Pascal Strupler, Director of the Swiss Federal Office of Public Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

EPP Enlarged Group Bureau Meeting EIN SUMMER UNIVERSITY 'EIN: Achievements and Its Role to Play in the Future' EN
EPP Enlarged Group Bureau Meeting EIN SUMMER UNIVERSITY ‘EIN: Achievements and its role to play in the future’ ‘The success of the Political Networking’ 19 June 2014 ALBUFEIRA Service Documentation - Publications Recherche EPP Group Group of the European People’s Party (Christian Democrats) in the European Parliament EN European Ideas Network 2 Vade-mecum of the speakers VADE-MECUM of the Speakers European Ideas Network 3 European Ideas Network 4 Vade-mecum of the speakers Michael BORCHARD, Head of the Department of Politics and Consulting, Konrad-Adenauer-Stiftung (KAS) Michael Borchard is Director of the Department for Policy Consulting, a think tank at the Konrad-Adenauer Foundation in Berlin. Previously, he headed the unit on domestic policy in this department. Before joining the Konrad-Adenauer Foundation, Mr. Borchard served as the Head of the Speech-Writing Division at the State-Chancellery of Thuringia, as senior speech-writer to the Minister-President of Thuringia, Dr. Bernhard Vogel. Prior to this he worked as a member at the team of speech-writers for Chancellor Dr. Helmut Kohl in the office of the Federal Chancellor. His previous work experience includes several years as a freelance journalist as well as researcher for contemporary history. Mr. Borchard holds a Ph.D. in contemporary history and political science from the University of Bonn, Germany. His dissertation on “The German Prisoners of War in the Soviet Union. The political importance of the Prisoner-of-War-Problem for both German States and the Western Allies between 1949 and 1955” was awarded the Geffrub-Prize 1999 from the University of Bonn for the best dissertation. -

2020-Activity-Report.Pdf
— 2020 — WILFRIED MARTENS CENTRE FOR EUROPEAN STUDIES ACTIVITY REPORT © February 2021 - Wilfried Martens Centre for European Studies 2020’s label will unfortunately be, above all, the year of Table of Contents the COVID-19 pandemic. It has marked the fates of many people, the way of life we used to enjoy, the way in which we communicated and worked, and in fact the entire world. On one hand, it has caused unprecedent fear for Welcome 04 human lives, but on the other hand it stimulated signifi- cant ones, such as the great effort to effectively coordi- nate the fight against the virus and the decision to create the Recovery Fund – Next Generation EU. However, we Publications 07 ended the year with the faith that the vaccines humanity European View 08 developed will save human lives and gradually get the Publications in 2020 10 situation under control, also eliminating the pandemic’s devastating impact on the economy. Another sad moment of 2020 for the EU was, of course, the UK’s official exit. It was a very painful process, but Events 13 largely chaotic on the British side. Even though we Events in 2020 14 parted “in an orderly fashion”, the consequences will be Economic Ideas Forum Brussels 2020 16 felt on both sides for years to come. 10th Transatlantic Think Tank Conference 20 Another unquestionably significant event of 2020 was the US presidential election. The pandemic, along with the events surrounding the US election, such as the Common Projects 23 attack on the Capitol, proved how fragile democracy NET@WORK 24 is, as are we. -
