2019-06-20 EOCCO Board Meeting Minutes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2016 Recognition Targets for Hospitals
Patient Safety Reporting Program 2016 Recognition Targets for Hospitals March 2016 Recognition targets provide attainable goals for healthcare facilities participating in the Patient Safety Reporting Program (PSRP). Targets can also help facilities incrementally and effectively build adverse event review and reporting into their culture of safety. On a statewide level, targets ensure OPSC receives enough adverse event reports to build a strong database of prevention strategies so that all Oregon healthcare facilities can learn from one another. Targets are effective as of January 1, 2016. Although a participant may meet or exceed targets at any time throughout the year, the facility should continue to report adverse events according to reporting program guidelines. Healthcare facilities that meet targets are recognized annually for their transparency efforts and commitment to patient safety. For more information, visit oregonpatientsafety.org. Meet Targets Exceed Targets Quantity The number of reports submitted by a participating Submit at least the Submit at least the facility minimum quantity minimum quantity target for target for Goal: Help ensure PSRP obtains enough reports to your facility your facility build a strong database for learning. (see page 2) (see page 2) Acceptable Quality The report identifies contributing factors, root Submit at least 2 Submit 75% of causes, and system-level action plans reports that are reports with acceptable quality acceptable quality Goal: Provide enough information so that your experience can help others learn and improve. See the Guide to Quality Reporting Timeliness The amount of time that passes between discovery Submit 50% of reports of an adverse event and when a report is submitted within 45 days of to PSRP event discovery Goal: Respond immediately after an adverse event to collect full and reliable information, reduce delays, and develop strong solutions. -

Impact of Policies on Rural Communities Oregon
Impact of Policies on Rural Communities Oregon Sequestration2 Bad Debt Reimbursement Cut3 2% Inpatient and Outpatient Medicare Revenue Cut 35% Medicare Bad Debt Reimburesment Cut Provider Operating Annual Potential Job Potential GDP Annual Potential Job Potential GDP Provider Name/Number 1 Type Margin 1 Revenue Lost 1 Loss 4 Loss 5 Revenue Lost Loss 4 Loss 5 Bay Area Hospital (380090) RPPS 5.1% $1,402,674 21 $2,694,287 $335,951 5 $645,302 Blue Mountain Hospital (381305) CAH 12.4% $103,038 2 $230,097 $22,265 0 $49,721 CHI St. Anthony Hospital (381319) CAH 14.1% $295,649 4 $570,912 $62,980 1 $121,616 Columbia Memorial Hospital (381320) CAH 13.3% $536,031 9 $1,188,408 $312,917 5 $693,753 Coquille Valley Hospital (381312) CAH -1.0% $221,858 3 $409,956 $18,291 0 $33,799 Curry General Hospital (381322) CAH -0.2% $285,231 5 $630,182 $100,353 2 $221,718 Good Shepherd Health Care System (381325) CAH 4.5% $425,575 7 $923,659 $62,123 1 $134,829 Grande Ronde Hospital (381321) CAH 3.6% $445,021 7 $879,693 $167,414 3 $330,936 Harney District Hospital (381307) CAH -1.8% $103,560 2 $240,129 $17,862 0 $41,417 Lake District Hospital (381309) CAH 0.3% $120,338 3 $338,664 $11,533 0 $32,456 Lower Umpqua Hospital District (381311) CAH -5.8% $121,920 2 $285,842 $68,875 1 $161,478 Mercy Medical Center (380027) RPPS 16.5% $1,187,722 20 $2,610,228 $101,817 2 $223,760 Mid-Columbia Medical Center (380001) RPPS 3.2% $477,045 9 $1,109,291 $139,303 3 $323,927 PeaceHealth Cottage Grove Community Medical Center CAH 19.4% $237,056 4 $483,247 $87,272 1 $177,907 (381301) 1 CMS Healthcare Cost Report Information System (HCRIS) Q1 2020. -

Beacon Name Changing to Affinity
