Russian Mortality Beyond Vital Statistics. Effects of Social Status and Behaviours on Deaths from Circulatory Disease and Extern
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Russian Peasant Letters
Slavistische Studienbücher. Neue Folge 18 Russian Peasant Letters Texts and Contexts Bearbeitet von Olga T Yokoyama 1. Auflage 2008. Buch. VII, 973 S. Hardcover ISBN 978 3 447 05653 3 Format (B x L): 17 x 24 cm Weitere Fachgebiete > Literatur, Sprache > Sprachwissenschaften Allgemein Zu Inhaltsverzeichnis schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. Olga T. Yokoyama Russian Peasant Letters Texts and Contexts Part 1 and 2 2008 Harrassowitz Verlag · Wiesbaden ISSN 05835445 ISBN 978-3-447-05653-3 CONTENTS OF VOLUME I Acknowledgements ............................................................................................ vii Introduction ........................................................................................................ 1 Guide for the reader ............................................................................................ 9 Chronology of letters and events ........................................................................ 15 Chapter one: Transcribed letter texts .................................................................. 27 Chapter two: Essay A Linguistic features of the texts ................................................................ -

Politics, Feasts, Festivals SZEGEDI VALLÁSI NÉPRAJZI KÖNYVTÁR BIBLIOTHECA RELIGIONIS POPULARIS SZEGEDIENSIS 36
POLITICS, FEASTS, FESTIVALS SZEGEDI VALLÁSI NÉPRAJZI KÖNYVTÁR BIBLIOTHECA RELIGIONIS POPULARIS SZEGEDIENSIS 36. SZERKESZTI/REDIGIT: BARNA, GÁBOR MTA-SZTE RESEARCH GROUP FOR THE STUDY OF RELIGIOUS CULTURE A VALLÁSI KULTÚRAKUTATÁS KÖNYVEI 4. YEARBOOK OF THE SIEF WORKING GROUP ON THE RITUAL YEAR 9. MTA-SZTEMTA-SZTE VALLÁSIRESEARCH GROUP KULTÚRAKUTATÓ FOR THE STUDY OF RELIGIOUS CSOPORT CULTURE POLITICS, FEASTS, FESTIVALS YEARBOOK OF THE SIEF WORKING GROUP ON THE RITUAL YEAR Edited by Gábor BARNA and István POVEDÁK Department of Ethnology and Cultural Anthropology Szeged, 2014 Published with the support of the Hungarian National Research Fund (OTKA) Grant Nk 81502 in co-operation with the MTA-SZTE Research Group for the Study of Religious Culture. Cover: Painting by István Demeter All the language proofreading were made by Cozette Griffin-Kremer, Nancy Cassel McEntire and David Stanley ISBN 978-963-306-254-8 ISSN 1419-1288 (Szegedi Vallási Néprajzi Könyvtár) ISSN 2064-4825 (A Vallási Kultúrakutatás Könyvei ) ISSN 2228-1347 (Yearbook of the SIEF Working Group on the Ritual Year) © The Authors © The Editors All rights reserved Printed in Hungary Innovariant Nyomdaipari Kft., Algyő General manager: György Drágán www.innovariant.hu https://www.facebook.com/Innovariant CONTENTS Foreword .......................................................................................................................... 7 POLITICS AND THE REMEMBraNCE OF THE Past Emily Lyle Modifications to the Festival Calendar in 1600 and 1605 during the Reign of James VI and -

Udmurtia. Horizons of Cooperation.Pdf
UDMURTIA Horizons of Cooperation The whole world is familiar fiber, 8th – in production of pork; or hammer out a nail for a house with the gun maker Mikhail Ka- it is among 5 major regions - fur- with your own hands to have a tra- lashnikov, motor cycles «Izh», the niture producers in Russia and ditional Udmurt wedding, to re- composer Pyotr Tchaikovsky and among 10 major regions of Russia cover physical health with help of the skier Galina Kulakova but as producing dairy and meat prod- unique mud, mineral waters and long as 20 years ago there were ucts. health-giving honey (apiotherapy) few people who were able to as- Acquaintance with future part- and spiritual health – in cathe- sociate them with Udmurtia. Now ners from Udmurtia is related to drals and at sacred springs, to re- it is just a fact in history explained business tourism. Citizens of oth- lieve stresses of the metropolitan by strategic significance of the er countries and regions of Russia city in the patriarchal tranquility Republic in the defense complex when selecting a holiday destina- of villages, to choose an educa- of Russia and its remoteness from tion will not consider our region tional institution for studying. the state borders. as a health resort or touristic cen- Udmurtia is the region of hospi- Business partner highly appre- ter along with London or Paris in table and purposeful people open ciate products manufactured in the first place. for dialogue and cooperation. the Republic and extend relations However, Udmurtia is attrac- with its manufacturers. tive not only as the industrial-in- Udmurtia produces equipment novative or educational center. -

