Review Human African Trypanosomiasis: Current
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Health Information for International Travel 1996-97
CDCCENTERS FOR DISEASE CONTROL AND PREVENTION Health Information for International Travel 1996-97 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service This document was created with FrameMaker 4.0.4 ATTENTION READERS It is impossible for an annual publication on international travel to remain absolutely current given the nature of disease transmission in the world today. For readers of this text to be the most up-to-date on travel-related diseases and recommendations, this text must be used in conjunction with the other services provided by the Travelers’ Health Section of the Centers for Disease Control and Prevention (CDC). Changes such as vaccine requirements, disease outbreaks, drug availability, or emerging infections will be posted promptly on these services. For these and other changes, please consult either our Voice or Fax Information Service at 404-332-4559 or our Internet address on the World Wide Web Server at http://www.cdc.gov or the File Transfer Protocol server at ftp.cdc.gov . Because certain countries require vaccination against yellow fever only if a traveler arrives from a country currently infected with this disease, it is essential that up-to-date information regarding infected areas be maintained for reference. The CDC publishes a biweekly "Summary of Health Information for Interna- tional Travel" (Blue Sheet) which lists yellow fever infected areas. Subscriptions to the Blue Sheet are available to health departments, physicians, travel agencies, international airlines, shipping companies, travel clinics, and other private and public agencies that advise international travelers concerning health risks they may encounter when visiting other countries. -

Autophagy in Trypanosomatids
Cells 2012, 1, 346-371; doi:10.3390/cells1030346 OPEN ACCESS cells ISSN 2073-4409 www.mdpi.com/journal/cells Review Autophagy in Trypanosomatids Ana Brennand 1,†, Eva Rico 2,†,‡ and Paul A. M. Michels 1,* 1 Research Unit for Tropical Diseases, de Duve Institute, Université catholique de Louvain, Avenue Hippocrate 74, postal box B1.74.01, B-1200 Brussels, Belgium; E-Mail: [email protected] 2 Department of Biochemistry and Molecular Biology, University Campus, University of Alcalá, Alcalá de Henares, Madrid, 28871, Spain; E-Mail: [email protected] † These authors contributed equally to this work. ‡ Present Address: Centre for Immunity, Infection and Evolution, Institute of Immunology and Infection Research, School of Biological Sciences, King’s Buildings, University of Edinburgh, West Mains Road, Edinburgh EH9 3JT, UK. * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +32-2-7647473; Fax: +32-2-7626853. Received: 28 June 2012; in revised form: 14 July 2012 / Accepted: 16 July 2012 / Published: 27 July 2012 Abstract: Autophagy is a ubiquitous eukaryotic process that also occurs in trypanosomatid parasites, protist organisms belonging to the supergroup Excavata, distinct from the supergroup Opistokontha that includes mammals and fungi. Half of the known yeast and mammalian AuTophaGy (ATG) proteins were detected in trypanosomatids, although with low sequence conservation. Trypanosomatids such as Trypanosoma brucei, Trypanosoma cruzi and Leishmania spp. are responsible for serious tropical diseases in humans. The parasites are transmitted by insects and, consequently, have a complicated life cycle during which they undergo dramatic morphological and metabolic transformations to adapt to the different environments. -

Programme Against African Trypanosomiasis Year 2006 Volume
ZFBS 1""5 1SPHSBNNF *44/ WPMVNF "HBJOTU "GSJDBO QBSU 5SZQBOPTPNJBTJT 43%43%!.$4290!./3/-)!3)3).&/2-!4)/. $EPARTMENTFOR )NTERNATIONAL $EVELOPMENT year 2006 PAAT Programme volume 29 Against African part 1 Trypanosomiasis TSETSE AND TRYPANOSOMIASIS INFORMATION Numbers 13466–13600 Edited by James Dargie Bisamberg Austria FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS Rome, 2006 The designations employed and the presentation of material in this information product do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations concerning the legal or development status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. All rights reserved. Reproduction and dissemination of material in this in- formation product for educational or other non-commercial purposes are authorized without any prior written permission from the copyright holders provided the source is fully acknowledged. Reproduction of material in this information product for resale or other commercial purposes is prohibited without written permission of the copyright holders. Applications for such permission should be addressed to the Chief, Electronic Publishing Policy and Support Branch, Information Division, FAO, Viale delle Terme di Caracalla, 00100 Rome, Italy or by e-mail to [email protected] © FAO 2006 Tsetse and Trypanosomiasis Information Volume 29 Part 1, 2006 Numbers 13466–13600 Tsetse and Trypanosomiasis Information TSETSE AND TRYPANOSOMIASIS INFORMATION The Tsetse and Trypanosomiasis Information periodical has been established to disseminate current information on all aspects of tsetse and trypanosomiasis research and control to institutions and individuals involved in the problems of African trypanosomiasis. -
M the Battle Against Neglected Tropical Diseases Forging the Chain “Results Innovative Build Trust, and with Intensified Trust, Commitment Management Escalates.”