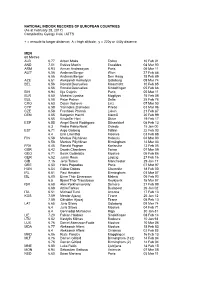
As at February 28, 2017) Compiled by György Csiki / ATFS
NATIONAL INDOOR RECORDS OF EUROPEAN COUNTRIES (As at February 28, 2017) Compiled by György Csiki / ATFS + = enroute to longer distance; A = high altitude; y = 220y or 440y distance MEN 60 Metres ALB 6.77 Arben Maka Torino 10 Feb 01 AND 7.01 Estéve Martin Escaldes 04 Mar 00 ARM 6.93 Arman Andreasyan Paris 05 Mar 11 AUT* 6.56 Andreas Berger Wien 27 Feb 88 6.56 Andreas Berger Den Haag 18 Feb 89 AZE 6.61 Aleksandr Kornelyuk Göteborg 09 Mar 74 BEL 6.56 Ronald Desruelles Maastricht 10 Feb 85 6.56 Ronald Desruelles Sindelfingen 05 Feb 88 BIH 6.94 Ilija Cvijetic Paris 05 Mar 11 BLR 6.60 Maksim Lynsha Mogilyov 15 Feb 08 BUL 6.58 Petar Petrov Sofia 25 Feb 78 CRO 6.63 Dejan Vojnovic Linz 07 Mar 03 CYP 6.58 Yiannakis Zisimides Pireás 03 Mar 96 CZE 6.58 Frantisek Ptácník Liévin 21 Feb 87 DEN 6.65 Benjamin Hecht Malmö 20 Feb 99 6.65 Kristoffer Hari Skive 19 Feb 17 ESP 6.55 Angel David Rodriguez Düsseldorf 08 Feb 13 6.3 Pedro Pablo Nolet Oviedo 15 Jan 00 EST 6.71 Argo Golberg Tallinn 22 Feb 03 6.4 Enn Lilienthal Moskva 03 Feb 88 FIN 6.58 Markus Pöyhönen Helsinki 04 Mar 03 6.58 Markus Pöyhönen Birmingham 14 Mar 03 FRA 6.45 Ronald Pognon Karlsruhe 13 Feb 05 GBR 6.42 Dwain Chambers Torino 07 Mar 09 GEO 6.71 Besik Gotsiridze Moskva 05 Feb 86 GER 6.52 Julian Reus Leipzig 27 Feb 16 GIB 7.16 Jerai Torres Manchester 29 Jan 17 GRE 6.50 Haris Papadiás Paris 07 Mar 97 HUN 6.54 Gábor Dobos Chemnitz 18 Feb 00 IRL 6.61 Paul Hession Birmingham 03 Mar 07 ISL 6.80 Einar Thór Einarsson Malmö 06 Feb 93 6.5 Bjarni Thór Traustason Reykjavík 15 Mar 97 ISR 6.68 Alex Porkhomovskiy -

List of Members
Delegation to the Parliamentary Assembly of the Union for the Mediterranean Members David Maria SASSOLI Chair Group of the Progressive Alliance of Socialists and Democrats in the European Parliament Italy Partito Democratico Asim ADEMOV Member Group of the European People's Party (Christian Democrats) Bulgaria Citizens for European Development of Bulgaria Alex AGIUS SALIBA Member Group of the Progressive Alliance of Socialists and Democrats in the European Parliament Malta Partit Laburista François ALFONSI Member Group of the Greens/European Free Alliance France Régions et Peuples Solidaires Malik AZMANI Member Renew Europe Group Netherlands Volkspartij voor Vrijheid en Democratie Nicolas BAY Member Identity and Democracy Group France Rassemblement national Tiziana BEGHIN Member Non-attached Members Italy Movimento 5 Stelle François-Xavier BELLAMY Member Group of the European People's Party (Christian Democrats) France Les Républicains Sergio BERLATO Member European Conservatives and Reformists Group Italy Fratelli d'Italia Manuel BOMPARD Member The Left group in the European Parliament - GUE/NGL France La France Insoumise 24/09/2021 1 Sylvie BRUNET Member Renew Europe Group France Mouvement Démocrate Jorge BUXADÉ VILLALBA Member European Conservatives and Reformists Group Spain VOX Catherine CHABAUD Member Renew Europe Group France Mouvement Démocrate Nathalie COLIN-OESTERLÉ Member Group of the European People's Party (Christian Democrats) France Les centristes Gilbert COLLARD Member Identity and Democracy Group France Rassemblement national -

