Fundamentals of Anesthesiology for Spaceflight
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Space Resources : Social Concerns / Editors, Mary Fae Mckay, David S
Frontispiece Advanced Lunar Base In this panorama of an advanced lunar base, the main habitation modules in the background to the right are shown being covered by lunar soil for radiation protection. The modules on the far right are reactors in which lunar soil is being processed to provide oxygen. Each reactor is heated by a solar mirror. The vehicle near them is collecting liquid oxygen from the reactor complex and will transport it to the launch pad in the background, where a tanker is just lifting off. The mining pits are shown just behind the foreground figure on the left. The geologists in the foreground are looking for richer ores to mine. Artist: Dennis Davidson NASA SP-509, vol. 4 Space Resources Social Concerns Editors Mary Fae McKay, David S. McKay, and Michael B. Duke Lyndon B. Johnson Space Center Houston, Texas 1992 National Aeronautics and Space Administration Scientific and Technical Information Program Washington, DC 1992 For sale by the U.S. Government Printing Office Superintendent of Documents, Mail Stop: SSOP, Washington, DC 20402-9328 ISBN 0-16-038062-6 Technical papers derived from a NASA-ASEE summer study held at the California Space Institute in 1984. Library of Congress Cataloging-in-Publication Data Space resources : social concerns / editors, Mary Fae McKay, David S. McKay, and Michael B. Duke. xii, 302 p. : ill. ; 28 cm.—(NASA SP ; 509 : vol. 4) 1. Outer space—Exploration—United States. 2. Natural resources. 3. Space industrialization—United States. I. McKay, Mary Fae. II. McKay, David S. III. Duke, Michael B. IV. United States. -

Space Day Teacher's Resource Guide
Space Day Teacher’s Resource Guide Thank you for participating in Science Museum Oklahoma’s Space Day 2019! We compiled this resource guide to help enrich your students’ experience beyond the museum. It includes thought- provoking talking points to encourage group discussions and extension activities that promote critical thinking skills. Talking Points • At one of the day’s activities you constructed and launched water rockets using compressed air and water. Discuss the variables that could be altered in order to make the rocket travel higher. What factors affected the flight of the rocket? How are these similar to factors that affect the launch of full-scale rockets, satellites, and other orbital objects? • Discuss the various types of preparations and training potential astronauts had to undergo, both physical and psychological, before being selected for missions. • In 1969, hundreds of millions of people eagerly watched the Moon landing on television. Why do you think so many were interested? Have people’s feelings about space travel changed over 50 years? If so, how? • The Apollo 11 mission was dangerous, with no guarantee that the astronauts would return safely. If you were a family member or friend of the astronauts in 1960s, would you have encouraged them to be a part of Apollo 11? • Put yourself into the shoes of one of those astronauts. Would you put your life at risk for something that could benefit others? Is it worth the risk in order to gain understanding of the unknown? • With the advancements we’ve had in technology and science, how do you think a mission to the Moon might be different today? • Astronauts often comment that their experiences impacted the way they view our place in the universe. -

What the Dogs Did: Animal Agency in the Soviet Manned Space Flight
BJHS: Themes 2:79–99, 2017. © British Society for the History of Science 2017. This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http:// creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited. doi:10.1017/bjt.2017.9 What the dogs did: animal agency in the Soviet manned space flight programme AMY NELSON* Abstract. This paper examines the agency of the dogs used to develop the Soviet manned space flight programme by considering what the dogs did as experimental subjects, as dog technolo- gies, and as individual dogs in the context of the historically conditioned practices of Soviet science. Looking at how Soviet space researchers refined Pavlovian behaviourism and inte- grated it into a complex engineering project helps clarify the conditions under which the dogs worked and the assumptions that guided the human researchers. The paper uses theoret- ical perspectives that contextualize animal agency in terms of relationships and then looks at those relationships from an ethological perspective. This provides a sense of what the dogs did that distinguishes between how humans understand dogs and what we know about dogs’ cognitive and social capacities. The paper proposes a model of animal agency that looks seriously at the dogs’ relationships with human researchers and suggests that the dogs’ significance as historical subjects depends as much on what they did as dogs as it does on how their contributions to the space race were perceived. Among the legions of animals used in scientific research few have garnered the fame of the Soviet space dogs. -
Year 5 History Week Beginning 4Th May L.O.: I Can Learn
YEAR 5 HISTORY WEEK BEGINNING 4TH MAY L.O.: I CAN LEARN ABOUT ANIMALS IN SPACE AND DEBATE WHETHER THIS IS ACCEPTABLE. As we learnt last week, there was a great Space Race between USA and USSR. Both wanted to be the best at Space travel and exploration! We learnt about the humans who went in to Space, but animals have played a very important part too… Both countries were using experimental technology that was extremely dangerous and a lot was at stake. Whoever got there first, without casualties, would be the better country - and the whole world was watching. In the 1940s and 50s, Space flight was still too dangerous to risk an astronaut’s life… so animals were sent instead. The USA sent fruit flies into space in 1947 so they were technically the first animals in space. In 1949 however, a rhesus monkeys called Albert 1 reached 30– 39 miles (48–63 km) altitude (height above Earth). Another monkey, Albert II, reached about 83 miles (134 km) on a different space mission. Albert II died on impact after a parachute failure. The USSR decided to send the spacecraft 'Sputnik' into space with a stray dog called Laika as it's passenger. By using a dog, their scientists could see the effects of zero-gravity on a living animal. They believed that if the mission was unsuccessful, then the loss of a dog's life wouldn't be as bad as a lost human. On November 3rd 1957, Sputnik 2 was launched into space with Laika. She had gone from being a stray dog in Moscow to being an animal astronaut pioneer. -