SCENES FROM THE BATTLE AGAINST NEGLECTED TROPICAL DISEASES FORGING THE CHAIN “RESULTS INNOVATIVE BUILD TRUST, AND WITH INTENSIFIED TRUST, COMMITMENT MANAGEMENT ESCALATES.” Dr Margaret Chan, WHO Director-General “RESULTS INNOVATIVE BUILD TRUST, AND WITH INTENSIFIED TRUST, COMMITMENT MANAGEMENT ESCALATES.” Dr Margaret Chan, WHO Director-General WHO Library Cataloguing-in-Publication Data Forging the chain: scenes from the battle against neglected tropical diseases, with the support of innovative partners. 1. Tropical Medicine 2. Neglected Diseases I. World Health Organization ISBN 978 92 4 151000 4 (NLM classification: WC 680) © World Health Organization 2016 Acknowledgements All rights reserved. Publications of the World Health Organization are available on the WHO website Forging the chain: scenes from the battle against neglected tropical diseases (with the support of (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, innovative partners) was prepared by the Innovative and Intensified Disease Management (IDM) unit 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). of the WHO Department of Control of Neglected Tropical Diseases under the overall coordination and supervision of Dr Jean Jannin. Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press through the WHO website The writing team was coordinated by Deboh Akin-Akintunde and Lise Grout, in collaboration with (www.who.int/about/licensing/copyright_form/en/index.html). Grégoire Rigoulot Michel, Pedro Albajar Viñas, Kingsley Asiedu, Daniel Argaw Dagne, Jose Ramon Franco Minguell, Stéphanie Jourdan, Raquel Mercado, Gerardo Priotto, Prabha Rajamani, Jose The designations employed and the presentation of the material in this publication do not imply the Antonio Ruiz Postigo, Danilo Salvador and Patricia Scarrott. -

COVID-19 Mrna Pfizer- Biontech Vaccine Analysis Print
COVID-19 mRNA Pfizer- BioNTech Vaccine Analysis Print All UK spontaneous reports received between 9/12/20 and 22/09/21 for mRNA Pfizer/BioNTech vaccine. A report of a suspected ADR to the Yellow Card scheme does not necessarily mean that it was caused by the vaccine, only that the reporter has a suspicion it may have. Underlying or previously undiagnosed illness unrelated to vaccination can also be factors in such reports. The relative number and nature of reports should therefore not be used to compare the safety of the different vaccines. All reports are kept under continual review in order to identify possible new risks. Report Run Date: 24-Sep-2021, Page 1 Case Series Drug Analysis Print Name: COVID-19 mRNA Pfizer- BioNTech vaccine analysis print Report Run Date: 24-Sep-2021 Data Lock Date: 22-Sep-2021 18:30:09 MedDRA Version: MedDRA 24.0 Reaction Name Total Fatal Blood disorders Anaemia deficiencies Anaemia folate deficiency 1 0 Anaemia vitamin B12 deficiency 2 0 Deficiency anaemia 1 0 Iron deficiency anaemia 6 0 Anaemias NEC Anaemia 97 0 Anaemia macrocytic 1 0 Anaemia megaloblastic 1 0 Autoimmune anaemia 2 0 Blood loss anaemia 1 0 Microcytic anaemia 1 0 Anaemias haemolytic NEC Coombs negative haemolytic anaemia 1 0 Haemolytic anaemia 6 0 Anaemias haemolytic immune Autoimmune haemolytic anaemia 9 0 Anaemias haemolytic mechanical factor Microangiopathic haemolytic anaemia 1 0 Bleeding tendencies Haemorrhagic diathesis 1 0 Increased tendency to bruise 35 0 Spontaneous haematoma 2 0 Coagulation factor deficiencies Acquired haemophilia -

Diseases of the Digestive System (KOO-K93)
CHAPTER XI Diseases of the digestive system (KOO-K93) Diseases of oral cavity, salivary glands and jaws (KOO-K14) lijell Diseases of pulp and periapical tissues 1m Dentofacial anomalies [including malocclusion] Excludes: hemifacial atrophy or hypertrophy (Q67.4) K07 .0 Major anomalies of jaw size Hyperplasia, hypoplasia: • mandibular • maxillary Macrognathism (mandibular)(maxillary) Micrognathism (mandibular)( maxillary) Excludes: acromegaly (E22.0) Robin's syndrome (087.07) K07 .1 Anomalies of jaw-cranial base relationship Asymmetry of jaw Prognathism (mandibular)( maxillary) Retrognathism (mandibular)(maxillary) K07.2 