Booklet Elecond.Pdf
ОАО "Элеконд" является одним из основных производителей и поставщиков на российский рынок и в страны СНГ алюминиевых, ниобиевых и танталовых конденсаторов. Предприятие находится в городе Сарапуле Удмуртской республики, в одном из промышленно развитых районов Западного Урала, Имеет удобное транспортное сообщение. Через г. Сарапул проходит Горьковская железная дорога, есть речной порт. Город связан сетью автомобильных дорог с соседними областными центрами, республиками, аэропортом города Ижевска, Open Joint-Stock Company «ELECOND», a leading Russian manufacturer of aluminum, tantalum and niobium capacitors, supplies its products to RF and CIS markets. The company is situated in Sarapul, Udmurt Republic - an industrially developed region of Western Ural. Sarapul has favorable transport communications: it has a railway station (Gorky railway) and a river port and is connected to neighboring regional centers, republics and airport of Izhevsk via roads, Удмуртская Республика расположена в западной части Среднего Урала между реками Кама и Вятка. На западе и севере она граничит с Кировской областью, на востоке - с Пермской областью, на юге - с Башкортостаном и Татарстаном. Территория Удмуртии занимает площадь 42,1 тыс.кв.км. Столица - город Ижевск. Наиболее древние археологические памятники свидетельствуют о том, что люди на территории Удмуртии появились в эпоху мезолита (8-5 тыс. лет до н.э.). Первые русские поселения появились на р. Вятке в XII-XIII веках. Север Удмуртии стал частью формирующегося Русского государства. К 1557 году после взятия Иваном Грозным Казани завершился процесс присоединения удмуртов к Русскому государству. До Октябрьской революции территория Удмуртии входила в состав Казанской и Вятской губерний. Благодаря своему выгодному геополитическому положению Удмуртия в XX веке превратилась в крупный промышленный центр страны. \VS Сегодня Удмуртская Республика является неотъемлемой составной частью Российской Федерации. -

A Necktie for Lawyer Shumkov
A Necktie for Lawyer Shumkov By Vladimir Voronov Translated by Arch Tait January 2016 This article is published in English by The Henry Jackson Society by arrangement with Radio Free Europe / Radio Liberty. The article refects the views of the author and not necessarily those of The Henry Jackson Socity or its staf. A NECKTIE FOR LAWYER SHUMKOV 1 On the evening of Friday, 4 December 2015 the body of 43-yeAr old Dmitry Shumkov wAs discovered in an office in the Federation Tower of the Moscow City business centre. Shumkov’s name became known to the general public only from reports of his deAth. These reports, summArizing the dynamic business life of the deceAsed, reveAled that Mr Shumkov wAs A dollAr billionaire; co-owner of the Olympic Sports Complex in Moscow; co-owner of the Norilsk-1 mines; co-owner of A complex of buildings AdjAcent to the Kremlin on VArvarka Street And Kitai- Gorod Drive; owner of a “Centre for Network Impact Technology”, which is one of the top five Internet traffic regulators; And, owner of A mAjority holding in the Moscow Internet eXchange” (MSK-IX) hub, which serves 60% of Russian Internet trAffic, And of NGENIX, the mArket leAder in services providing content. The successes of the deceAsed were not confined to business. He wAs one of the top ten Russian lawyers, A Doctor of Laws, Professor of Public Administration And Legal Support of State And Municipal Services of the Russian Presidential AcAdemy of NAtionAl Economy and Public Service, Academic Director of the Institute of Energy Law At the Kutafin Moscow State Law University, A member of the Presidium of the Russian Law Society And ChairmAn of the BoArd of the Russian NAtionAl Centre for Legal InitiAtives. -

