Overview of Selected Zoonotic Mosquito-Borne Viruses in Florida
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Mosquito Species Identification Using Convolutional Neural Networks With
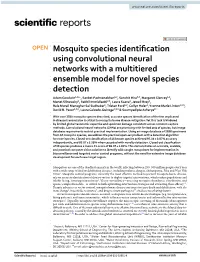
www.nature.com/scientificreports OPEN Mosquito species identifcation using convolutional neural networks with a multitiered ensemble model for novel species detection Adam Goodwin1,2*, Sanket Padmanabhan1,2, Sanchit Hira2,3, Margaret Glancey1,2, Monet Slinowsky2, Rakhil Immidisetti2,3, Laura Scavo2, Jewell Brey2, Bala Murali Manoghar Sai Sudhakar1, Tristan Ford1,2, Collyn Heier2, Yvonne‑Marie Linton4,5,6, David B. Pecor4,5,6, Laura Caicedo‑Quiroga4,5,6 & Soumyadipta Acharya2* With over 3500 mosquito species described, accurate species identifcation of the few implicated in disease transmission is critical to mosquito borne disease mitigation. Yet this task is hindered by limited global taxonomic expertise and specimen damage consistent across common capture methods. Convolutional neural networks (CNNs) are promising with limited sets of species, but image database requirements restrict practical implementation. Using an image database of 2696 specimens from 67 mosquito species, we address the practical open‑set problem with a detection algorithm for novel species. Closed‑set classifcation of 16 known species achieved 97.04 ± 0.87% accuracy independently, and 89.07 ± 5.58% when cascaded with novelty detection. Closed‑set classifcation of 39 species produces a macro F1‑score of 86.07 ± 1.81%. This demonstrates an accurate, scalable, and practical computer vision solution to identify wild‑caught mosquitoes for implementation in biosurveillance and targeted vector control programs, without the need for extensive image database development for each new target region. Mosquitoes are one of the deadliest animals in the world, infecting between 250–500 million people every year with a wide range of fatal or debilitating diseases, including malaria, dengue, chikungunya, Zika and West Nile Virus1. -

Pesticide Discharge Management Plan
Pesticide Discharge Management Plan 1. PDMP Team a. Person(s) responsible for managing pests in relation to pest management area: All operational and biological support staff along with the Director of Mosquito Management Services (Wade Brennan, 5531 Pinkney Ave. Sarasota, FL. 34233) b. Person(s) responsible for developing and revising PDMP John Eaton, Operations Supervisor, and Wade Brennan Environmental Scientist III, are the individuals responsible for monitoring changes in Federal and State regulatory agencies that govern mosquito control operations. c. John Eaton, and Wade Brennan, are the individuals responsible for developing, revising and implementing corrective actions and other effluent requirements d. Person(s) responsible for pesticide applications Persons (supervisors and above) who direct applicators these include: All Operational staff employed by Sarasota County Mosquito Management Services that hold a Public Health Pest Control License administered by Florida Department of Agriculture and Consumer Services are directly responsible for pesticide applications (because they can oversee uncertified applicators) additionally, Sarasota County’s awarded Contractors must have required state certification (s). 2. Pest Management Area Description Overview Sarasota County Mosquito Management Services (SCMMS) has been mitigating pestiferous nuisance host seeking mosquitoes of public health importance for over 60 years. A total of forty- four mosquito species are found in Sarasota County of which a dozen are in need of management through a typical peak mosquito season, April through November. When intervention action plans are developed and implemented more than one species is usually involved. Past and current mitigation strategies for both larval and adult mosquitoes have always been in full compliance with FIFRA conditions which have met water quality standards. -
Investigating the Role of Host TTR-Rbps During SFV4 and MHV-68 Infection
Investigating the role of host TTR-RBPs during SFV4 and MHV-68 infection Thesis submitted in accordance with the requirements of the University of Liverpool for the degree of Doctor in Philosophy by Jamie Casswell October 2019 Contents Figure Contents Page……………………………………………………………………………………7 Table Contents Page…………………………………………………………………………………….9 Acknowledgements……………………………………………………………………………………10 Abbreviations…………………………………………………………………………………………….11 Abstract……………………………………………………………………………………………………..17 1. Chapter 1 Introduction……………………………………………………………………………19 1.1 DNA and RNA viruses ............................................................................. 20 1.2 Taxonomy of eukaryotic viruses ............................................................. 21 1.3 Arboviruses ............................................................................................ 22 1.4 Togaviridae ............................................................................................ 22 1.4.1 Alphaviruses ............................................................................................................................. 23 1.4.1.1 Semliki Forest Virus ........................................................................................................... 25 1.4.1.2 Alphavirus virion structure and structural proteins ......................................................... 26 1.4.1.3 Alphavirus non-structural proteins ................................................................................... 29 1.4.1.4 Alphavirus genome organisation -

