Somnology-Jr-Book.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How to Take a Sleep History
1/25/2015 How to take a sleep history Joan Santamaria Neurology Service and Multidisciplinary Sleep Disorders Unit Hospital Clínic of Barcelona 1.- Clinical history: Fundamental: the best “sleep test” Examination: helpful, but not always 2.- Investigations : Sleep tests: PSG, Video-PSG, respiratory polygraphy, MSLT, MWT, actimetry 3.- To rush into a sleep test without considering the history is of little use Taking a good sleep history The bed partner is essential By definition, people is unconscious during sleep Parasomnias, PLMs, Snoring, Sleep apnea, Seizures Daytime sleepiness may be neglected by some patients Even in insomnia patients, the bed partner information may be helpful 1 1/25/2015 Three main complaints I cannot sleep as much as I want (insomnia) Excessive daytime sleepiness (hypersomnia) Abnormal behaviors during sleep (parasomnias and other problems…noise, apnea, enuresis, seizures… ) What are the main questions? Nocturnal sleep characteristics Schedule of sleep during the week and week-end or holidays Latency to sleep, number of awakenings and cause (bathroom, pain, nightmare...) Time and type of final awakening (spontaneous/induced) Feel refreshed / tired on awakening? 23 1 4:30 6 8 Nocturnal sleep pattern Sleep onset insomnia 24 1:30 7:30 Delayed sleep phase 24 3 12 Week day Insufficient sleep 24 5:30 1 11 Week end (> 2 hrs additional sleep duration on week ends, high sleep efficiency) 2 1/25/2015 Sleep diary DEFINITION OF INSOMNIA Two key elements Nocturnal sleep: Difficulty in sleeping as much or as deep as one would -

Sleep and Its Disorders: Is the Problem
38 ISSN 0049-6804. «Врачеб. дело». 2017, № 1–2 ОБЗОР ЛИТЕРАТУРЫ 43. Williams G. R., Duncan Bassett J. H. Local control of thyroid hormone action: role of type 2 deiodinase Deiodinases: the balance of thyroid hormone // J. of Endocrinol. – 2011. – Vol. 209. – P. 261–272. 44. Wittmann G., Harney J. W., Singru P. S. et al. Inflammation-inducible type 2 deiodinase expres- sion in the leptomeninges, choroid plexus, and at brain blood vessels in male rodents // Endocri- nology. – 2014. – Vol. 155. – P. 2009–2019. 45. Yu J., Koenig R. J. Induction of type 1 iodothyronine deiodinase to prevent the nonthyroidal illness syndrome in mice // Endocrinol. – 2006. – Vol. 147, N 7. – Р. 3580–3585. СУЧАСНІ УЯВЛЕННЯ ПРО СИНДРОМ НЕТИРЕОЇДНОЇ ПАТОЛОГІЇ В КЛІНІЧНІЙ ПРАКТИЦІ Н. О. Абрамова, Н. В. Пашковська (Чернівці) Будь-які гострі та хронічні захворювання, що втягують у патологічний процес весь організм, можуть викликати порушення обміну тиреоїдних гормонів на фоні відсутності супутньої патології щитоподібної залози, гіпофіза та (або) гіпоталамуса. Такі порушення називають «син- дромом нетиреоїдної патології» (СНТП), або «синдромом низького Т3», і зустрічаються у 70 % госпіталізованих. У даному огляді ми розглянули етіологію, патогенез та частково шляхи корекції синдрому нетиреоїдної патології. Ключові слова: синдром нетиреоїдної патології, синдром низького Т3, порушення обміну тиреоїдних гормонів. CURRENT VIEWS ON NONTHYROIDAL ILLNESS SYNDROME IN CLINICAL PRACTICE (REVIEW) N. O. Abramova, N. V. Pashkovska (Chernivtsi, Ukraine) Higher State Educational Establishment of Ukraine «Bukovinian State Medical University» Any acute and chronic diseases that involve the whole organism into pathological process, can cause violation of thyroid hormones metabolism against a background of absence of concomitant diseases of thyroid gland, pituitary gland or hypothalamus. -