Classification of Urban Habitats of Towns of the Udmurt Republic (Russia)
Plants in Urban Areas and Landscape Slovak University of Agriculture in Nitra Faculty of Horticulture and Landscape Engineering DOI 10.15414/2014.9788055212623.105–107 CLASSIFICATION OF URBAN HABITATS OF TOWNS OF THE UDMURT REPUBLIC (RUSSIA) Ekaterina N. ZYANKINA, Olga G. BARANOVA* Udmurt State University, Russia The purpose of this study is to discover the species composition of urban floras through studying and comparing certain partial floras. The object of our research is flora of small towns in Udmurtia. We have developed methodological approaches for analysis of different urban habitats. These approaches are significant for identifying of plants species composition in cities. This study is based on the method of partial floras. The term “partial flora” is understood in the interpretation of Boris A. Yurtsev. This method is widely used in Russia (Yurtsev, 1982). We’ve created the classification of habitats groups based on examination of cartographic material, aerial and satellite photography, primary analysis of the flora habitats. We have distinguished two types, 16 classes and 43 habitats kinds. The Type of natural and semi-natural habitats with little disturbance of vegetation is divided into 7 classes of habitats: meadow, forest, forest-steppe, swamp, water, coastal, naturally bare habitats. The type of anthropogenically – transformed habitats includes 9 classes: communicationly-tape, erosion, slotted, agricultural, water, artificial tree plantation, landfills, landscape gardenings, cemeteries Preliminary lists of kinds of partial flora habitats are made. Both native and alien species of plants are allocated there. Alien flora fraction was divided into groups according to the degree of danger for biodiversity. Typical species were pointed out for all habitats. -

DEPARTURE CITY CITY DELIVERY Region Terms of Delivery
DEPARTURE Terms of delivery COST OF CITY DELIVERY Region CITY (working days) DELIVERY Moscow VIP - in Yekaterinburg Sverdlovsk 1 845 Moscow VIP - by Kazan Rep. Tatarstan 1 845 Moscow VIP - on Kaliningrad Kaliningrad 1-2 845 Moscow VIP - in Krasnodar Krasnodar region 1 845 Moscow VIP - around Krasnoyarsk (unless in Krasnoyarsk) Krasnoyarsk region 1 1420 Moscow VIP - Moscow Moscow 1 1420 Moscow VIP - in Nizhny Novgorod Nizhny Novgorod 1 845 Moscow VIP - in Novosibirsk Novosibirsk 1 1420 Moscow VIP - for Perm Perm 1 845 Moscow VIP - to Rostov-on-Don Rostov 1 845 Moscow VIP - by Samara Samara 1 845 Moscow VIP - in St. Petersburg Leningrad 1 1420 Moscow VIP - of Ufa Rep. Bashkiria 1 845 Moscow A.Kosmodemyanskogo village (Kaliningrad) Kaliningrad 2-3 550 Moscow Ababurovo (Leninsky district, Moscow region). Moscow 2-3 930 Moscow Abaza (Resp. Khakassia) Khakassia 6-7 1645 Moscow Abakan (rep. Khakassia) Khakassia 3-4 1180 Moscow Abbakumova (Moscow region). Moscow 2-3 930 Moscow Abdreevo (Ulyanovsk region.) Ulyanovsk 3-4 1300 Moscow Abdullno (Orenburg region). Orenburg 4-5 1060 Moscow Abdulov (Ulyanovsk region.) Ulyanovsk 3-4 1300 Moscow Abinsk (Krasnodar) Krasnodar region 3-6 1300 Moscow Abramovka (Ulyanovsk region.) Ulyanovsk 3-4 1300 Moscow Abramtsevo (Balashikha district, Moscow region). Moscow 2-3 930 Moscow Abrau Djurso (Krasnodar) Krasnodar region 3-5 1060 Moscow Avdon (rep. Bashkortostan) Bashkortostan 4 630 Moscow Aviators (Balashikha district, Moscow region). Moscow 2-3 930 Moscow Autorange (Moscow region). Moscow 2-3 930 Moscow Agalatovo (Len.oblasti) Leningrad 4 1060 Moscow Ageevka (Orel). Oryol 2-3 930 Moscow Aghidel (rep. -

