Council of Governors 19Th February 2018 Public
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cobia Database Articles Final Revision 2.0, 2-1-2017
Revision 2.0 (2/1/2017) University of Miami Article TITLE DESCRIPTION AUTHORS SOURCE YEAR TOPICS Number Habitat 1 Gasterosteus canadus Linné [Latin] [No Abstract Available - First known description of cobia morphology in Carolina habitat by D. Garden.] Linnaeus, C. Systema Naturæ, ed. 12, vol. 1, 491 1766 Wild (Atlantic/Pacific) Ichthyologie, vol. 10, Iconibus ex 2 Scomber niger Bloch [No Abstract Available - Description and alternative nomenclature of cobia.] Bloch, M. E. 1793 Wild (Atlantic/Pacific) illustratum. Berlin. p . 48 The Fisheries and Fishery Industries of the Under this head was to be carried on the study of the useful aquatic animals and plants of the country, as well as of seals, whales, tmtles, fishes, lobsters, crabs, oysters, clams, etc., sponges, and marine plants aml inorganic products of U.S. Commission on Fisheries, Washington, 3 United States. Section 1: Natural history of Goode, G.B. 1884 Wild (Atlantic/Pacific) the sea with reference to (A) geographical distribution, (B) size, (C) abundance, (D) migrations and movements, (E) food and rate of growth, (F) mode of reproduction, (G) economic value and uses. D.C., 895 p. useful aquatic animals Notes on the occurrence of a young crab- Proceedings of the U.S. National Museum 4 eater (Elecate canada), from the lower [No Abstract Available - A description of cobia in the lower Hudson Eiver.] Fisher, A.K. 1891 Wild (Atlantic/Pacific) 13, 195 Hudson Valley, New York The nomenclature of Rachicentron or Proceedings of the U.S. National Museum Habitat 5 Elacate, a genus of acanthopterygian The universally accepted name Elucate must unfortunately be supplanted by one entirely unknown to fame, overlooked by all naturalists, and found in no nomenclator. -

Common Errors in English by Paul Brians [email protected]
Common Errors in English by Paul Brians [email protected] http://www.wsu.edu/~brians/errors/ (Brownie points to anyone who catches inconsistencies between the main site and this version.) Note that italics are deliberately omitted on this page. What is an error in English? The concept of language errors is a fuzzy one. I'll leave to linguists the technical definitions. Here we're concerned only with deviations from the standard use of English as judged by sophisticated users such as professional writers, editors, teachers, and literate executives and personnel officers. The aim of this site is to help you avoid low grades, lost employment opportunities, lost business, and titters of amusement at the way you write or speak. But isn't one person's mistake another's standard usage? Often enough, but if your standard usage causes other people to consider you stupid or ignorant, you may want to consider changing it. You have the right to express yourself in any manner you please, but if you wish to communicate effectively you should use nonstandard English only when you intend to, rather than fall into it because you don't know any better. I'm learning English as a second language. Will this site help me improve my English? Very likely, though it's really aimed at the most common errors of native speakers. The errors others make in English differ according to the characteristics of their first languages. Speakers of other languages tend to make some specific errors that are uncommon among native speakers, so you may also want to consult sites dealing specifically with English as a second language (see http://www.cln.org/subjects/esl_cur.html and http://esl.about.com/education/adulted/esl/). -

Massachusetts Institute of Technology Bulletin