Autophagy in Trypanosomatids
Cells 2012, 1, 346-371; doi:10.3390/cells1030346 OPEN ACCESS cells ISSN 2073-4409 www.mdpi.com/journal/cells Review Autophagy in Trypanosomatids Ana Brennand 1,†, Eva Rico 2,†,‡ and Paul A. M. Michels 1,* 1 Research Unit for Tropical Diseases, de Duve Institute, Université catholique de Louvain, Avenue Hippocrate 74, postal box B1.74.01, B-1200 Brussels, Belgium; E-Mail: [email protected] 2 Department of Biochemistry and Molecular Biology, University Campus, University of Alcalá, Alcalá de Henares, Madrid, 28871, Spain; E-Mail: [email protected] † These authors contributed equally to this work. ‡ Present Address: Centre for Immunity, Infection and Evolution, Institute of Immunology and Infection Research, School of Biological Sciences, King’s Buildings, University of Edinburgh, West Mains Road, Edinburgh EH9 3JT, UK. * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +32-2-7647473; Fax: +32-2-7626853. Received: 28 June 2012; in revised form: 14 July 2012 / Accepted: 16 July 2012 / Published: 27 July 2012 Abstract: Autophagy is a ubiquitous eukaryotic process that also occurs in trypanosomatid parasites, protist organisms belonging to the supergroup Excavata, distinct from the supergroup Opistokontha that includes mammals and fungi. Half of the known yeast and mammalian AuTophaGy (ATG) proteins were detected in trypanosomatids, although with low sequence conservation. Trypanosomatids such as Trypanosoma brucei, Trypanosoma cruzi and Leishmania spp. are responsible for serious tropical diseases in humans. The parasites are transmitted by insects and, consequently, have a complicated life cycle during which they undergo dramatic morphological and metabolic transformations to adapt to the different environments. -

Sleepiness the Wheel
SLEEPINESS AT THE WHEEL WHITE PAPER SLEEPINESS AT THE WHEEL WHITE PAPER Sleepiness at the Wheel WHITE PAPER PREFACE Improving road safety is a priority of the French Government. Among the various causes of road accidents, one of them is especially common on motorways: lack of alertness, which leads to inattention and sleepiness. Lack of alertness is responsible for one in three collisions resulting in deaths on the motorway network, although it is the safest of all road networks! This phenomenon is not fully grasped by the public. Therefore, it is essential to gain knowledge and raise the publics’ awareness as regards sleepiness at the wheel. In more general terms, sleepiness at the wheel remains underestimated both socially and culturally speaking, which is a major issue for road safety and public health. This white book, put together by the French Motorway Companies (ASFA) and the National Institute of Sleep and Vigilance (INSV), presents the most recent knowledge on the subject at both the French and European levels and provides a number of recommendations. By contributing to a better understanding of sleepiness at the wheel, this work will help promote the implementation of new prevention strategies, to further reduce the number of victims on the road. Our objective is to cut down to less than 2000 the number of deaths per year on French roads by 2020. Manuel VALLS French Minister of Interior ASFA and INSV would like to express their deep thanks to the panel of European sleep experts who author this book. Most of them also participate in the research on traffic accidents associated with sleepiness in their own country and thus have contributed to enrich our knowledge and proposals for preventing from the consequences of sleepiness at the wheel. -

COVID-19 Mrna Pfizer- Biontech Vaccine Analysis Print
COVID-19 mRNA Pfizer- BioNTech Vaccine Analysis Print All UK spontaneous reports received between 9/12/20 and 22/09/21 for mRNA Pfizer/BioNTech vaccine. A report of a suspected ADR to the Yellow Card scheme does not necessarily mean that it was caused by the vaccine, only that the reporter has a suspicion it may have. Underlying or previously undiagnosed illness unrelated to vaccination can also be factors in such reports. The relative number and nature of reports should therefore not be used to compare the safety of the different vaccines. All reports are kept under continual review in order to identify possible new risks. Report Run Date: 24-Sep-2021, Page 1 Case Series Drug Analysis Print Name: COVID-19 mRNA Pfizer- BioNTech vaccine analysis print Report Run Date: 24-Sep-2021 Data Lock Date: 22-Sep-2021 18:30:09 MedDRA Version: MedDRA 24.0 Reaction Name Total Fatal Blood disorders Anaemia deficiencies Anaemia folate deficiency 1 0 Anaemia vitamin B12 deficiency 2 0 Deficiency anaemia 1 0 Iron deficiency anaemia 6 0 Anaemias NEC Anaemia 97 0 Anaemia macrocytic 1 0 Anaemia megaloblastic 1 0 Autoimmune anaemia 2 0 Blood loss anaemia 1 0 Microcytic anaemia 1 0 Anaemias haemolytic NEC Coombs negative haemolytic anaemia 1 0 Haemolytic anaemia 6 0 Anaemias haemolytic immune Autoimmune haemolytic anaemia 9 0 Anaemias haemolytic mechanical factor Microangiopathic haemolytic anaemia 1 0 Bleeding tendencies Haemorrhagic diathesis 1 0 Increased tendency to bruise 35 0 Spontaneous haematoma 2 0 Coagulation factor deficiencies Acquired haemophilia -