2018 World Indoor Championships Statistics - Women’S HJ - by K Ken Nakamura Summary Page
2018 World Indoor Championships Statistics - Women’s HJ - by K Ken Nakamura Summary Page: All time Performance List at the World Indoor Championships Performance Performer Height Name Nat Pos Venue Year 1 1 2.05 Stefka Kostadinova BUL 1 Indianapolis 19 87 2 2 2.04 Yelena Slesarenko RUS 1 Budapest 2004 3 3 2.03 Blanka Vlasic CRO 1 Valencia 2008 4 4 2.02 Susanne Beyer GDR 2 Indianapolis 1987 4 2.02 Stefka Kostadinova 1 Budapest 1989 4 2.02 Stefka Kostadinova 1 Toronto 1993 4 4 2.02 Heike Henkel GER 2 Toronto 1993 4 2.02 Stefka Kostadinova 1 Paris 1997 4 2.02 Yelena Slesarenko 1 Moskva 2006 Lowest winning Height: 1.96m by Vashti Cunningham (USA) in 2016 is the lowest winning Height in history. 1.98m by Chaunte Lowe (USA) in 2012 is the second lowest winning height in the history of the World Indoor; 1.99m by Khristina Kalcheva (BUL) in 1999 is the third lowest winning height; 1.97m by Stefka Kostadinova in 1985 World Indoor Games is even lower. Margin of Victory Difference Height Name Nat Venue Year Max 4cm 2.04m Yelena Slesarenko RUS Budapest 2004 Min 0cm 2.02m Stefka Kostadinova BUL Toronto 1993 2.00m Kajsa Bergqvist UKR Lisboa 2001 1.96m Vasti Cunningham USA Portland 2016 Best Marks for Places in the World Indoor Championships Pos Height Name Nat Venue Year 1 2.05 Stefka Kostadinova BUL Indianapolis 1987 2 2.02 Susanne Beyer GDR Indianapolis 1987 Heike Henkel GER Toronto 1993 2.01 Yelena Slesarenko RUS Valencia 2008 3 2.01 Vita Palamar UKR Valencia 2008 4 1.99 Ruth Beitia ESP Valencia 2008 Multiple Gold Medalists: Blanka Vlasic (CRO): -
Official Directory of the European Union
ISSN 1831-6271 Regularly updated electronic version FY-WW-12-001-EN-C in 23 languages whoiswho.europa.eu EUROPEAN UNION EUROPEAN UNION Online services offered by the Publications Office eur-lex.europa.eu • EU law bookshop.europa.eu • EU publications OFFICIAL DIRECTORY ted.europa.eu • Public procurement 2012 cordis.europa.eu • Research and development EN OF THE EUROPEAN UNION BELGIQUE/BELGIË • БЪЛГАРИЯ • ČESKÁ REPUBLIKA • DANMARK • DEUTSCHLAND • EESTI • ΕΛΛΑΔΑ • ESPAÑA • FRANCE • ÉIRE/IRELAND • ITALIA • ΚΥΠΡΟΣ/KIBRIS • LATVIJA • LIETUVA • LUXEMBOURG • MAGYARORSZÁG • MALTA • NEDERLAND • ÖSTERREICH • POLSKA • PORTUGAL • ROMÂNIA • SLOVENIJA • SLOVENSKO • SUOMI/FINLAND • SVERIGE • UNITED KINGDOM • BELGIQUE/BELGIË • БЪЛГАРИЯ • ČESKÁ REPUBLIKA • DANMARK • DEUTSCHLAND • EESTI • ΕΛΛΑ∆Α • ESPAÑA • FRANCE • ÉIRE/IRELAND • ITALIA • ΚΥΠΡΟΣ/KIBRIS • LATVIJA • LIETUVA • LUXEMBOURG • MAGYARORSZÁG • MALTA • NEDERLAND • ÖSTERREICH • POLSKA • PORTUGAL • ROMÂNIA • SLOVENIJA • SLOVENSKO • SUOMI/FINLAND • SVERIGE • UNITED KINGDOM • BELGIQUE/BELGIË • БЪЛГАРИЯ • ČESKÁ REPUBLIKA • DANMARK • DEUTSCHLAND • EESTI • ΕΛΛΑΔΑ • ESPAÑA • FRANCE • ÉIRE/IRELAND • ITALIA • ΚΥΠΡΟΣ/KIBRIS • LATVIJA • LIETUVA • LUXEMBOURG • MAGYARORSZÁG • MALTA • NEDERLAND • ÖSTERREICH • POLSKA • PORTUGAL • ROMÂNIA • SLOVENIJA • SLOVENSKO • SUOMI/FINLAND • SVERIGE • UNITED KINGDOM • BELGIQUE/BELGIË • БЪЛГАРИЯ • ČESKÁ REPUBLIKA • DANMARK • DEUTSCHLAND • EESTI • ΕΛΛΑΔΑ • ESPAÑA • FRANCE • ÉIRE/IRELAND • ITALIA • ΚΥΠΡΟΣ/KIBRIS • LATVIJA • LIETUVA • LUXEMBOURG • MAGYARORSZÁG • MALTA • NEDERLAND -

Republic of Slovenia