Environmental Enrichment in the ISS Rodent Habitat Hardware System
Environmental Enrichment in the ISS Rodent Habitat Hardware System Sophie Orr1, Rhonda Weigand2, Tanner Adams2, Raycho Raychev3 & Yuri Griko4 1 University of North Dakota, Grand Forks, ND, USA 2 Redlands Community College, El Reno, OK, USA 3 Space Challenges Program, EnduroSat Inc. Sofia, Bulgaria 4 Division of Space Biosciences, NASA Ames Research Center, Moffett Field, CA, USA *Corresponding author: Space Biosciences Division, NASA Ames Research Center, MS261-3, Moffett Field, CA 94035, USA. Tel: +1 650-604-0519; fax: +1 650-604-0046 Email: [email protected] (Y.V. Griko). ABSTRACT Responses of animals exposed to microgravity during in-space experiments were observed via available video recording stored in the NASA Ames Life Sciences Data Archive. These documented observations of animal behavior, as well as the range and level of activities during spaceflight, demonstrate that weightlessness conditions and the extreme novelty of the surroundings may exert damaging psychological stresses on the inhabitants. In response to a recognized need for in-flight animals to improve their wellbeing we propose to reduce such stresses by shaping and interrelating structures and surroundings to satisfying vital physiological needs of inhabitants. A Rodent Habitat Hardware System (RHHS) based housing facility incorporating a tubing network system, to maintain and monitor rodent health environment with advanced accessories has been proposed. Placing mice in a tubing-configured environment creates more natural space-restricted nesting environment for rodents, thereby facilitating a more comfortable transition to living in microgravity. A sectional tubing structure of the RHHS environment will be more beneficial under microgravity conditions than the provision of a larger space area that is currently utilized. -

Animal Models in Space Research
Animal models in space research Merel Van Walleghem [email protected] Copyright © 2014 1 SCK•CEN Spaceflight history Preparation for human spaceflight Is the space environment suitable for human presence? Copyright © 2014 2 SCK•CEN Spaceflight history Preparation for human spaceflight 1783 st Is the1 passengersspace environment in a hot air balloon suitable: duck, for rooster human & sheep presence? All 3 animals survived the flight Humans followed experienced the symptoms of hypoxia Copyright © 2014 3 SCK•CEN Spaceflight history Preparation for human spaceflight 1950’s Is the Decision space environmentmade to explore suitable space for human presence? Extensive animal experimentation in both US and Soviet/Russian space programs in order to Test the country’s ability to launch a living organism into space and bring it back alive and unharmed Collect medical information and test the concepts used to place humans in space Copyright © 2014 4 SCK•CEN Animals in space Suborbital flights: V2 rocket 1946 First animals intentionally sent into space Fruit flies Explore effects of radiation exposure at high altitudes Copyright © 2014 5 SCK•CEN Animals in space Suborbital flights: V2 rocket 1948-1949 Albert I - IV Anaesthesized monkeys Monitoring vital functions during flight I died before launch because of breathing difficulties II, III & IV survived the flight but died due to parachute recovery system failure Copyright © 2014 6 SCK•CEN Animals in space Suborbital flights: V2 rocket 1950 Mouse Photographed in flight but did not survive -