Diseases of the Digestive System (KOO-K93)
CHAPTER XI Diseases of the digestive system (KOO-K93) Diseases of oral cavity, salivary glands and jaws (KOO-K14) lijell Diseases of pulp and periapical tissues 1m Dentofacial anomalies [including malocclusion] Excludes: hemifacial atrophy or hypertrophy (Q67.4) K07 .0 Major anomalies of jaw size Hyperplasia, hypoplasia: • mandibular • maxillary Macrognathism (mandibular)(maxillary) Micrognathism (mandibular)( maxillary) Excludes: acromegaly (E22.0) Robin's syndrome (087.07) K07 .1 Anomalies of jaw-cranial base relationship Asymmetry of jaw Prognathism (mandibular)( maxillary) Retrognathism (mandibular)(maxillary) K07.2 Anomalies of dental arch relationship Cross bite (anterior)(posterior) Dis to-occlusion Mesio-occlusion Midline deviation of dental arch Openbite (anterior )(posterior) Overbite (excessive): • deep • horizontal • vertical Overjet Posterior lingual occlusion of mandibular teeth 289 ICO-N A K07.3 Anomalies of tooth position Crowding Diastema Displacement of tooth or teeth Rotation Spacing, abnormal Transposition Impacted or embedded teeth with abnormal position of such teeth or adjacent teeth K07.4 Malocclusion, unspecified K07.5 Dentofacial functional abnormalities Abnormal jaw closure Malocclusion due to: • abnormal swallowing • mouth breathing • tongue, lip or finger habits K07.6 Temporomandibular joint disorders Costen's complex or syndrome Derangement of temporomandibular joint Snapping jaw Temporomandibular joint-pain-dysfunction syndrome Excludes: current temporomandibular joint: • dislocation (S03.0) • strain (S03.4) K07.8 Other dentofacial anomalies K07.9 Dentofacial anomaly, unspecified 1m Stomatitis and related lesions K12.0 Recurrent oral aphthae Aphthous stomatitis (major)(minor) Bednar's aphthae Periadenitis mucosa necrotica recurrens Recurrent aphthous ulcer Stomatitis herpetiformis 290 DISEASES OF THE DIGESTIVE SYSTEM Diseases of oesophagus, stomach and duodenum (K20-K31) Ill Oesophagitis Abscess of oesophagus Oesophagitis: • NOS • chemical • peptic Use additional external cause code (Chapter XX), if desired, to identify cause. -

Sleep, Its Attributes, Deprivation & Hygiene: a Recapitulation
Review Article Annals of Sleep Medicine Research Published: 21 Jun, 2019 Sleep, Its Attributes, Deprivation & Hygiene: A Recapitulation Priyanka Malhotra* Nursing in Mental Health Nursing From PGIMER, Chandigarh, India Presently working as Nursing Tutor, AIIMS, Rishikesh, India Abstract Sleep is a biological and behavioral phenomenon that has been studied from many different perspectives. Today it is clear that sleep quantity and quality is related to the development of chronic diseases and even mental disorders. However, many people ignore their sleep habits and fail to take active steps to adopt sleep hygiene practices preferring instead to relay on non-prescribed or prescribed pharmacological products. As a result of the potential consequences of sleep deprivation, health care professionals should be vigilant of how managing underlying medical conditions may help to optimize sleep continuity and consider prescribing interventions that minimize sleep disruption. Keywords: Sleep; Sleep deprivation; Sleep hygiene Introduction Almost every night we are engaging ourselves in a sound sleep. However, pattern of sleep and its features vary from person to person. Various body functions such as metabolism, appetite, cardiovascular system, and immune system has been maintained and regulated by sleep. Hence, for the optimum level of health, sleep is an important factor [1,2]. Sleep is a state of reduced consciousness that is relatively easy to reverse. A normal healthy sleep is distinguish by good quality, appropriate time and regularity, enough duration and without any sleep disorder and disturbance [3]. Attributes of Normal Sleep OPEN ACCESS The stages of sleep have historically been divided into one stage of Rapid Eye Movement (REM) sleep and four stages (Stages 1-4) of Non-Rapid Eye Movement (NREM) sleep that are characterized *Correspondence: by increasing sleep depth. -

