crooked smile j cole mp3 Continue 5:36 J. Cole - Curve Smile (Video) foot TLC 496 K 63 M 4:37 J. Cole ft. TLC - Curve Smile (LYRICS) 325 K 34 M 4:38 J. Cole - Wry smile foot TLC (Official Audio) 21 K 4 M 4:39 Curve Smile 14 52 K 4:39 J.Cole feat. TLC - Curve Smile 0 479 5:25 J. Cole - Wry smile (Live at iHeartRadio Music Festival) 5 K 600 K 4:39 J. Cole - Wry smile (Explicit) 34 30 K 4:40 J. Cole - Wry smile (Live on Letterman) 2 K 921 K 4:43 Curve Smile - J. Cole foot TLC - Official Music Lyrics 7 1 K 4:54 J.Cole performs Crooked Smile LIVE at POWER 106 4 K 512 K 4:01 J. Cole - Wet Dreamz (Video) 1 M 155 M 4:43 Curve Smile - j. Lyrics Cole 77 8 K 6:47 J. Cole (Crooked) / SiriusXM / Hip-Hop Nation 272 178 K 4:03 J. Cole - Power Trip (Internet) Miguel 679 K 74 M 2:48 Curve Smile (J Cole cover) 67 13 K 4:17 J Cole - Wry smile foot. TLC (1 hour) 22 4 K 4:37 J. Cole - Wry Smile Lyrics-Clean 2 K 567 K 4:39 Curve Smile - J. Cole Foot TLC (Lyrica) 503 51 K 4:54 J. Cole - 14 Smile TLC CLEAN 34 36 K Wry smile J. Cole - Cover wesley Stromberg and Kenny Holland 4 K 649 K Gaana English Songs Crooked Smile Songs Requested Tracks Are Not Available in Your Region Listen to J. -

Lift Ev'ry Voice & Sing for an Afrocentric Pedagogy Of
LIFT EV’RY VOICE & SING FOR AN AFROCENTRIC PEDAGOGY OF MUSIC TEACHING AND LEARNING by David Wayne Robinson, Jr. Dissertation Committee: Professor Mariana Souto-Manning, Co-sponsor Professor Christopher Emdin, Co-sponsor Professor Yolanda Sealy-Ruiz Approved by the Committee on the Degree of Doctor of Education Date May 20, 2020 Submitted in partial fulfillment of the requirements for the degree of Doctor of Education Teachers College, Columbia University 2020 ABSTRACT LIFT EV’RY VOICE & SING FOR AN AFROCENTRIC PEDAGOGY OF MUSIC TEACHING AND LEARNING David Wayne Robinson, Jr. Currently, Eurocentric theories and practices of urban teachers and students are often studied under a White gaze of expected deficits. Much of this research is quantitative (e.g., documenting the number of teachers of color); the qualitative research that documents the experiences of people of color usually lacks the personal lived experiences of racial marginalization that only one who has endured them can tell. Addressing this research problem, in this dissertation, I share findings generated from a 9-month autoethnographic study of my experiences in light of the blockade of anti-Black epistemologies and ontologies in (music) teacher education. Framed by Critical Race Theory, Critical Pedagogy, and Postcolonial Theory, the aim of this study is to examine the lived experiences and narratives of a Black-queer doctoral student and teacher educator—in dialogue with majority Black and Latinx preservice early childhood and elementary students in his music teacher education -

Download Jcole Album ALBUM: Dreamville & J
download jcole album ALBUM: Dreamville & J. Cole – Revenge of the Dreamers III Director’s (ZIP) Dreamville & J. Cole drops a new album “Revenge of the Dreamers III Director’s” and it right here for your fast download. DOWNLOAD HERE. Download Dreamville & J. Cole – Revenge of the Dreamers III Director’s Below: Get Updates On Our Telegram Channel. Related Articles. ALBUM: J. Cole – The Off-Season. DOWNLOAD!! J. Cole The Off-Season ZIP DOWNOAD J. Cole comes through with a new 12 tracks album project titled “The Off-Season” and is right here for your fast download. DOWNLOAD HERE Download J. Cole – The […] ALBUM: Dreamville & J. Cole – Revenge of the Dreamers III Director’s (ZIP FILE) Dreamville & J. Cole Revenge of the Dreamers III Director’sAlbum Zip Download. Zip Download Dreamville & J. Cole Revenge of the Dreamers III Director’s album, Dreamville & J. Cole Revenge of the Dreamers III Director’s Zip Download is a titled brand new music album dropped by Dreamville & J. Cole , and right below you can download Dreamville & J. Cole Revenge of the Dreamers III Director’s Zip Download in any of these formats Zip, Mp3, Rar. DOWNLOAD NOW. We are sure this new project from Dreamville & J. Cole – Revenge of the Dreamers III Director’s won’t let you down on search. For More Zip Files mp3 album download, check it out. We know you have sought for mp3 download, mp4 video, download music mp3, zip download, hiphop song, hit song &, etc. If you are in need of such, visit the homepage. You can now stream & download Dreamville & J.