Catalogo De Los Diptera De Nicaragua. 4. Culicidae (Nematocera)
Rev Rev. Nica. Ent., (1990) 14:19-39. CATALOGO DE LOS DIPTERA DE NICARAGUA. 4. CULICIDAE (NEMATOCERA). Por Jean-Michel Maes * & Pedro Rivera Mendoza.** Resumen. Este catálogo presenta las 40 especies de Culicidae (Diptera : Nematocera) reportadas de Nicaragua. Para cada especie se cita la sinonimia, la distribución geográfica, los hospederos, las enfermedades transmitidas y los enemigos naturales. La bibliografía conocida está agregada. Abstract. This catalogue presents the 40 species of Culicidae (Diptera : Nematocera) reported from Nicaragua. The geographical distribution, synonyms, hosts, diseases transmitted and natural enemies are given for each species. A bibliography of the Nicaraguayan species is included. * Museo Entomológico, A.P. 527, León, Nicaragua. ** Director del Departamento de Entomología Médica del Centro Nacional de Higiene y Epidemiología, Villa Ruben Darío M-254, Managua - 14, Nicaragua. file:///C|/My%20Documents/REVISTA/REV%2014A/14A%20Culicidae.htm (1 of 25) [20/12/2002 03:34:12 p.m.] Rev Introducción. Los Culicidae forman una familia numerosa de Diptera Nematocera. Las larvas son acuáticas, los adultos pueden ser identificados por la venacion alar presentando escamas y la proboscis larga. Son importantes a nivel medico por ser vectores de muchas enfermedades tropicales. Las larvas de zancudos se encuentran en muchos tipos de aguas, por ejemplo en charcos, huecos o recipientos artificiales, cada especie tiene un tipo de agua característico donde se reproduce. Los huevos son dejados en paquetes sobre la superficie del agua. Las larvas comen algas y materia vegetal en decomposición. Las larvas respiran principalmente a la superficie, ayudandose muchas veces de un sifón. La pupas son acuáticas y al contrario de los otros insectos, son bastante activas. -

Eastern Equine Encephalitis (EEE) Description
Eastern Equine Importance Eastern, Western, and Venezuelan equine encephalomyelitis are mosquito-borne, Encephalomyelitis, viral infections that can cause severe encephalitis in horses and humans. Some of Western Equine these viruses also cause disease occasionally in other mammals and birds. No specific treatment is available, and depending on the virus and host, the case fatality rate may Encephalomyelitis and be as high as 90%. As a result of vaccination, severe Eastern (EEE) and Western (WEE) equine encephalomyelitis epidemics no longer occur regularly in the U.S., but Venezuelan Equine sporadic cases and small outbreaks are still seen. Epidemic Venezuelan equine Encephalomyelitis encephalomyelitis (VEE) viruses continue to emerge periodically in South America, and sweep through equine and human populations. One two-year VEE epidemic, Sleeping Sickness which began in 1969, extended from South America to the southern U.S., and caused an estimated 38,000-50,000 cases in equids. Epidemic VEE viruses are also potential Eastern Equine Encephalomyelitis bioterrorist weapons. (EEE) –Eastern Equine Encephalitis, Eastern Encephalitis Etiology Eastern, Western and Venezuelan equine encephalomyelitis result from infection Western Equine Encephalomyelitis by the respectively named viruses in the genus Alphavirus (family Togaviridae). In (WEE) –Western Equine Encephalitis the human literature, the disease is usually called Eastern, Western or Venezuelan equine encephalitis rather than encephalomyelitis. Venezuelan Equine Encephalomyelitis (VEE) –Peste Loca, Venezuelan Equine Eastern equine encephalomyelitis virus Encephalitis, Venezuelan Encephalitis, The numerous isolates of the Eastern equine encephalomyelitis virus (EEEV) can Venezuelan Equine Fever be grouped into two variants. The variant found in North America is more pathogenic than the variant that occurs in South and Central America. -