Parasomnias Revisited New Mexico Thoracic Society Sapna Bhatia Md 02/25/17 Objectives
PARASOMNIAS REVISITED NEW MEXICO THORACIC SOCIETY SAPNA BHATIA MD 02/25/17 OBJECTIVES • Appreciate the clinical semiology to help differentiate between REM and NREM parasomnias • Appreciate the ICSD III Classification Scheme for the major parasomnias • Understand management modalities including behavioral and pharmacological for NREM and REM parasomnias • Understand the difference between parasomnias and seizures WHAT ARE PARASOMNIAS? Undesirable motor, or verbal phenomena that arise from sleep or sleep-wake transition PARASOMNIAS: OVERLAPPING STATES REM PARASOMNIAS WAKE NREM PARASOMNIAS REM NREM PARASOMNIAS: DIFFERENTIAL DIAGNOSIS RBD Confusional Arousals Recurrent Isolated Sleep Paralysis Sleepwalking Nightmare Disorder Sleep Terrors WAKE Sleep Related Eating Disorder REM NREM PYSCHOGENIC SEIZURES SPELLS NFLE Dissociative Disorder ICSD II ICSD III REM Parasomnias • RBD • RBD • Recurrent Isolated Sleep • Recurrent Isolated Sleep Paralysis ICSD II VS ICSDParalysis III CLASSIFICATION• Nightmare Disorder • Nightmare Disorder Disorders of arousal • Confusional Arousals • Confusional Arousals (NREM sleep) • Sleepwalking • Sleep Walking • Sleep Terrors • Sleep Terrors • SRED Other Parasomnias • SRED • Sleep Related Dissociative • Sleep Related Dissociative Disorders Disorders • Sleep Enuresis • Sleep Enuresis • Catathrenia SDB • Catathrenia • Exploding Head Syndrome • Exploding Head syndrome • Sleep Related Hallucinations • Sleep Related Hallucinations • Parasomnia, Unspecified • Parasomnia, Unspecified • Parasomnia due to Drug or • Parasomnia -

What Every Clinician Should Know About Polysomnography
What Every Clinician Should Know About Polysomnography Susheel P Patil MD PhD Introduction Electrical Concepts Current, Voltage, Resistance Capacitance, Inductance, and Impedance Differential Amplifiers Polarity Common Mode Rejection Amplifier Gain, Sensitivity, and Type Patient Ground, Electrical Ground, and Electrical Safety Filters and Filtering Low-Frequency Filters High-Frequency Filters Notch Filters Aspects Unique to Digital Polysomnography Sampling Rate and Aliasing Bit Resolution and Input Voltage Monitor Aliasing Artifacts Updates in Polysomnography Scoring Visual Rules for Sleep Changes in the Scoring of Sleep Under the AASM Manual Comparison of the AASM Manual and R&K Sleep Staging Rules Scoring Reliability of Sleep Staging Under the AASM Manual Scoring of Arousals Movement Rules Scoring of Respiratory Events Summary Polysomnography studies are an essential tool for the sleep physician and aid in the diagnosis and treatment of sleep disorders. Polysomnography refers to the recording, analysis, and interpretation of multiple physiologic signals collected simultaneously. Rapid advancements in technology have transformed the field from a time when analog studies were collected on paper to computer-assisted collection of digitally transformed studies. Sleep clinicians, whether physicians, respiratory thera- pists, or sleep technologists, must therefore have an understanding of a broad array of principles underlying the collection of the various signals. In addition, an understanding of basic technical rules in the evaluation of polysomnography studies is necessary for both the scoring and interpre- tation of such studies. The American Academy of Sleep Medicine published a new manual for the scoring of sleep and associated events in 2007. These changes included modifications to the visual scoring of sleep, the scoring of sleep-disordered breathing events, and movement disorders during sleep. -
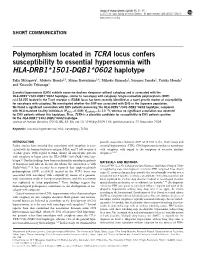
Polymorphism Located in TCRA Locus Confers Susceptibility to Essential Hypersomnia with HLA-DRB1&Ast;1501-DQB1&Ast;0602
Journal of Human Genetics (2010) 55, 63–65 & 2010 The Japan Society of Human Genetics All rights reserved 1434-5161/10 $32.00 www.nature.com/jhg SHORT COMMUNICATION Polymorphism located in TCRA locus confers susceptibility to essential hypersomnia with HLA-DRB1*1501-DQB1*0602 haplotype Taku Miyagawa1, Makoto Honda2,3, Minae Kawashima1,4, Mihoko Shimada1, Susumu Tanaka2, Yutaka Honda3 and Katsushi Tokunaga1 Essential hypersomnia (EHS) exhibits excessive daytime sleepiness without cataplexy and is associated with the HLA-DRB1*1501-DQB1*0602 haplotype, similar to narcolepsy with cataplexy. Single-nucleotide polymorphism (SNP) rs1154155 located in the T-cell receptor a (TCRA) locus has been recently identified as a novel genetic marker of susceptibility for narcolepsy with cataplexy. We investigated whether the SNP was associated with EHS in the Japanese population. We found a significant association with EHS patients possessing the HLA-DRB1*1501-DQB1*0602 haplotype, compared À4 with HLA-matched healthy individuals (Pallele¼0.008; Ppositivity¼5Â10 ), whereas no significant association was observed for EHS patients without this haplotype. Thus, TCRA is a plausible candidate for susceptibility to EHS patients positive for the HLA-DRB1*1501-DQB1*0602 haplotype. Journal of Human Genetics (2010) 55, 63–65; doi:10.1038/jhg.2009.118; published online 20 November 2009 Keywords: essential hypersomnia; HLA; narcolepsy; TCRA INTRODUCTION possible association between SNP rs1154155 in the TCRA locus and Earlier studies have revealed that narcolepsy with cataplexy is asso- essential hypersomnia (EHS), CNS hypersomnia similar to narcolepsy ciated with the human leukocyte antigen (HLA) and T-cell receptor a with cataplexy, with regard to the symptom of excessive daytime (TCRA) genes. -