Anomalies of dental arch relationship Cross bite (anterior)(posterior) Dis to-occlusion Mesio-occlusion Midline deviation of dental arch Openbite (anterior )(posterior) Overbite (excessive): • deep • horizontal • vertical Overjet Posterior lingual occlusion of mandibular teeth 289 ICO-N A K07.3 Anomalies of tooth position Crowding Diastema Displacement of tooth or teeth Rotation Spacing, abnormal Transposition Impacted or embedded teeth with abnormal position of such teeth or adjacent teeth K07.4 Malocclusion, unspecified K07.5 Dentofacial functional abnormalities Abnormal jaw closure Malocclusion due to: • abnormal swallowing • mouth breathing • tongue, lip or finger habits K07.6 Temporomandibular joint disorders Costen's complex or syndrome Derangement of temporomandibular joint Snapping jaw Temporomandibular joint-pain-dysfunction syndrome Excludes: current temporomandibular joint: • dislocation (S03.0) • strain (S03.4) K07.8 Other dentofacial anomalies K07.9 Dentofacial anomaly, unspecified 1m Stomatitis and related lesions K12.0 Recurrent oral aphthae Aphthous stomatitis (major)(minor) Bednar's aphthae Periadenitis mucosa necrotica recurrens Recurrent aphthous ulcer Stomatitis herpetiformis 290 DISEASES OF THE DIGESTIVE SYSTEM Diseases of oesophagus, stomach and duodenum (K20-K31) Ill Oesophagitis Abscess of oesophagus Oesophagitis: • NOS • chemical • peptic Use additional external cause code (Chapter XX), if desired, to identify cause. -

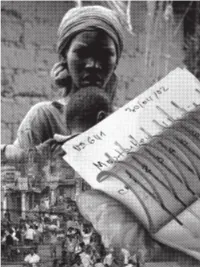
The Battle Is Not Over Until It Is Won
HUMAN AFRICAN TRYPANOSOMIASIS SLEEPING SICKNESS The battle is not over until it is won Sleeping sickness, or human African trypa- melarsoprol. The latter, however, is still the nosomiasis, threatens millions of people in first-line treatment for the less commonT.b. 36 countries across sub-Saharan Africa. The rhodesiense HAT. Democratic Republic of the Congo bears the To contribute to the WHO elimination goal, a brunt, accounting for 83% of all cases. In the ‘test and treat’ strategy that would be imple- 1960s there were less than 5,000 patients mented at the primary healthcare level is on suffering from the disease in the whole of the the horizon, with potential simple oral pills continent. However, the end of the 20th cen- for both the early and late stage as well as tury – with internal conflict, competing health both types of HAT, that are currently in devel- priorities, and decolonization – witnessed a opment, along with new rapid diagnostics, halt in the successful control methods, and which together would remove the need for the number of cases reported rose painful and dangerous lumbar punc- steeply, peaking in 1998 with tures. This would mean that rural over 37,000 cases reported in health centres, rather than hos- that year. Nowadays, thanks pitals, will play an increasingly to the combined efforts of important role, especially as the WHO, National Sleeping number of reported cases con- Sickness Control Pro- tinues to dwindle. grammes, NGOs and other partners, the disease has once more been brought under control, and since 2010 the number of reported cases has fallen below 8,000. -

Plants As Sources of Anti-Protozoal Compounds
PLANTS AS SOURCES OF ANTI- PROTOZOAL COMPOUNDS Thesis presented by Angela Paine for the degree of Doctor of Philosophy in the Faculty of Medicine of the University of London Department of Pharmacognosy The School of Pharmacy University of London 1995 ProQuest Number: 10104878 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest. ProQuest 10104878 Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States Code. Microform Edition © ProQuest LLC. ProQuest LLC 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106-1346 dedicated to my late father Abstract The majority of the world's population relies on traditional medicine, mainly plant-based, for the treatment of disease. This study focuses on plant remedies used to treat tropical diseases caused by protozoan parasites. The following protozoal diseases: African trypanosomiasis, leishmaniasis. South American trypanosomiasis and malaria, and the traditional use of plant remedies in their treatment, are reviewed in a world wide context. In the present work, vector and mammalian forms of Trypanosoma b. brucei, the vector forms of Leishmania donovani and Trypanosoma cruzi and the mammalian forms of Plasmodium falciparum were maintained in culture in vitro in order to evaluate the activity of a series of plant extracts, pure natural products and synthetic analogues against these protozoan parasites in vitro. -