MOSQUITOES of the SOUTHEASTERN UNITED STATES
L f ^-l R A R > ^l^ ■'■mx^ • DEC2 2 59SO , A Handbook of tnV MOSQUITOES of the SOUTHEASTERN UNITED STATES W. V. King G. H. Bradley Carroll N. Smith and W. C. MeDuffle Agriculture Handbook No. 173 Agricultural Research Service UNITED STATES DEPARTMENT OF AGRICULTURE \ I PRECAUTIONS WITH INSECTICIDES All insecticides are potentially hazardous to fish or other aqpiatic organisms, wildlife, domestic ani- mals, and man. The dosages needed for mosquito control are generally lower than for most other insect control, but caution should be exercised in their application. Do not apply amounts in excess of the dosage recommended for each specific use. In applying even small amounts of oil-insecticide sprays to water, consider that wind and wave action may shift the film with consequent damage to aquatic life at another location. Heavy applications of insec- ticides to ground areas such as in pretreatment situa- tions, may cause harm to fish and wildlife in streams, ponds, and lakes during runoff due to heavy rains. Avoid contamination of pastures and livestock with insecticides in order to prevent residues in meat and milk. Operators should avoid repeated or prolonged contact of insecticides with the skin. Insecticide con- centrates may be particularly hazardous. Wash off any insecticide spilled on the skin using soap and water. If any is spilled on clothing, change imme- diately. Store insecticides in a safe place out of reach of children or animals. Dispose of empty insecticide containers. Always read and observe instructions and precautions given on the label of the product. UNITED STATES DEPARTMENT OF AGRICULTURE Agriculture Handbook No. -

Taxonomy of the Order Bunyavirales: Update 2019
Archives of Virology (2019) 164:1949–1965 https://doi.org/10.1007/s00705-019-04253-6 VIROLOGY DIVISION NEWS Taxonomy of the order Bunyavirales: update 2019 Abulikemu Abudurexiti1 · Scott Adkins2 · Daniela Alioto3 · Sergey V. Alkhovsky4 · Tatjana Avšič‑Županc5 · Matthew J. Ballinger6 · Dennis A. Bente7 · Martin Beer8 · Éric Bergeron9 · Carol D. Blair10 · Thomas Briese11 · Michael J. Buchmeier12 · Felicity J. Burt13 · Charles H. Calisher10 · Chénchén Cháng14 · Rémi N. Charrel15 · Il Ryong Choi16 · J. Christopher S. Clegg17 · Juan Carlos de la Torre18 · Xavier de Lamballerie15 · Fēi Dèng19 · Francesco Di Serio20 · Michele Digiaro21 · Michael A. Drebot22 · Xiaˇoméi Duàn14 · Hideki Ebihara23 · Toufc Elbeaino21 · Koray Ergünay24 · Charles F. Fulhorst7 · Aura R. Garrison25 · George Fú Gāo26 · Jean‑Paul J. Gonzalez27 · Martin H. Groschup28 · Stephan Günther29 · Anne‑Lise Haenni30 · Roy A. Hall31 · Jussi Hepojoki32,33 · Roger Hewson34 · Zhìhóng Hú19 · Holly R. Hughes35 · Miranda Gilda Jonson36 · Sandra Junglen37,38 · Boris Klempa39 · Jonas Klingström40 · Chūn Kòu14 · Lies Laenen41,42 · Amy J. Lambert35 · Stanley A. Langevin43 · Dan Liu44 · Igor S. Lukashevich45 · Tāo Luò1 · Chuánwèi Lüˇ 19 · Piet Maes41 · William Marciel de Souza46 · Marco Marklewitz37,38 · Giovanni P. Martelli47 · Keita Matsuno48,49 · Nicole Mielke‑Ehret50 · Maria Minutolo3 · Ali Mirazimi51 · Abulimiti Moming14 · Hans‑Peter Mühlbach50 · Rayapati Naidu52 · Beatriz Navarro20 · Márcio Roberto Teixeira Nunes53 · Gustavo Palacios25 · Anna Papa54 · Alex Pauvolid‑Corrêa55 · Janusz T. Pawęska56,57 · Jié Qiáo19 · Sheli R. Radoshitzky25 · Renato O. Resende58 · Víctor Romanowski59 · Amadou Alpha Sall60 · Maria S. Salvato61 · Takahide Sasaya62 · Shū Shěn19 · Xiǎohóng Shí63 · Yukio Shirako64 · Peter Simmonds65 · Manuela Sironi66 · Jin‑Won Song67 · Jessica R. Spengler9 · Mark D. Stenglein68 · Zhèngyuán Sū19 · Sùróng Sūn14 · Shuāng Táng19 · Massimo Turina69 · Bó Wáng19 · Chéng Wáng1 · Huálín Wáng19 · Jūn Wáng19 · Tàiyún Wèi70 · Anna E. -