The History of the Animal Care Program at NASA Johnson Space
The Animal Care Program • Johnson Space Center is committed to the ethical and humane care and use of animals and each person must share responsibility in meeting that commitment. • Our role in the care and use of animals carries the responsibility to effectively meet the needs of the animals in our charge while actively seeking and employing methods that embody respect for the life of animals. - JSC Animal Care & Use Handbook, JSC29259 STS-3 Insect Flight Motion Study December 1959 Wallops Island, VA Rhesus Monkey “SAM” MDS – Mice Drawer System • Study bone loss – long duration • ACP provided training on animal handling and euthanasia • 100- 150 days housing Actual Animals in Space… Before humans actually went into space, one of the prevailing theories of the perils of space flight was that humans might not be able to survive long periods of weightlessness. American and Russian scientists utilized animals - mainly monkeys, chimps and dogs - in order to test each country's ability to launch a living animal into space and bring it back alive and unharmed. Dog: Laika in Sputnik II Scientists want to know how the body reacts to microgravity. Many experiments can be conducted on humans while they work aboard the Space Shuttle or International Space Station (ISS), but many others interfere with daily activities; that's where the animals come into play. And while scientists may not really care how a rat reacts to space conditions, animal data can Chimpanzee: Enose transfer to human models and help prevent or Mercury Atlas 5 solve physical issues people face today. Animals go into space to help conduct scientific research only when absolutely necessary. -

Space Activity Book
Elliot and Friends Space Activity Book written by jeffrey ault and elliot illustrated by debi mcnabb Elliot and Friends Space Activity Book This activity book belongs to ________________________________________ written by Jeffrey Ault and Elliot illustrated by Debi McNabb copyright 2008, 2020 Elliot and Friends, Inc. All rights reserved under International and Pan-American Copyright Conventions. Published in the United States by Elliot Publishing, an imprint of Elliot and Friends, Inc., Florida. 1 Hi! My name is Elliot. I’m a cute floppy eared dog who can fly! Cool, huh?! My friends and I travel through portals in my backyard to go on exciting adventures around the world, to space and under the sea. We have lots of fun while learning about nature, animals, science, art, history and all sorts of interesting things. Today we are learning about Space and America’s Space program. So come join our adventures. It’s time for fun! Your friend, 2 America’s Space Program 1958 - 2011 In 1958 the United States formed NASA, the National Aeronautics and Space Administration, to lead the peaceful exploration of space. Kennedy Space Center, Florida is the home of America’s Space program. It is named after President John F. Kennedy and is nicknamed, “America’s Gateway to Space.” Kennedy Space Center is the main launch and landing site for space flights. It is one of the places where NASA trains astronauts. Astronauts are men and women who fly into space. Some of the first space missions launched from Kennedy Space Center were called Mercury missions. Mercury missions allowed one astronaut at a time to lift-off in rockets and reach space. -

The Nonhuman Autonomous Space Agency
The Nonhuman Autonomous Space Agency In the summer of 2011, the last Space Shuttle launch took place at Cape Canaveral, Florida. When the Shuttle landed 13 days later, the United States, for the first time in 30 years, no longer operated a vehicle capable of carrying humans into Low Earth Orbit. FRED SCHARMEN A few miles from Cape Canaveral, in places like Blue Springs State Park, Florida’s Morgan State University endangered population of manatees takes shelter in the warm spring water that rises through the state’s porous limestone geology. Manatees are famous for their somewhat goofy hybridity, which according to stories led some sailors to mistake them for the half human, half fish mermaids of legend. Like the Space Shuttle, itself a hybrid compromise between budgetary, political, and per- formance constraints, manatees become surprisingly graceful when they are embedded and active in the their environment. In ecological science, biologists talk about the concept of the ‘charismatic megafauna’1, a species of animal that is well known and well liked, which serves as a stand-in and focal point for the complexities of the ecosystem in which it lives. Polar bears serve as a good start- ing point for discussions about the effects of climate change. Talking about mana- tees is a way to begin to talk about how we use the landscape of Florida and the Caribbean recreationally, and how to possibly change some careless habits asso- ciated with that use. MASCOTS AND MEGAFAUNA With the absence of the Space Shuttle as a recognizable icon, the whole enter- prise of space exploration now has a unique problem, it no longer has a mascot. -