Office for Democratic Institutions and Human Rights REPUBLIC OF SLOVENIA PRESIDENTIAL ELECTION 22 OCTOBER 2017 OSCE/ODIHR Election Expert Team Final Report Warsaw 20 December 2017 TABLE OF CONTENTS I. EXECUTIVE SUMMARY ................................................................................................................. 1 II. INTRODUCTION AND ACKNOWLEDGMENTS ........................................................................ 1 III. BACKGROUND AND POLITICAL CONTEXT ............................................................................ 2 IV. LEGAL FRAMEWORK ..................................................................................................................... 3 V. PARTY AND CAMPAIGN FINANCE ............................................................................................. 5 A. FUNDING SOURCES ....................................................................................................................... 5 B. CAMPAIGN EXPENDITURE ............................................................................................................ 6 C. DISCLOSURE AND REPORTING ..................................................................................................... 6 D. OVERSIGHT ................................................................................................................................... 7 VI. RECOMMENDATIONS .................................................................................................................... 8 A. PRIORITY RECOMMENDATIONS ................................................................................................. -

Bundesrat Unterrichtung
Bundesrat Drucksache 558/09 04.06.09 Unterrichtung durch das Europäische Parlament Erklärung des Europäischen Parlaments zur Unterstützung von Special Olympics in der Europäischen Union _________________________________________________________________ Zugeleitet mit Schreiben des Generalsekretärs des Europäischen Parlaments - 107274 - vom 2. Juni 2009. Das Europäische Parlament hat die Entschließung in der Sitzung am 5. Mai 2009 angenommen. Vertrieb: Bundesanzeiger Verlagsgesellschaft mbH, Amsterdamer Str. 192, 50735 Köln Telefon: (02 21) 97 66 83 40, Telefax: (02 21) 97 66 83 44 ISSN 0720-2946 Drucksache 558/09 - 2 - Erklärung des Europäischen Parlaments zur Unterstützung von Special Olympics in der Europäischen Union Das Europäische Parlament, – gestützt auf Artikel 116 seiner Geschäftsordnung, A. in der Erwägung, dass Special Olympics in Europa Erwachsenen und Jugendlichen mit geistigen Behinderungen sportliche und gesellschaftliche Möglichkeiten bietet, B. in der Erwägung, dass Special Olympics in allen Mitgliedstaaten etabliert ist und eine halbe Million Athleten umfasst, C. in der Erwägung, dass Special Olympics jeden Tag EU-Politik umsetzt, indem Sport und ehrenamtliche Tätigkeit grenzüberschreitend gefördert, Vorurteile über Behinderungen abgebaut, die Volksgesundheit unterstützt und Randgruppen in gesellschaftliche Aktivitäten eingebunden werden, D. in der Erwägung, dass Special Olympics in Europa in den kommenden Jahren zwei große Veranstaltungen ausrichten wird: 2010 die Europäischen Special Olympics Sommerspiele in Warschau -

En En Minutes