Wing Variation in Culex Nigripalpus (Diptera: Culicidae) in Urban Parks
de Carvalho et al. Parasites & Vectors (2017) 10:423 DOI 10.1186/s13071-017-2348-5 RESEARCH Open Access Wing variation in Culex nigripalpus (Diptera: Culicidae) in urban parks Gabriela Cristina de Carvalho1, Daniel Pagotto Vendrami2, Mauro Toledo Marrelli1,2 and André Barretto Bruno Wilke1* Abstract Background: Culex nigripalpus has a wide geographical distribution and is found in North and South America. Females are considered primary vectors for several arboviruses, including Saint Louis encephalitis virus, Venezuelan equine encephalitis virus and Eastern equine encephalitis virus, as well as a potential vector of West Nile virus. In view of the epidemiological importance of this mosquito and its high abundance, this study sought to investigate wing variation in Cx. nigripalpus populations from urban parks in the city of São Paulo, Brazil. Methods: Female mosquitoes were collected in seven urban parks in the city of São Paulo between 2011 and 2013. Eighteen landmark coordinates from the right wing of each female mosquito were digitized, and the dissimilarities between populations were assessed by canonical variate analysis and cross-validated reclassification and by constructing a Neighbor-Joining (NJ) tree based on Mahalanobis distances. The centroid size was calculated to determine mean wing size in each population. Results: Canonical variate analysis based on fixed landmarks of the wing revealed a pattern of segregation between urban and sylvatic Cx. nigripalpus, a similar result to that revealed by the NJ tree topology, in which the population from Shangrilá Park segregated into a distinct branch separate from the other more urban populations. Conclusion: Environmental heterogeneity may be affecting the wing shape variation of Cx. -

Notification Requirements
Protocol for Public Health Agencies to Notify CDC about the Occurrence of Nationally Notifiable Conditions, 2021 Categorized by Notification Timeliness IMMEDIATELY NOTIFIABLE, EXTREMELY URGENT: Call the CDC ROUTINELY NOTIFIABLE: Submit electronic case notification Emergency Operations Center (EOC) at 770.488.7100 within 4 hours of within the next reporting cycle. a case meeting the notification criteria, followed by submission of an electronic case notification to CDC by the next business day. IMMEDIATELY NOTIFIABLE, URGENT: Call the CDC EOC at 770.488.7100 Approved by CSTE: June 2019 within 24 hours of a case meeting the notification criteria, followed by Interim Update Approved by CSTE: April 5, 2020 submission of an electronic case notification in next regularly scheduled Implemented: January 1, 2020 electronic transmission. Updated: May 28, 2020 Condition Notification Timeliness Cases Requiring Notification Anthrax Immediately notifiable, Confirmed and probable cases - Source of infection not recognized extremely urgent - Recognized BT exposure/potential mass exposure - Serious illness of naturally-occurring anthrax Botulism Immediately notifiable, All cases prior to classification - Foodborne (except endemic to Alaska) extremely urgent - Intentional or suspected intentional release - Infant botulism (clusters or outbreaks) - Cases of unknown etiology/not meeting standard notification criteria Page 1 of 5 Plague Immediately notifiable, All cases prior to classification - Suspected intentional release extremely urgent Paralytic poliomyelitis -