September 30, 2016 Dear Provider, A few months ago we sent you some information and an attestation of acknowledgement that the Beacon network name will be changing to the Affinity network for the 2017 plan year. With 2017 open enrollment beginning in November, we want to make sure you are aware of changes to Moda’s Beacon Network, which is available to individuals purchasing health coverage directly from Moda or through the federal marketplace exchange. For plans effective January 1, 2017, the Beacon Network name in your area will change to the Affinity Network. The Beacon Network will continue to serve members in select Western Oregon counties. The Affinity Network will be available to individual members residing in the following counties: Baker Morrow Gilliam Sherman Grant Umatilla Harney Union Lake Wallowa Malheur Wheeler Affinity is designed to ensure members find the care they need, when they need it, Affinity helps members looking for customized care that fits their individual lifestyle and budget, and find the care they need, when they need it. With Affinity, members have access to a large selection of providers including Blue Mountain Hospital District, Good Shepherd, Grande Ronde Hospital, Harney District Hospital, Lake District Hospital, Pioneer Memorial Hospital (Heppner), St. Alphonsus Baker City, St. Alphonsus Ontario, and Wallowa Memorial Hospital. Although the Affinity name is new, we don’t expect any changes to your current workflow. Reimbursement, referrals to in-network providers, prior authorizations and processes will be the same. Individuals choosing plans supported by the Affinity network will be asked to select a primary care physician (PCP) to coordinate care. -

Umatilla &Morrow
Safe Kids Oregon 2012 State Report Dear Child Safety Advocates, Injury prevention efforts continue to make a difference to Oregon’s children. Between 2005-2007 and 2009-2011 deaths to children ages 0 – 14 from unintentional injuries decreased by 18.9% (from 148 to 120) and hospitalizations decreased by 17.3% (from 3,539 to 3,214). The important injury prevention messages and events hosted by Safe Kids Coalitions and partners throughout communities in 2012 continue to help families make safe INSIDE THIS REPORT: choices. This report details the extensive work of Safe Kids Oregon and the eight coalitions and three chapters in Introduction 1-3 Oregon. Please take a moment to read about our efforts. Prevention Activity Statewide 4-6 2012 was a year of transition for Safe Kids Oregon. I wish Motor Vehicle Occupant Safety to thank Adrienne Greene for her support as she moved Pedestrian Safety into her role as CDC Grant Manager and Tam Peterson for Bicycle and Wheeled Sports Safety her valuable training in website maintenance and Suffocation Prevention and Safe newsletter design. Additionally, the Safe Kids Oregon Sleep Advisory Board has been very active and involved in Fire and Burn Prevention providing guidance to Safe Kids Oregon. Fall Prevention Water Safety Sports Safety Ruth Harshfield Safe Kids Oregon Director Chapters & Coalitions 7 - 18 Safe Kids Oregon Safe Kids Central Oregon Safe Kids Columbia County Safe Kid Columbia Gorge Safe Kids Harney County Safe Kids Malheur County A MESSAGE FROM Safe Kids Portland Metro Safe Kids Rogue Valley KAREN GUNSON, MD ~ Safe Kids Umatilla/Morrow Counties HONORARY CHAIR Safe Kids Union County Safe Kids Washington County The work of Safe Kids Oregon continues to be important. -
157 Entities in LIVE Status EHR/PDMP
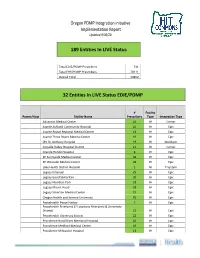
Oregon PDMP Integration initiative Implementation Report Updated 9/30/20 189 Entities In LIVE Status Total EDIE/PDMP Prescribers 741 Total EHR/PDMP Prescribers 20111 Overall Total 20852 32 Entities In LIVE Status EDIE/PDMP # Facility Parent/Host Facility Name Prescribers Type Integration Type Adventist Medical Center 26 IH Cerner Asante Ashland Community Hospital 10 IH Epic Asante Rogue Regional Medical Center 41 IH Epic Asante Three Rivers Medical Center 19 IH Epic CHI St. Anthony Hospital 19 IH Meditech Coquille Valley Hospital District 12 IH Cerner Grande Ronde Hospital 8 IH Epic KP Sunnyside Medical Center 36 IH Epic KP Westside Medical Center 36 IH Epic Lake Health District Hospital 5 IH T-System Legacy Emanuel 25 IH Epic Legacy Good Samaritan 30 IH Epic Legacy Meridian Park 18 IH Epic Legacy Mount Hood 28 IH Epic Legacy Silverton Medical Center 15 