The Battle Is Not Over Until It Is Won
HUMAN AFRICAN TRYPANOSOMIASIS SLEEPING SICKNESS The battle is not over until it is won Sleeping sickness, or human African trypa- melarsoprol. The latter, however, is still the nosomiasis, threatens millions of people in first-line treatment for the less commonT.b. 36 countries across sub-Saharan Africa. The rhodesiense HAT. Democratic Republic of the Congo bears the To contribute to the WHO elimination goal, a brunt, accounting for 83% of all cases. In the ‘test and treat’ strategy that would be imple- 1960s there were less than 5,000 patients mented at the primary healthcare level is on suffering from the disease in the whole of the the horizon, with potential simple oral pills continent. However, the end of the 20th cen- for both the early and late stage as well as tury – with internal conflict, competing health both types of HAT, that are currently in devel- priorities, and decolonization – witnessed a opment, along with new rapid diagnostics, halt in the successful control methods, and which together would remove the need for the number of cases reported rose painful and dangerous lumbar punc- steeply, peaking in 1998 with tures. This would mean that rural over 37,000 cases reported in health centres, rather than hos- that year. Nowadays, thanks pitals, will play an increasingly to the combined efforts of important role, especially as the WHO, National Sleeping number of reported cases con- Sickness Control Pro- tinues to dwindle. grammes, NGOs and other partners, the disease has once more been brought under control, and since 2010 the number of reported cases has fallen below 8,000. -
Diagnostic Testing for Sleep Disorders
Diagnostic Testing for Sleep Disorders LISA CUTCHEN MD ASSISTANT PROFESSOR UNIVERSITY OF NEW MEXICO HOSPITALS SLEEP DISORDERS CENTER NOVEMBER 11, 2016 Objectives of Talk • Describe the most common types of sleep tests • Explain how and why we test for sleep disorders • Briefly review the most common sleep disorders that require testing Diagnostic Tests for Sleep Disorders • Polysomnography (PSG, Sleep Study) • Overnight Oximetry • Actigraphy • Multiple Sleep Latency Test (MSLT) • Maintenance of Wakefulness Test (MWT)f Diagnostic Tests for Sleep Disorders Sleep Test Quality Measured Polysomnography Simultaneous recording of multiple biophysiological signals to study and characterize sleep and sleep disorders. Overnight oximetry Monitor oxygen saturation and heart rate in bed overnight. Actigraphy Measure sleep/wake patterns over long periods of time by monitoring body movements. Multiple Sleep Latency Test Test ability to fall asleep during the day when permitted and whether REM sleep appears earlier than usual. Maintenance of Wakefulness Test Test ability to stay awake with low levels of stimulation without resorting to extraordinary measures. Polysomnography • 4 Levels of Polysomnograms • Conducted during the patient’s Level I Full PSG, in-lab, attended typical sleep time Level II Full PSG, unattended • Varying levels of complexity Partial PSG, ≥4 • # of signals recorded cardiorespiratory Level III simultaneously parameters, unattended, • Whether attended by a sleep typically done at home technologist Partial PSG, 1-2 cardiorespiratory