d 7I THE DEAN OF SCIEN<C OCT 171972 MASSACHUSETTS INSTITUTE OF TECHNOLOGY BULLETIN REPORT OF THE PRESIDENT 1971 MASSACHUSETTS INSTITUTE OF TECHNOLOGY BULLETIN REPORT OF THE PRESIDENT FOR THE ACADEMIC YEAR 1970-1971 MASSACHUSETTS INSTITUTE OF TECHNOLOGY BULLETIN VOLUME 107, NUMBER 2, SEPTEMBER, 1972 Published by the Massachusetts Institute of Technology 77 MassachusettsAvenue, Cambridge, Massachusetts, five times yearly in October, November, March, June, and September Second class postage paid at Boston, Massachusetts. Issues of the Bulletin include REPORT OF THE TREASURER REPORT OF THE PRESIDENT SUMMER SESSION CATALOGUE PUBLICATIONS AND THESES and GENERAL CATALOGUE Send undeliverable copies and changes of address to Room 5-133 Massachusetts Institute of Technology Cambridge,Massachusetts 02139. THE CORPORATION Honorary Chairman:James R. Killian, Jr. Chairman:Howard W. Johnson President:Jerome B. Wiesner Chancellor: Paul E. Gray Vice Presidentand Treasurer:Joseph J. Snyder Secretary:John J. Wilson LIFE MEMBERS Bradley Dewey, Vannevai Bush, James M. Barker, Thomas C. Desmond, Marshall B. Dalton, Donald F. Carpenter, Thomas D. Cabot, Crawford H. Greenewalt, Lloyd D. Brace, William A. Coolidge, Robert C. Sprague, Charles A. Thomas, David A. Shepard, George J. Leness, Edward J. Hanley, Cecil H. Green, John J. Wilson, Gilbert M. Roddy, James B. Fisk, George P. Gardner, Jr., Robert C. Gunness, Russell DeYoung, William Webster, William B. Murphy, Laurance S. Rockefeller, Uncas A. Whitaker, Julius A. Stratton, Luis A. Ferr6, Semon E. Knudsen, Robert B. Semple, Ir6n6e du Pont, Jr., Eugene McDermott, James R. Killian, Jr. MEMBERS Albert H. Bowker, George P. Edmonds, Ralph F. Gow, Donald A. Holden, H. I. Romnes, William E. -

Objective Is
Lehigh Preserve Institutional Repository Design of a microprocessor-based emulsion polymerization process control facility Dimitratos, John N. 1987 Find more at https://preserve.lib.lehigh.edu/ This document is brought to you for free and open access by Lehigh Preserve. It has been accepted for inclusion by an authorized administrator of Lehigh Preserve. For more information, please contact [email protected]. Design of a Microprocessor-based Emulsion Polymerization Process Control Facility A research report written in partial fulfillment of the requirements for the degree of Master of Science in Chemical F:ngim·ering, Lehigh University, Bethlehem, Pennsylvania by John N. Dimitratos June 1987 ,. Design of a Microprocessor-based Emulsion Polymerization .. ,_.,,-•• ·, ,, -i •:>:.·.:':' Process Control Facility ' A research report written in partial fulfillment of the requirements for the degree of Master of Science in Chemical Engineering, Lehigh University, Bethlehem, Pennsylvania by John N. Dimitratos June 1987 •1 to my father and my brother there art times when it is hard to decide what should be chosen at what price, and what endured in return for what reward. Perhaps it is still harder to stick to the decision Aristotle (384-322 B.C) Ethics, Book Ill. Abstract The explosion of microcomputer technology and the recent developments in software and hardware products introduce a new horizon of capabilities for the process control engineer. However, taking advantage of this new technology is not something easily done. H the process control engineer has to undertake such a project soon he will have to deal with the different languages the software engineer and the plant operator use. -
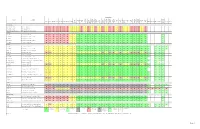
Operating System Support Matrix
Operating System Win Win Win Win Win Win Win Win THEOS Product Description Win Win Win Win Windows Win XP Win XP Server Server Server Server Server Server Win 7 Win 7 Win 8 Win 8 Server Server Win 8.1 Win 8.1 Corona DOS Win 3.x Win NT4 Win 95 Win 98 Win 98SE Win Me Win 2000 Server Server Vista Vista Thin a Mac 8.6+ QNX 6.2 THEOS SCO 5.07 SCO 6.0 32 64 2003 2003 R2 2003 R2 2008 2008 2008 R2 32 64 32 64 2012 2012 R2 32 64 Linux Ver. 5.0 2000 2003 64 32 64 Client 32 32 64 32 64 64 64 64 PL182 USB-Serial Links USB-Serial Link 2-232-DB9 Two RS-232, 9-pin DB-9s USB-Serial Link 4-232-DB9 Four RS-232, 9-pin DB-9s USB-Serial Link 4-232-DB9 Cabled Four RS-232, 9-pin DB-9s with fan-out cable Serial PCIe SSerial-PCIe One 25-pin port, 16550 UART SSerial-PCIe/LP One 25-pin port, 16550 UART, low-profile DSerial-PCIe Two 9-pin ports, 16550 UARTs DSerial-PCIe/LP Two 9-pin ports, 16550 UARTs, low-profile Quattro-PCIe Four 9-pin ports, 16550 UARTs Serial PCI SSerial-PCI One 9-pin port, 16550 UART ? SSerial-PCI/LP One 25-pin port, 16550 UART, low-profile ? RS422 SS-PCI One 9-pin port, 16550 UART, RS-422 pinout ? LavaPort-650 One 9-pin port, 16650 UART ? DSerial-PCI Two 9-pin ports, 16550 UARTs -