IH Epic Oregon Health and Science University 70 IH Epic Peacehealth Peace Harbor 7 IH Epic Peacehealth Riverbend (2 Locations Riverbend & University District) 22 IH Epic Peacehealth University District 22 IH Epic Providence Hood River Memorial Hospital 10 IH Epic Providence Medford Medical Center 19 IH Epic Providence Milwaukie Hospital 13 IH Epic # Facility Parent/Host Facility Name Prescribers Type Integration Type Providence Newberg Hospital 26 IH Epic Providence Portland Medical Center 43 IH Epic Providence Seaside Hospital 7 IH Epic Providence St Vincent Medical Center 47 IH Epic Providence Willamette Falls Medical Center 12 IH Epic Salem Hospital 42 IH Epic Sky Lakes Medical Center -

Hospital Presumptive Medical -- Authorized Sites 1-Nov-14
Hospital Presumptive Medical -- Authorized Sites 1-Nov-14 Hospital Identification Number Contact Email Phone Adventist Medical Center Portland 1801887658 Donna Krenzler [email protected] 503.251.6153 Asante Tonya Richner [email protected] 541-789-5208 Asante Ashland Community Hospital 1386644029; 136114 Asante Three Rivers Medical Center 1801891809; 022560 Asante Rogue Regional Medical Center 1770587107; 162008 Blue Mountain Hospital District 1356414395 Barb Oliver [email protected] 541-575-4153 Good Shepherd Medical Center 1295789667 Jonathan Edwards [email protected] 541-667-3438 Grande Ronde Hospital 1407446195; 067801 KARLI WRIGHT [email protected] 541-963-1555 Kaiser Permanente Northwest 1124182902 Melissa Inskeep [email protected] 503 813 4111 Lake Health District 1376698522 Brian McCarthy [email protected] 541-947-7290 Legacy System Terrie Handy [email protected] Melody Jackson [email protected] Kim Carter [email protected] Legacy Emanuel 1831112358 Legacy Good Samaritan 1780608216 Legacy Meridian Park 1184647620 Legacy Mt. Hood 1255354700 Legacy Randall Children's Hospital at Legacy Emanuel 1831112358 Legacy Salmon Creek 1700809829 Lower Umpqua Hospital 1003874819; 000054; 286986 Mark Sayler [email protected] 541-271-2171 x395 Mercy Medical Center 1477590198 John Kasberger Kasberger [email protected] Luke Martin [email protected] 303-513-2502 Laurie Jones [email protected] 541-677-2461 OHSU Hospital 1609824010 Kippi Coffey [email protected] 503-494-6664 PeaceHealth -
ROR) + Library Partnership
WLA/OLA 2019 – Charting the Unknown Together Healthcare Providers & Libraries Collaborating to Support Families How to start a Reach Out and Read (ROR) + Library Partnership Step 1: Check with your librarians, early learning staff, and Youth Services/Community Managers to see if relationships already exist. Talk internally to see what type/level of partnership might make sense. Step 2: Find out if a ROR clinic exists near you! Washington https://reachoutandreadwa.org/ - 206.524.3579 - [email protected] Oregon: http://reachoutandread.org/oregon/ - 503-830-0510 - [email protected] Find a program near you: http://www.reachoutandread.org/resource-center/find-a-program/ For large scale partnerships, identify the best person at your library to reach out to the ROR director for your state. For local, clinic-to-branch level connections, ROR staff can help with making an initial introduction. In some cases, there may be value in setting up an in-person meeting with ROR, the clinic, and the library. In others, an email introduction may be ideal. Step 3: Get to know your clinic! Set up a phone or in-person meeting. Here are some questions you might ask: I am interested in knowing more about the communities you serve at your clinic. Do you serve low income families or families from specific cultural groups? What languages are spoken as a first language by your clients? What community resources do you frequently refer families to? Do you have any questions for me about what resources are available at the library? WLA/OLA -
Weekly Data Report - August 11, 2021 Table of Contents Background