The Space Shuttle Brought a New Dimension to the Study of Biology in Space
The Space The Space Shuttle brought a new dimension to the study of biology in space. Prior to the shuttle, scientists relied primarily on uncrewed robotic spacecraft Shuttle: to investigate the risks associated with venturing into the space environment. A Platform Various biological species were flown because they were accepted as models with which to study human disease and evaluate human hazards. The results That Expanded from the pioneering biological experiments aboard uncrewed robotic spacecraft the Frontiers not only provided confidence that humans could indeed endure the rigors of spaceflight, they also formed the foundation on which to develop risk mitigation of Biology procedures; i.e., countermeasures to the maladaptive physiological changes the human body makes to reduced gravity levels. For example, the musculoskeletal Kenneth Souza system reacts by losing mass. This may pose no hazard in space; however, on returning to Earth after long spaceflights, such a reaction could result in an increased risk of bone fractures and serious muscle atrophy. Unfortunately, most biological research in uncrewed spacecrafts was limited to data that could only be acquired before and/or after spaceflight. With crew support of the experiments aboard the Space Shuttle and Spacelab, and with adequate animal housing and lab support equipment, scientists could train the crew to obtain multiple biospecimens during a flight, thus providing windows into the adaptation to microgravity and, for comparison, to samples obtained during readaptation to normal terrestrial conditions postflight. With the Space Shuttle and its crews, earthbound scientists had surrogates in orbit —surrogates who could be their eyes and hands within a unique laboratory. -
Rodent Research Hardware System Studying Animals in Space Aboard the International Space Station
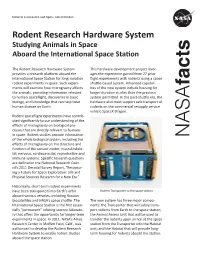
National Aeronautics and Space Administration Rodent Research Hardware System Studying Animals in Space Aboard the International Space Station The Rodent Research Hardware System This hardware development project lever- provides a research platform aboard the ages the experience gained from 27 prior International Space Station for long-duration flight experiments with rodents using a space rodent experiments in space. Such experi- shuttle-based system. Advanced capabili- facts ments will examine how microgravity affects ties of the new system include housing for the animals, providing information relevant longer duration studies than the previous to human spaceflight, discoveries in basic system permitted. In the post-shuttle era, the biology, and knowledge that can help treat hardware also must support safe transport of human disease on Earth. rodents on the commercial resupply service vehicle SpaceX Dragon. Rodent spaceflight experiments have contrib- uted significantly to our understanding of the effects of microgravity on biological pro- cesses that are directly relevant to humans in space. Rodent studies provide information NASA of the whole biological system, including the effects of microgravity on the structure and function of the sensori-motor, musculoskele- tal, nervous, cardiovascular, reproductive and immune systems. Specific research questions are defined in the National Research Coun- cil’s 2011 Decadal Survey Report, “Recaptur- ing a Future for Space Exploration: Life and Physical Sciences Research for a New Era.” Historically, -

Animals in Space: from Research Rockets to the Space Shuttle (Springer Praxis)
Animals in Space From Research Rockets to the Space Shuttle Colin Burgess and Chris Dubbs Animals in Space From Research Rockets to the Space Shuttle Published in association with PPraxisraxis PPublishiublishingng Chichester, UK Mr Colin Burgess, BIS Bonnet Bay New South Wales Australia Mr Chris Dubbs Edinboro Pennsylvania USA SPRINGER±PRAXIS BOOKS IN SPACE EXPLORATION SUBJECT ADVISORY EDITOR: John Mason, M.Sc., B.Sc., Ph.D. ISBN 10: 0-387-36053-0 Springer Berlin Heidelberg New York Springer is part of Springer-Science + Business Media (springer.com) Library of Congress Control Number: 2006937358 Apart from any fair dealing for the purposes of research or private study, or criticism or review, as permitted under the Copyright, Designs and Patents Act 1988, this publication may only be reproduced, stored or transmitted, in any form or by any means, with the prior permission in writing of the publishers, or in the case of reprographic reproduction in accordance with the terms of licences issued by the Copyright Licensing Agency. Enquiries concerning reproduction outside those terms should be sent to the publishers. # Praxis Publishing Ltd, Chichester, UK, 2007 Printed in Germany The use of general descriptive names, registered names, trademarks, etc. in this publication does not imply, even in the absence of a speci®c statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. Cover design: Jim Wilkie Project management: Originator Publishing Services, Gt Yarmouth, Norfolk, UK Printed on acid-free paper Contents Authors' preface ....................................... xvii Acknowledgements...................................... xxiii Foreword............................................ xxv List of ®gures ........................................ xxxi List of abbreviations and acronyms ...........................xxxvii Prologue ...........................................