Program and Abstracts
Seventy 2019 years of Soixante-dix AU/ISCTRC Années de 1949 l’UA / CSIRLT 35TH GENERAL CONFERENCE OF THE INTERNATIONAL SCIENTIFIC COUNCIL FOR TRYPANOSOMIASIS RESEARCH AND CONTROL (ISCTRC) AND 18TH PATTEC NATIONAL COORDINATORS MEETING PROGRAMME AND ABSTRACTS BOOK 35TH GENERAL CONFERENCE OF THE INTERNATIONAL SCIENTIFIC COUNCIL FOR TRYPANOSOMIASIS RESEARCH AND CONTROL (ISCTRC) AND 18TH PATTEC NATIONAL COORDINATORS MEETING PROGRAMME AND ABSTRACTS BOOK ABOUT THE CONFERENCE Theme of the Conference Impact of African Trypanosomiasis on Human and Animal Health, Sustainable Agriculture and Rural Development in the face of challenges to sustainable investment in AAT control and HAT elimination”Members of the Scientific Committee The members of the 35th ISCTRC Scientific Committee that were appointed by the Director of AU-IBAR were drawn from various institutions working on Tsetse and Trypanosomiasis. The committee received and considered 140 abstracts addressing the various sub- themes of the conference. Prof. Ahmed Elsawalhy, Director of AU-IBAR, Chairperson Dr. James Wabacha, ISCTRC Secretary, Member Dr. Gift Wanda, Member Dr. Daniel Masiga, Member Dr. Jose Ramon Franco Rapporteur and Moderators Rapporteur General Grace Mulira Deputy Rapporteur General Njelembo Mbewe Moderators and rapporteurs for the various thematic sessions are as per the programme Presentation guidelines Allocated time for presentations: Each presentation will be allocated 10 minutes and 5 minutes for discussion. Viewing of posters There will be continuous viewing of the posters. The presenters for the posters will be at the stands during the coffee/tea breaks. There will be general discussion on the posters in the plenary on Thursday, 26th September 2019. Uploading of presentations in the conference computer Presenters who will be making presentation during the first day are IV requested to upload their presentation during registration on Sunday. -
Somnology-Jr-Book.Pdf
1 To Grace Zamudio and Zoe Lee-Chiong. 2 Preface Carpe noctem. Teofilo Lee-Chiong MD Professor of Medicine Division of Sleep Medicine National Jewish Health Denver, Colorado University of Colorado Denver School of Medicine Denver, Colorado Chief Medical Liaison Philips Respironics Murrysville, Pennsylvania 3 Abbreviations AHI Apnea-hypopnea index BPAP Bi-level positive airway pressure CPAP Continuous positive airway pressure CSA Central sleep apnea ECG Electrocardiography EEG Electroencephalography EMG Electromyography EOG Electro-oculography FEV1 Forced expiratory volume in 1 second GABA Gamma-aminobutyric acid N1 NREM stage 1 sleep N2 NREM stage 2 sleep N3 NREM stages 3 (and 4) sleep NREM Non-rapid eye movement O2 Oxygen OSA Obstructive sleep apnea PaCO2 Partial pressure of arterial carbon dioxide PaO2 Partial pressure of arterial oxygen REM Rapid eye movement sleep SaO2 Oxygen saturation SOREMP Sleep onset REM period 4 Table of contents Introduction 15 Neurobiology of sleep 16 Neural systems generating wakefulness 16 Neural systems generating NREM sleep 16 Neural systems generating REM sleep 16 Main neurotransmitters 17 Acetylcholine 17 Adenosine 17 Dopamine 17 Gamma-aminobutyric acid 17 Glutamate 17 Glycine 17 Histamine 18 Hypocretin 18 Melatonin 18 Norepinephrine 18 Serotonin 18 Physiology during sleep 19 Autonomic nervous system 19 Respiratory system 19 Respiratory patterns 19 Cardiovascular system 19 Gastrointestinal system 20 Renal and genito-urinary systems 20 Endocrine system 20 Growth hormone 20 Thyroid stimulating hormone -

Human Trypanosomiasis in India: Is It an Emerging New Zoonosis?