The Search for Immortality in Archaic Greek Myth
The Search for Immortality in Archaic Greek Myth Diana Helen Burton PhD University College, University of London 1996 ProQuest Number: 10106847 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest. ProQuest 10106847 Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States Code. Microform Edition © ProQuest LLC. ProQuest LLC 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106-1346 Abstract This thesis considers the development of the ideology of death articulated in myth and of theories concerning the possibility, in both mythical and 'secular' contexts, of attaining some form of immortality. It covers the archaic period, beginning after Homer and ending with Pindar, and examines an amalgam of (primarily) literary and iconographical evidence. However, this study will also take into account anthropological, archaeological, philosophical and other evidence, as well as related theories from other cultures, where such evidence sheds light on a particular problem. The Homeric epics admit almost no possibility of immortality for mortals, and the possibility of retaining any significant consciousness of 'self' or personal identity after death and integration into the underworld is tailored to the poems rather than representative of any unified theory or belief. The poems of the Epic Cycle, while lacking Homer's strict emphasis on human mortality, nonetheless show little evidence of the range and diversity of types of immortality which develops in the archaic period. -

High-Order Electromechanical Couplings in Ferroelectrics
High-order electromechanical couplings in ferroelectrics THÈSE NO 6266 (2014) PRÉSENTÉE LE 15 JUILLET 2014 À LA FACULTÉ DES SCIENCES ET TECHNIQUES DE L'INGÉNIEUR LABORATOIRE DE CÉRAMIQUE PROGRAMME DOCTORAL EN SCIENCE ET GÉNIE DES MATÉRIAUX ÉCOLE POLYTECHNIQUE FÉDÉRALE DE LAUSANNE POUR L'OBTENTION DU GRADE DE DOCTEUR ÈS SCIENCES PAR Alexander KVASOV acceptée sur proposition du jury: Prof. H. Hofmann, président du jury Prof. A. Tagantsev, directeur de thèse Prof. J. Hlinka, rapporteur Prof. I. Kornev, rapporteur Prof. N. Marzari, rapporteur Suisse 2014 "Gravitation is not responsible for people falling in love." – Albert Einstein To Bárbara. Acknowledgements I would like to express my high gratitude to my thesis director Prof. Alexander Tagantsev who guided me throughout my thesis. Always available for discussion, always ready to help and explain, he taught me how to solve the problems and moreover how to solve difficult problems myself. His profound understanding and knowledge of almost all areas of physics in combination with his unique talent of explaining complex problems and ideas in a simple way makes him not only an excellent scientist, but also a very good supervisor. Without him this work would never have been accomplished. I would like to thank the members of my thesis jury: Prof. Heinrich Hofmann (EPFL), Prof. Nicola Marzari (EPFL), Prof. Igor Kornev (École Centrale Paris) and Prof. Jirka Hlinka (Institute of Physics, Academy of Sciences of the Czech Republic) I also would like to thank people from Ceramics Laboratory, especially Arnaud Crassous, Leo Mc Gilly, Maxim Gureev, Kaushik Vaideeswaran, Peter Yudin, many others, for interesting and useful discussions in the lab and even more interesting free time out of the lab. -

The Role of Autophagy in Chemical Proteasome Inhibition Model of Retinal Degeneration