European Parliament 2019-2024 Committee on the Environment, Public Health and Food Safety ENVI_PV(2020)0928_1 MINUTES Meeting of 28 September 2020, 13.45-15.45 BRUSSELS The meeting opened at 13.55 on Monday, 28 September 2020, with Pascal Canfin (Chair) presiding. 1. Adoption of agenda ENVI_OJ(2020)0928_1 The agenda was adopted in the form shown in these minutes. 2. Chair's announcements The Chair made the following announcements: Interpretation status: due to scarcity of resources and technical restrictions in the meeting room and based on the linguistic profile of ENVI Members, interpretation was available in 6 languages: French, German, Italian, English, Spanish and Polish. Electronic meeting file/Webstreaming: The Chair announced that as usual, the meeting file was available electronically via the e-meeting application and that the meeting would be web streamed. Remote participation of ENVI Members: The Chair announced that the meeting would be held in a remote participation format. At 15.45, the remote voting session opened. Members taking part in the vote had received a ballot paper- voting list that needed to be signed and sent back with the voting indications PV\1217944EN.docx PE660.271v01-00 EN United in diversityEN before 17.45. The results of the votes on the amendments would be announced in writing. Information on the outcome on the budget amendments : The Chair informed that during the voting session on 21 September 2020, ENVI had voted on the amendments to the "General budget of the European Union for the financial year 2021 - all sections". The list of the adopted amendments could be found on the website. -
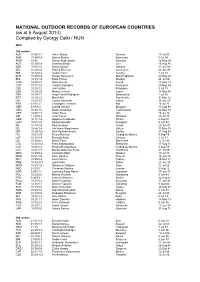
(As at 6 August 2014) Compiled by György Csiki / HUN
NATIONAL OUTDOOR RECORDS OF EUROPEAN COUNTRIES (as at 6 August 2014) Compiled by György Csiki / HUN MEN 100 metres: ALB 10.56/1.1 Arben Makaj Donnas 15 Jul 03 AND 10.94/0.9 Esteve Martin Barcelona 5 Jul 00 ARM 10.45 Arman Andreasyan Artashat 16 May 09 AUT 10.15/0.9 Andreas Berger Linz 15 Aug 88 AZE 10.08/1.3 Ramil Guliyev Istanbul 13 Jun 09 BEL 10.14/1.0 Patrick Stevens Oordegem 28 Jun 97 BIH 10.42/0.2 Nedim Covic Velenje 1 Jul 10 BLR 10.27/0.9 Sergey Kornelyuk Biala Podlaska 28 May 94 BUL 10.13/1.4 Petar Petrov Moskva 24 Jul 80 CRO 10.20/1.5 Dario Horvat Azusa 11 May 13 CYP 10.11/1.5 Yiannis Zisimides Rethymno 25 May 96 CZE 10.23/1.0 Jan Veleba Pardubice 3 Jul 10 DEN 10.29/2.0 Morten Jensen Greve 18 Sep 04 ESP 10.14/1.7 Angel David Rodriguez Salamanca 2 Jul 08 EST 10.19/1.5 Marek Niit Fayetteville 31 Mar 12 FIN 10.21/0.5 Tommi Hartonen Vaasa 23 Jun 01 FRA 9.92/2.0 Christophe Lemaitre Albi 29 Jul 11 GBR 9.87/0.3 Linford Christie Stuttgart 15 Aug 93 GEO 10.35/1.5 Besik Gotsiridze Tsakhkadzor 22 May 87 GER 10.05/1.8 Julian Reus Ulm 26 Jul 14 GIB 11.27/0.2 Jerai Torres Hamilton 15 Jul 13 GRE 10.11/1.4 Aggelos Pavlakakis Athína 2 Aug 97 HUN 10.08/1.0 Roland Németh Budapest 9 Jun 99 IRL 10.18/1.9 Paul Hession Vaasa 23 Jun 07 ISL 10.56/1.4 Jón Arnar Magnússon Götzis 31 May 97 ISR 10.20/-0.6 Alex Porkhomovskiy Sevilla 21 Aug 99 ITA 10.01/0.9 Pietro Mennea Ciudad de México 4 Sep 79 LAT 10.18/1.4 Ronalds Arajs Donnas 3 Jul 11 LIE 10.53/0.6 Martin Frick Bellinzona 12 Jul 96 LTU 10.14/-0.2 Rytis Sakalauskas Shenzhen 17 Aug 11 LUX 10.41/0.2 Roland -

Steht Später Die Headline