Chapter 4 Human Trypanosomiasis in India: Is it an Emerging New Zoonosis? Prashant P Joshi HUMAN TRYPANOSOMIASIS Trypanosomes are flagellated protozoan parasites infecting man (human trypanosomiasis) and a wide range of animals (animal trypanosomiasis) (Figures 1 and 6). Human trypanosomiasis is confined to Sub-Saharan Africa and Latin America and exists in two forms: 1. Human African trypanosomiasis (HAT) (sleeping sickness) is endemic in Sub-Saharan Africa. It is a dreadful fatal disease and was responsible for devastating epidemics in 1920s, with resurgence in 1990s. It is caused by Trypanosoma brucei (T.b.) gambiense (chronic form) or Trypanosoma brucei rhodesiense (acute form) and 2. American trypanosomiasis (Chagas disease) caused by T. cruzi is endemic in Latin America. Both diseases are transmitted by vectors: Human African Trypanosomiasis by infected saliva of Tsetse fly, and chagas by infected feces of bugs (Figure 2). Clinically, HAT has two Figure 2: Tsetse fly—the vector for HAT is not found in India stages: Stage 1 or hemolymphatic stage characterized by fever, cervical lymphadenopathy, especially in the posterior triangle (Winterbottom’s sign), splenomegaly, rash, pruritus, muscular pain, anemia, thrombocytopenia and carditis, which can sometimes be fatal. This is followed by stage two, the neurological phase or the meningoencephalitic stage with CNS invasion, in which there is marked sleep disturbance characterized by day-time somnolence and night-time insomnia. However, human trypanosomiasis of neither the kind which is evidenced in Africa and America, nor their vectors is found in India. ANIMAL TRYPANOSOMIASIS In contrast to human trypanosomiasis, animal trypano-somiasis has a worldwide distribution and is common in India. -
Section B – Abstracts
ISSN 0142-193X TSETSE AND TRYPANOSOMIASIS INFORMATION QUARTERLY Volume 22 Part 1, 1999 Numbers 10713–10823 DFID Cirad-emvt 1999 Tsetse and Trypanosomiasis Information Quarterly SECTION A – NEWS PROGRAMME AGAINST AFRICAN TRYPANOSOMIASIS Fourth Meeting of PAAT Programme Committee The fourth meeting of the PAAT Programme Committee was convened at IAEA Headquarters, Vienna, Austria, from 25 to 27 November 1998. The objective of meetings of the PAAT Committee is, on the basis of technical and scientific advice forwarded from the Advisory Group Co-ordinators and the Liaison Officers, to provide the focus for collaborative efforts to alleviate trypanosomiasis in Africa. Discussions at the current meeting were largely devoted to matters arising from the meeting of the PAAT Advisory Group Co-ordinators convened in Harare, Zimbabwe, October 1998 (see TTIQ, 21 (4)). Progress since the last meeting was reviewed. This included: ISCTRC representation on the Programme Committee and increased donor involvement; considerable progress on the development of the information systems for both animal and human trypanosomiasis (both the prototype PAAT-IS for animal trypanosomiasis and the CD-ROM-based information system developed by WHO for the human disease were demonstrated and the need for cross-linkages between the two was stressed); evaluation of the socio-economic impact of trypanosomiasis and the identification of priority control strategies; development of position papers on technical and policy aspects of the PAAT following open discussion via e-mail (that on drug resistance having been published as the first in the new PAAT Technical and Scientific Series); production and distribution of a glossy brochure announcing PAAT; and initiation of a quarterly PAAT Newsletter.