International Journal of Molecular Sciences Article The Role of Autophagy in Chemical Proteasome Inhibition Model of Retinal Degeneration Merry Gunawan 1, Choonbing Low 1, Kurt Neo 1, Siawey Yeo 2, Candice Ho 3, Veluchamy A. Barathi 2,4,5, Anita Sookyee Chan 3, Najam A. Sharif 6 and Masaaki Kageyama 1,* 1 Santen-SERI Open Innovation Centre, 20 College Road, The Academia, Singapore 169856, Singapore; [email protected] (M.G.); [email protected] (C.L.); [email protected] (K.N.) 2 Translational Pre-Clinical Model Platform, Singapore Eye Research Institute, 20 College Road, The Academia, Singapore 169856, Singapore; [email protected] (S.Y.); [email protected] (V.A.B.) 3 Singapore Eye Research Institute, 20 College Road, The Academia, Singapore 169856, Singapore; [email protected] (C.H.); [email protected] (A.S.C.) 4 Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore, 21 Lower Kent Ridge Road, Singapore 119077, Singapore 5 Academic Clinical Program in Ophthalmology, Duke-NUS Medical School, 8 College Road, Singapore 169857, Singapore 6 Global Alliance and External Research, Santen Inc., Emeryville, CA 94608, USA; [email protected] * Correspondence: [email protected] Abstract: We recently demonstrated that chemical proteasome inhibition induced inner retinal degeneration, supporting the pivotal roles of the ubiquitin–proteasome system in retinal structural integrity maintenance. In this study, using beclin1-heterozygous (Becn1-Het) mice with autophagic dysfunction, we tested our hypothesis that autophagy could be a compensatory retinal protective mechanism for proteasomal impairment. -

Theos Whitepaper May 8, 2021
TheOS Whitepaper May 8, 2021 Abstract Introduction Agents in TheOS Key TheOS Mechanics Token Utility Economics Token Staking Utility Token Liquidity Mining Utility Interactions The NFT Minting Process The Auction Process THe NFTIZE Process Definitions Appendix I - NFT Pooling Properties DRAFT The Hyper Economy Operating System (THEOS) “Symbolic communication mechanisms played a significant part in the evolutionary process by allowing plants, animals and humans to exchange individual experiences and thus turning collections of relatively isolated organisms into adaptive distributed cognition systems. By providing aggregated information on comparative values of goods and services to participants with bounded interests and rationality, the economic signalling mechanisms give them incentives to adjust their consumption and production efforts in accordance with the collective requirements of all other agents in the system. The suggested model of a "hypereconomic" system combines flows of globally aggregated scalar information on prices with mechanisms for sharing knowledge about situational utilities of groups of resources. The project presents methods for combining value and utility signalling mechanisms, introduces non-scalar representations of common experiences analogous to derivative financial instruments and researches their efficiency in different types of economics environments.” Source: https://ieeexplore.ieee.org/document/713811 p. 1 Abstract We propose TheOS, an ecosystem design that is set to accommodate the demands of the emerging hyper-economy. While not a vigorously defined academic term, hyper-economy is an ecosystem that is much closer to the Arrow-Debreu complete markets setup, an ecosystem that builds upon the assumption of availability of global instant liquidity for any asset as well as transparent and complete information sets available to every market agent. -
Tech Giants, Artificial Intelligence, and the Future of Journalism
Tech Giants, Artificial Intelligence, and the Future of Journalism This book examines the impact of the “Big Five” technology companies – Apple, Google, Amazon, Facebook, and Microsoft – on journalism and the media industries. It looks at the current role of algorithms and artifi- cial intelligence in curating how we consume media and their increasing influence on the production of the news. Exploring the changes that the technology industry and automation have made in the past decade to the production, distribution, and con- sumption of news globally, the book considers what happens to journal- ism once it is produced and enters the media ecosystems of the Internet tech giants – and the impact of social media and AI on such things as fake news in the post-truth age. The audience for this book are students and researchers working in the field of digital media, and journalism studies or media