Construção E Aplicação De Hmms De Perfil Para a Detecção E Classificação De Vírus
UNIVERSIDADE DE SÃO PAULO PROGRAMA INTERUNIDADES DE PÓS-GRADUAÇÃO EM BIOINFORMÁTICA Construção e Aplicação de HMMs de Perfil para a Detecção e Classificação de Vírus Miriã Nunes Guimarães SÃO PAULO 2019 Construção e Aplicação de HMMs de Perfil para a Detecção e Classificação de Vírus Miriã Nunes Guimarães Dissertação apresentada à Universidade de São Paulo, como parte das exigências do Programa de Pós-Graduação Interunidades em Bioinformática, para obtenção do título de Mestre em Ciências. Área de Concentração: Bioinformática Orientador: Prof. Dr. Arthur Gruber SÃO PAULO 2019 “Na vida, não existe nada a temer, mas a entender.” Marie Curie Agradecimentos Ao Professor Arthur Gruber pela oportunidade desde o início como estagiária no laboratório, pela orientação neste período de aprendizado no mestrado e por fornecer um ambiente de trabalho favorável. À aluna de doutorado Liliane Santana Oliveira que aguentou todas as minhas amolações diárias no laboratório pelo Hangouts, por dúvidas que eram erros meus em comandos de execução, pela paciência, pela amizade, pela companhia nos bandejões da faculdade com cardápio glutenfree que nem sempre eram tão bons assim. À aluna de mestrado Irina Yuri Kawashima que estava comigo no laboratório diariamente, pelas várias discussões sobre o mundo dos vírus e de conhecimentos da bioinformática, pelas ferramentas para facilitar o andamento do projeto, por todas guloseimas glutenfree que seria impossível eu não agradecer pois tenho ciência que não vou encontrar outra amiga masterchef assim. À Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) pelo financiamento durante estes 24 meses de mestrado. Aos meus pais pelo carinho e preocupação comigo durante estes 24 anos, pelo incentivo aos estudos e pelo apoio para eu me manter a uma distância de quase 400km de pura saudade. -

Presence of Dirofilaria Immitis in Mosquitoes in Southeastern Georgia
Georgia Southern University Digital Commons@Georgia Southern University Honors Program Theses 2019 Presence of Dirofilaria immitis in mosquitoes in Southeastern Georgia Angelica C. Tumminello Georgia Southern University Follow this and additional works at: https://digitalcommons.georgiasouthern.edu/honors-theses Part of the Laboratory and Basic Science Research Commons, Other Animal Sciences Commons, Parasitology Commons, Small or Companion Animal Medicine Commons, and the Veterinary Infectious Diseases Commons Recommended Citation Tumminello, Angelica C., "Presence of Dirofilaria immitis in mosquitoes in Southeastern Georgia" (2019). University Honors Program Theses. 495. https://digitalcommons.georgiasouthern.edu/honors-theses/495 This thesis (open access) is brought to you for free and open access by Digital Commons@Georgia Southern. It has been accepted for inclusion in University Honors Program Theses by an authorized administrator of Digital Commons@Georgia Southern. For more information, please contact [email protected]. Presence of Dirofilaria immitis in mosquitoes in Southeastern Georgia An Honors Thesis submitted in partial fulfillment of the requirements for Honors in the Department of Biology by Angelica C. Tumminello Under the mentorship of Dr. William Irby, PhD ABSTRACT Canine heartworm disease is caused by the filarial nematode Dirofilaria immitis, which is transmitted by at least 25 known species of mosquito vectors. This study sought to understand which species of mosquitoes are present in Bulloch County, Georgia, and which species are transmitting canine heartworm disease. This study also investigated whether particular canine demographics correlated with a greater risk of heartworm disease. Surveillance of mosquitoes was conducted in known heartworm-positive canine locations using traditional gravid trapping and vacuum sampling. Mosquito samples were frozen until deemed inactive, then identified by species and sex. -

August 2019 in St
Monthly Report AUGUST 2019 From the Director: The late summer month of August is the time of the year when South Loui- sianans are most at risk of infection from an arthropod-borne virus (arbovi- rus). Every year thousands of residents are bitten by mosquitoes infected with Eastern equine encephalitis virus (EEE), St. Louis encephalitis virus (SLE), and West Nile virus (WNV). All three endemic arboviruses in the region are primarily amplified by birds and transmitted by mosquitoes among birds, and incidentally to humans and other hosts. Fortunately, most of these infectious bites cause no or minor pathology and symptoms in humans. For the unfortunate minority, this trio of arboviral pathogens can be life-al- tering and life ending in some tragic cases. Eastern equine encephalitis virus (EEE) Eastern equine encephalitis virus is the rarest and most dangerous of the three arboviruses. Nearly a third of people that develop neurological symp- toms from EEE die from the infection. Culiseta melanura mosquitoes, a freshwater swamp species that primarily feeds on birds, are the primary Kevin A. Caillouet, Ph.D., M.S.P.H. vectors of EEE. Culiseta melanura are difficult to find in nature, as they rear Director their larvae in cryptic habitats in forested swamps. Adult Cs. melanura do not readily enter mosquito traps. Though most mosquitoes infected with EEE are Cs. melanura, occasionally other species may bite an infected bird and pose a more significant risk to humans. A single pool (or group) of EEE-infected Culex quinquefasciatus mosquitoes was collected from Fairview Riverside State Park on August 28th.