Agrarian Technologies in Russia in the Late XIX - Early XX Centuries: Traditions and Innovations (Basing on the Materials of Vyatka Province)
ISSN 0798 1015 HOME Revista ESPACIOS ! ÍNDICES ! A LOS AUTORES ! Vol. 38 (Nº 52) Year 2017. Page 32 Agrarian technologies in Russia in the late XIX - early XX centuries: traditions and innovations (basing on the materials of Vyatka province) Tecnologías agrarias en Rusia a finales del siglo XIX-principios del XX: tradiciones e innovaciones (basándose en los materiales de la provincia de Vyatka) Alexey IVANOV 1; Anany IVANOV 2; Alexey OSHAYEV 3; Anatoly SOLOVIEV 4; Aleksander FILONOV 5 Received: 09/10/2017 • Approved: 21/10/2017 Content 1. Introduction 2. Methodology 3. Results 4. Conclusions Bibliographic references ABSTRACT: RESUMEN: Basing on a wide range of published and unpublished Basándose en una amplia gama de fuentes publicadas e sources the article examines the historical experience of inéditas, el artículo examina la experiencia histórica de introducing and disseminating new technologies of la introducción y difusión de nuevas tecnologías de agricultural production in the peasant economy of producción agrícola en la economía campesina de la Vyatka province in the late 19th and early 20th provincia de Vyatka a fines del siglo XIX y principios del centuries when the most important changes took place XX, cuando se produjeron los cambios más importantes in the agriculture of Russia. The most notable en la agricultura de Rusia. El fenómeno más notable phenomenon for the agricultural province was the para la provincia agrícola fue la introducción de una introduction of a multi-field (grass-field) crop rotation in rotación de cultivos -

IZHEVSK ELECTROMECHANICAL PLANT) ━━ Two-Component Solutions for Peritoneal Dialysis
INVESTMENT AUDIT OF THE UDMURT REPUBLIC. VERSION 1.0 UDMURTIA ON THE MAP OF RUSSIA 1 Moscow MADE IN UDMURTIA Kirov 42,100 SQ KM Perm Nizhny Novgorod Area Izhevsk (56th/85*) Kazan Yekaterinburg Ufa Samara 1.5M Population (30th/85*) UDMURTIA’S LARGEST CITIES RUB 556BN 970 КМ GRP IZHEVSK 650,000 Distance from Izhevsk (33rd/85*) to Moscow: SARAPUL 98,000 2 hours VOTKINSK 98,000 18 hours — 1200 km GLAZOV 93,000 RUB 356,043 GRP per capita (42nd/85) KEY TRANSPORT INFRASTRUCTURE: Trans-Siberian Railway (Balezino Station, Glazov Station) The P320 Elabuga-Izhevsk regional highway, connection to M7 Volga. Udmurt Republic * ranking among Russian regions Volga Federal District (VFD) IGOR SHUVALOV MAKSIM ORESHKIN DENIS MANTUROV DMITRY PATRUSHEV 3 Chairman of VEB.RF Minister of Economic Development Minister of Industry and Trade Minister of Agriculture THE REGIONAL ADMINISTRATION HAS INITIATED AN INVESTMENT AUDIT TO SUPPORT UDMURTIA’S LONG-TERM ECONOMIC DEVELOPMENT MADE IN UDMURTIA 2014 2017 2019 2020 “VEB.RF, the Russian Export “Udmurtia’s focus on driving non- “Udmurtia is a region with “Udmurtia’s climate and Centre, DOM.RF and the SME resource-based exports, training enormous investment potential environment provide an excellent Investment strategy Map of investment Investment audit Udmurt Republic’s 2027 opportunities Social and Economic Corporation are providing people entrepreneurs and promoting and ambitious goals to develop foundation for the further Udmurtia’s 2025 The investment audit of Strategy of Udmurtia with essential support entrepreneurship, enhancing the manufacturing sector. There development of the agribusiness, Investment Strategy In 2017, Udmurtia the Udmurt Republic will tools to attract investors, open productivity and adopting best is intense demand for investment food, raw materials and consumer is aimed at enhancing undertook a massive highlight the following: The strategy will be based on new manufacturing sites, create practices from other regions, among companies in Udmurtia goods sectors. -