COVID-19 Weekly Report Oregon’s Weekly Surveillance Summary Novel Coronavirus (COVID-19) Weekly Data Report - August 11, 2021 Table of Contents Background ........................................................................................................................................... 3 Weekly Report Summary ..................................................................................................................... 4 Clinical Characteristics and risk factors ............................................................................................... 4 Epidemiologic links ........................................................................................................................... 4 Figure 1. Epidemiologic link of recent COVID-19 cases by week of onset ............................... 6 Figure 2. Epidemiologic link of all COVID-19 cases by week of onset ...................................... 7 Figure 3. Recent sporadic COVID-19 cases by race and week of onset .................................... 8 Figure 4. All sporadic COVD-19 cases by race and week of onset ............................................ 9 Figure 5. Recent sporadic COVID-19 cases by ethnicity and week of onset .......................... 10 Figure 6. All sporadic COVID-19 cases by ethnicity and week of onset .................................. 11 Clinical symptoms and reported risk factors ................................................................................ 11 Figure 7. Reported signs and symptoms for all COVID-19 cases ........................................... -

OAMSS Membership Roster4.Xlsx
OREGON ASSOCIATION MEDICAL STAFF SERVICES MAILING LIST & MEMBERSHIP DUES PAID - 2020 2020 Officers 2020 Volunteers Current Membership Totals: President Hillary Parks Web Master Vacant Category By Year President Elect Tamara Nesbitt Newsletter Editor Hillary Parks Active 127 2020 140 Past President Kelly Aebi Scholarship Chair Ann Klinger, CPCS Affiliate 12 2019 114 Secretary Ann Klinger, CPCS Librarian Cheryl Butler, CPCS Student 1 2018 105 Treasurer Amanda Walker, CPCS P&P Committee Vacant Honorary 0 2017 146 Membership Chair Megan Veliquette, CPCS Chair Certifications 2016 145 CPCS 23 2015 137 CPMSM 6 2014 127 Dual Certified 10 Name Facility Phone #s E-Mail Org Type Category 2020 Dues paid Aebi, Kelly Salem Hospital 503/814-3889 [email protected] Hosp Active Manager PO Box 14001 503/814-3898 (FAX) Salem, OR 97309 Antle, Jennifer Lake District Hospital 541/947-7284 [email protected] Hosp Active x Executive Assistant to CEO 700 S J St 541/947-2433 (FAX) Lakeview, OR 97630 Asay, Leah, CPCS, CPMSM 844 Pool St Ste 48 541/915-8670 [email protected] MCO Active Credentialing Specialist Eugene, OR 97401 Avila, Lisa Sky Lakes Medical Center 541/274-6152 [email protected] Hosp Active x Director, Medical Staff Services 2865 Daggett Ave 541/274-6725 (FAX) Klamath Falls, OR 97601 Barry, Julie, CPCS The Vancouver Clinic 360/397-3352 [email protected] Phys Grp Active Credentialing Coordinator 700 NE 87th Ave 360/604-1771 (FAX) Vancouver, WA 98687 Benson, Cheryl, CPCS The Oregon Clinic 503/963-2846 [email protected] Phys Grp -

Oregon 350 Winter St
Department of Consumer and Business Services Workers’ Compensation Division Oregon 350 Winter St. NE John A. Kitzhaber, MD, Governor P.O. Box 14480 Salem, OR 97309-0405 1-800-452-0288, 503-947-7810 www.wcd.oregon.gov BULLETIN NO. 290 (Revised) March 7, 2013 TO: Workers’ compensation insurers and Oregon hospitals SUBJECT: Hospital fee schedule — adjusted cost/charge ratios for Oregon hospitals This bulletin provides updated adjusted cost/charge ratios. Apply these ratios to hospital inpatient and outpatient services according to ORS 656.248 and OAR 436-009-0020. This bulletin replaces Bulletin 290 issued Sept. 19, 2012. The following are adjusted cost/charge ratios for the Oregon hospitals: Adjusted Adjusted Adjusted Adjusted cost/charge cost/charge cost/charge cost/charge Hospital name ratio ratio ratio ratio 4/1/13 – Notes 10/1/12 – Notes 4/1/12 - Notes 10/1/11 - Notes 9/30/2013 3/31/2013 9/30/2012 3/31/2012 Adventist Medical Center *Adventist Health System/West 0.405 0.411 0.452 0.456 Formerly Portland Adventist Ashland Community Healthcare 1.000 1 1.000 1 1.000 1 0.544 Services Bay Area Hospital 0.445 0.470 0.470 0.463 *Bay Area Health District Blue Mountain Hospital District 1.000 1 1.000 1 1.000 1 1.000 1 (CAH) Columbia Memorial Hospital (CAH) 1.000 1 1.000 1 1.000 1 1.000 1 Coquille Valley Hospital (CAH) 1.000 1 1.000 1 1.000 1 1.000 1 Cottage Grove Community Hospital (CAH) 1.000 1 1.000 1 1.000 1 1.000 1 *PeaceHealth Curry General Hospital (CAH) 1.000 1 1.000 1 1.000 1 1.000 1 *Curry Health District Good Samaritan Regional Medical Center *Samaritan Health Services, Inc. -