studies more generally. It will also be useful to those who are looking for ex- tended case studies of the role taken by tech giants such as Facebook and Google in the fake news scandal, or the role of Jeff Bezos in transforming The Washington Post. Jason Whittaker is the Head of the School of English and Journalism at the University of Lincoln. He worked for 15 years as a tech journalist and has written extensively on magazine journalism and digital media, most recently as the co-editor of the collection Online Journalism in Africa (2013) and as the author of Magazine Production (2016). Routledge Research in Journalism 19 News of Baltimore Race, Rage and the City Edited by Linda Steiner and Silvio Waisbord 20 The Trump Presidency, Journalism, and Democracy Edited by Robert E. -

IBM Personal Software Products
Winter, 1996 OPERATING SYSTEMS HOST ADAPTERS TESTED IBM Personal Software Products APA™-348 OS/2 WARP APA™-358 APA™-1460 AVA™-1505 AHA®-1510 With OS/2 Warp you can dictate a memo and navigate the Internet by AVA™-1515 simply talking. Use your voice to launch popular DOS, OS/2, AHA®-1520/2 Windows 3.1 and Java applications. OS/2 Warp 4 provides a clear AHA®-1530/2P path to a connected world. You can link to colleagues, customers and AHA®-1540/2/F/P the Internet. Set up peer-to-peer networks and tap into a variety of AHA®-1640 AHA®-1740/2/4 servers from work, home or on the road. This battle-tested operating AHA®-2740/2/4/T/W system provides improved security and tools to manage your network AHA®-2840/2VL easily. OS/2 Warps's wealth of connectivity function helps you save AHA®-2910A/Ai time and money in setting up your network. AHA®-2940/4/W AHA®-2940/4/U/UW AHA®-3940/W AHA®-3940U/UW LANGUAGE(S) SUPPORTED PRODUCTS AVAILABLE IN Worldwide 1140 BURNET ROAD • AUSTIN, TX 78758 • PHONE (512) 838-9926 TOLL FREE 800-3IBM-OS2 E-MAIL FAX URL http://www.austin.ibm.com/pspinfo Adaptec Compatibility Directory: A Guide to Products Compatible with Adaptec Host Adapters 1 Winter, 1996 OPERATING SYSTEMS HOST ADAPTERS TESTED Lynx Real-Time Systems APA™-1460 LYNXOS AHA®-1520/2 AHA®-1540/2/F/P AHA®-1740/2/4 The LynxOS is highly modular and scalable. At its fullest, it is a self- hosted development environment consisting of software development tools, UNIX compatible utilities, industry standard networking, a graphical user interface, and a UNIX-like file system. -
THEOS/OASIS User's Handbook
Weber/31-6/$17.95 US THEOS/OASIS User's Handbook A comprehensive guide to the business applications and functions of the THEOS operating system. by Walter C. Stagner Jr. THEOS User's Handbook by Walter c. Stagner Jr. Weber Systems, Inc. Cleveland, Ohio The authors have exercised due care in the preparation of this book and the programs contained in it. The authors and the publisher make no warran ties either express or implied with regard to the information and programs contained in this book. In no event shall the authors or publisher be liable for incidental or consequential damages arising out of the furnishing, perfor mance, or use of this book and/ or its programs. THEOS'· and THEOS86 are trademarks of THEOS Software Corp. Z80'· is a trademark of Zilog Corp. RM Cobol'· is"a trademark of Ryan-McFarland Lotus 1-2-3'· is a trademark of Lotus Development Corp. Apple DOS'· is a trademark of Apple Computer Corp. CPM'· is a trademark of Digital Research Inc. MS-DOS'· is a trademark of Microsoft Corp. Spellbinder'· is a trademark of Lexisoft Inc. multiWRITE'· and multi CALC· are trademarks of Logic Extension Resources UNIX'· is a trademark of Bell Laboratories Published by: Weber Systems, Inc. 8437 Mayfield Road Chesterland, Ohio '44026 For information on translations and book distributors outside of the United States, please contact WSI at the above address. THEOS User's Handbook Copyright© 1985 by Weber Systems, Inc. All rights reserved under International and Pan-American Copyright Conventions. Printed in United States of America. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopy, recording, or otherwise without the prior written permission of the publisher.