I–V Century Middle Kama Tarasovo Burial Ground – a Unique Monument of Ancient Udmurts
Estonian Journal of Archaeology, 2017, 21, 2, 186–215 https://doi.org/10.3176/arch.2017.2.05 Rimma Goldina I–V CENTURY MIDDLE KAMA TARASOVO BURIAL GROUND – A UNIQUE MONUMENT OF ANCIENT UDMURTS The Tarasovo burial ground (Russia, Udmurtia) is the largest among researched Finno- Ugric monuments of the I–V c. in Eurasia. It was excavated in 1980–1997 by the Kama- Vyatka archaeological expedition of the Udmurt State University (Izhevsk) under the guidance of Professor R. D. Goldina. 1,880 graves containing 2,096 burials and over 37,000 artifects were excavated on the area of more than 16,000 sq. m. The cemetery is dated to the end of the Early Iron Age and the Great Migration period (in the Middle Kama Region – the Cheganda archaeological culture of the Pyanoborye culture-historical community – ancient Udmurts). The monument is located on the territory of the IV–III c. BC sanctuary the remains of which were also studied. Materials of the monument are under study of the group of archaeologists at the Udmurt State University. The paper gives a brief review of the following studies: burial ritual, chronological account of the materials from the I to V centuries, numerous categories of goods such as metal decorations, belt set, fibulas, earthenware, weapons: bladed weapons, helmets, armour, heads of spears and arrows, fighting scythes, axes, scabbard, horse tack, etc. Rimma Goldina, Department of History, Archaeology and Ethnology of Udmurtia of the Institute of History and Sociology at the Udmurt State University, 1 Universitetskaya St., 426034 Izhevsk, Russia; [email protected] Introduction At present, the Tarasovo burial ground is the largest among all known and researched Finno-Ugric burial monuments in Eurasia. -
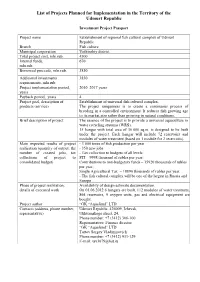
List of Projects Planned for Implementation in the Territory of the Udmurt Republic
List of Projects Planned for Implementation in the Territory of the Udmurt Republic Investment Project Passport Project name Establishment of regional fish cultural complex of Udmurt Republic Branch Fish culture Municipal corporation Votkinskiy district Total project cost, mln.rub. 4500 Internal funds, 670 mln.rub. Borrowed proceeds, mln.rub. 3830 Additional investments 3830 requirements, mln.rub. Project implementation period, 2010–2017 years years Payback period, years 4 Project goal, description of Establishment of universal fish cultural complex. products (service) The project uniqueness is to create a continuous process of breeding in a controlled environment. It reduces fish growing age to its market size rather than growing in natural conditions. Brief description of project The essence of the project is to provide a universal aquaculture in water recycling systems (WRS). 15 hangar with total area of 36 000 sq.m. is designed to be built under the project. Each hangar will include 72 reservoirs and modules of water treatment (based on 1 module for 2 reservoirs). Main expected results of project - 3 000 tones of fish production per year realization (quantity of output, the - 350 new jobs number of created jobs, tax - Tax collection to budgets of all levels: collections of project to PIT – 9998 thousand of rubles per year; consolidated budget) Contributions to non-budgetary funds – 15920 thousands of rubles per year; Single Agricultural Tax – 18890 thousands of rubles per year. - The fish cultural complex will be one of the largest in Russia and Europe Phase of project realization, Availability of design estimate documentation. details of executed work On 01.06.2012 6 hangars are built, 112 modules of water treatment, 864 reservoirs, 9 oxygen units, gas and electrical equipment are bought. -

Peasant Identities in Russia's Turmoil
PEASANT IDENTITIES IN RUSSIA’S TURMOIL: STATUS, GENDER, AND ETHNICITY IN VIATKA PROVINCE, 1914-1921 DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Aaron Benyamin Retish, M.A. The Ohio State University, 2003 Dissertation Committee: Approved by Professor David Hoffmann, Adviser Professor Eve Levin _________________ Professor Nicholas Breyfogle Adviser Department of History Copyright by Aaron Benyamin Retish 2003 ABSTRACT From 1914-21, the Russian countryside underwent an enormous social and political transformation. World War I and civil war led to conscription into the tsarist, Bolshevik, and anti-Bolshevik armies, removing over fourteen million young male peasants from their villages. Revolution destroyed the centuries-old peasant-landlord relationship, redistributed land among the peasantry, democratized the countryside, and allowed villages to install autonomous governing bodies. War and social turmoil also brought massive famine and government requisitioning of grain and possessions, killing thousands of peasants and destroying their means of existence. The Bolshevik victory, a defining event of the twentieth century, was ultimately determined by the temporary support of the peasantry, the vast majority of Russia's population. This project studies the interaction between peasants and government in the Russian province of Viatka from the beginning of World War I to the end of the Civil War in 1921. In doing so, it will advance how scholars understand the nature of the Revolution, peasant-state relations, and peasant society and culture in general. On the ii one hand, I analyze Russia’s changes through a study of peasant responses to tsarist, Provisional Government, and Soviet recruitment into the armed forces; requisitioning of grain and possessions; and establishment of local administrations.