Oregon's Rural Landscape
Oregon’s Rural Landscape Oregon’s 32 small and rural hospitals provide essential health care services to more than one million Oregonians. These hospitals are the cornerstones within the communities they serve. For most communities, they are the largest employer, offering family-wage jobs. What is the Critical Access Hospital Program? (Medicare Reimbursement) Twenty-five of Oregon’s 32 rural hospitals are Critical Access Hospitals (CAH), which is a federal program designed to improve rural health care access and reduce hospital closures. For its Medicare patients, CAHs receive cost- based reimbursement. As the name implies, cost-based reimbursement pays hospitals to cover the maximum allowable cost assumed by the hospital. Oregon’s rural hospitals have long depended on cost-based reimbursement from Medicaid and Medicare to remain viable. Prior to the CAH program and cost-based reimbursement, several rural hospitals around the country shut their doors as a result of poor reimbursement levels. What are A & B Designations? (Medicaid Reimbursement) Oregon’s rural hospitals also have a state designation based on their size and location. Similar to Medicare for CAHs, the state designation of Type A or B provides Medicaid reimbursement up to 100% of cost. These rural designations significantly improve the bottom line for many fragile community hospitals. Many rural hospitals lack the operating margins needed to access capital funding to replace or update facilities and purchase necessary health information technology or upgrades. Along with tackling financial challenges, small and rural hospitals must sustain a highly trained work force, including medical providers. Even with strong recruitment efforts, rural hospitals have difficulty attracting and retaining skilled workers. -
November 19, 2018
Q3 2018 HOSPITAL UTILIZATION AND FINANCIAL ANALYSIS November 19, 2018 4000 Kruse Way Place • Suite 100 • Lake Oswego, OR 97035 • Tel: (503) 479-6034 • www.apprisehealthinsights.com APPRISE HEALTH INSIGHTS IS A SUBSIDIARY OF THE OREGON ASSOCIATION OF HOSPITALS AND HEALTH SYSTEMS © 2018 Apprise Health Insights Q3 2018 HOSPITAL UTILIZATION AND FINANCIAL ANALYSIS ABOUT THIS REPORT This report aims to provide a quarterly analysis of the utilization and financial data submitted by Oregon’s hospitals to the DATABANK program. DATABANK is a state-mandated monthly hospital data program administered by Apprise Health Insights in collaboration with the Office for Oregon Health Policy and Research (OHPR). Please note that all DATABANK data are self-reported by the hospital and represent a twelve-month calendar year. Accuracy is the responsibility of the reporting hospitals. Because this report’s objective is to provide a complex dive into the data, the graphs and methods may change between reports. This forces only the most compelling stories to be exhibited. The determination of which graphs and stories to focus on is evaluated by hospital finance and data experts at Apprise. Note: Kaiser Sunnyside and Kaiser Westside hospitals are excluded from this analysis due to the lack of financial data available in DATABANK. LAYOUT INFORMATION Aggregate vs Median This report uses two statistics to report statewide hospital data: median and aggregate. Aggregate numbers sum up the entire amount for all hospitals into one number, where median only takes the number from the middle of the pack. Aggregate is useful when looking at the industry as a whole, such as the percent of Medicaid charges or the total number of patients visiting Emergency Departments in the state.