VORWAHLBERICHT Konrad-Adenauer-Stiftung e.V. KROATIEN DR. MICHAEL A. LANGE 13. Mai 2014 Slowenien vor den Europawahlen 2014 www.kas.de/kroatien Am 1. Mai 2014 jährt sich der EU-Beitritt Weltkrieg verlassen mussten. Im Rahmen Sloweniens zum zehnten Mal und in wenigen des sog. »Solana Kompromisses« wurde es Wochen -genau genommen am 25. Mai 2014- allen ehemals in Slowenien ansässigen EU werden in Slowenien ein weiteres nunmehr Bürgern erlaubt, Immobilien zu erwerben. drittes Mal seine acht Vertreter für das Euro- päische Parlament bestimmen. Die Wahlen Nach dem Start der Beitrittsverhandlungen werden dabei just am „Tag der Jugend“ im Jahre 1998 konnten diese bereits im stattfinden, jenem Feiertag aus jugosla- Herbst 2002 abgeschlossen werden, so dass wischer Zeit, als Hunderttausende Titos der EU Beitrittsvertrag schließlich bereits im Geburtstag zelebrierten.1 Dabei war 25. Folgejahr unterzeichnet werden konnte. Mai nicht wirklich Titos Geburtstag, son- Obwohl einige EU Mitgliedstaaten die Frei- dern sollte (ihn) an den 25. Mai 1944 er- zügigkeit von Arbeitnehmern auch aus Slo- innern, als Tito einem Angriff deutscher wenien für einige Jahre einschränkte, nahm Fallschirmjäger (Operation Rösselsprung) die Auswanderung von Slowenen erst mit auf sein Versteck in Drvar nur knapp ent- dem Beginn der Wirtschaftskrise deutlich kommen war. zu. 10 Jahre EU Mitgliedschaft Sloweniens Nach Einführung des Euro im Jahre 2007 und dem Beitritt zum Schengen Raum im Slowenien gehörte damals zu den ersten gleichen Jahr, stellte das neue EU- ex-kommunistischen Staaten, die der Union Mitgliedsland Slowenien schon in seiner ers- beitraten und galt lange Jahre als Erfolgs- ten EU Ratspräsidentschaft im ersten Halb- story. Zuletzt musste jedoch auch Slowe- jahr 2008 seine Ernsthaftigkeit und Bei- nien der Wirtschafts- und Finanzkrise in Eu- trittsreife unter Beweis. -

2014 European Championships Statistics – Women's 100M
2014 European Championships Statistics – Women’s 100m by K Ken Nakamura All time performance list at the European Championships Performance Performer Time Wind Name Nat Pos Venue Year 1 1 10.73 2.0 Christine Arron FRA 1 Budapest 1998 2 10.81 1.3 Christine Arron 1sf1 Budapest 1998 3 2 10.83 2.0 Irina Privalova RUS 2 Budapest 1998 4 3 10.87 2.0 Ekaterini Thanou GRE 3 Budapest 1998 5 4 10.89 1.8 Katrin Krabbe GDR 1 Split 1990 6 5 10.91 0.8 Marlies Göhr GDR 1 Stuttgart 1986 7 10.92 0.9 Ekaterini Thanou 1sf2 Budapest 1998 7 6 10.92 2.0 Zhanna Pintusevich -Block UKR 4 Budapest 1998 9 10.98 1.2 Marlies Göhr 1sf2 Stuttgart 1986 10 11.00 1.3 Zhanna Pintusevich -Block 2sf1 Budapest 1998 11 11.01 -0.5 Marlies Göhr 1 Athinai 1982 11 11.01 0.9 Zhanna Pintusevich -Block 1h2 Helsinki 1994 13 11.02 0.6 Irina Privalova 1 Helsinki 1994 13 11.02 0.9 Irina Privalova 2sf2 Budapest 1998 15 7 11.04 0.8 Anelia Nuneva BUL 2 Stuttgart 1986 15 11.04 0.6 Ekaterini Thanou 1h4 Budapest 1998 17 8 11.05 1.2 Silke Gladisch -Möller GDR 2sf2 Stuttgart 1986 17 11.05 0.3 Ekaterini Thanou 1sf2 München 2002 19 11.06 -0.1 Marlies Göhr 1h2 Stuttgart 1986 19 11.06 -0.8 Zhanna Pintusevich -Block 1h1 Budapest 1998 19 9 11.06 1.8 Kim Gevaert BEL 1 Göteborg 2006 22 10 11.06 1.7 Ivet Lalova BUL 1h2 Helsinki 2012 22 11.07 0.0 Katrin Krabbe 1h1 Split 1990 22 11 11.07 2.0 Melanie Paschke GER 5 Budapest 1998 25 11.07 0.3 Ekaterini Thanou 1h4 München 2002 25 11.08 1.2 Anelia Nuneva 3sf2 Stuttga rt 1986 27 12 11.08 0.8 Nelli Cooman NED 3 Stuttgart 1986 28 11.09 0.8 Silke Gladisch -Möller