Psychiatry As a Tool for Coercion in Post-Soviet Countries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
LINKING INFECTIOUS and NARCOLOGY CARE) Evidence-Based for Engagement in HIV Care
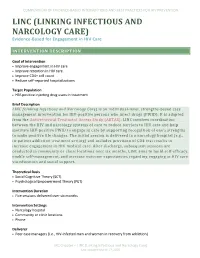
COMPENDIUM OF EVIDENCE-BASED INTERVENTIONS AND BEST PRACTICES FOR HIV PREVENTION LINC (LINKING INFECTIOUS AND NARCOLOGY CARE) Evidence-Based for Engagement in HIV Care INTERVENTION DESCRIPTION Goal of Intervention • Improve engagement in HIV care • Improve retention in HIV care • Improve CD4+ cell count • Reduce self-reported hospitalizations Target Population • HIV-positive injecting drug users in treatment Brief Description LINC (Linking Infectious and Narcology Care) is an individual-level, strengths-based case management intervention for HIV-positive persons who inject drugs (PWID). It is adapted from the Antiretroviral Treatment Access Study (ARTAS). LINC involves coordination between the HIV and narcology systems of care to reduce barriers to HIV care and help motivate HIV-positive PWID to engage in care by supporting recognition of one’s strengths to make positive life changes. The initial session is delivered in a narcology hospital (e.g., in-patient addiction treatment setting) and includes provision of CD4 test results to increase engagement in HIV medical care. After discharge, subsequent sessions are conducted in community or clinic locations over six months. LINC aims to build self-efficacy, enable self-management, and increase outcome expectancies regarding engaging in HIV care via education and social support. Theoretical Basis • Social Cognitive Theory (SCT) • Psychological Empowerment Theory (PET) Intervention Duration • Five sessions delivered over six months Intervention Settings • Narcology hospital • Community or clinic locations • Phone Deliverer • Peer case managers (i.e., HIV-infected men and women in recovery from addiction) LRC Chapter – LINC (Linking Infectious and Narcology Care) Last updated March 17, 2020 COMPENDIUM OF EVIDENCE-BASED INTERVENTIONS AND BEST PRACTICES FOR HIV PREVENTION Delivery Methods • Case management • Printed materials • Discussion • Video • Goal setting Structural Components There are no reported structural components reported for this study. -

Eugenics, Nazi and Soviet Psychiatry Jason Luty
Advances in psychiatric treatment (2014), vol. 20, 52–60 doi: 10.1192/apt.bp.112.010330 ARTICLE Psychiatry and the dark side: eugenics, Nazi and Soviet psychiatry Jason Luty Jason Luty is consultant in restrict liberty, that tends towards abuse if not SUMMARY addictions psychiatry at Borders regulated by the legal or political system. In the Health. He has published in the Psychiatrist Thomas Szasz fought coercion past, there have been abuses of psychiatrists’ addictions field and trained at (compulsory detention) and denied that mental the Maudsley Hospital, London powers to detain people, but these have been illness existed. Although he was regarded as a and spent 8 years as consultant instigated at the direction of governments such maverick, his ideas are much more plausible when in addictions at the South Essex as that in Nazi Germany (leading to genocide of Partnership University NHS one discovers that between 1939 and 1941, up to Foundation Trust. He has a PhD in 100 000 mentally ill people, including 5000 children, mentally ill people) and the USSR (where political pharmacology following a study were killed in Nazi Germany. In the course of the dissidents were detained with a diagnosis of of the molecular mechanisms Nazi regime, over 400 000 forced sterilisations took ‘sluggish schizophrenia’). of receptor desensitisation and place, mainly of people with mental illnesses. Other tolerance. He is a wobbly member of the English Conservative Party. countries, including Denmark, Norway, Sweden Psychiatry and eugenics and Switzerland, had active forced sterilisation Correspondence Dr Jason Luty, The science of eugenics emerged during the Borders Addiction Service, The programmes and eugenics laws. -

The Ukrainian Weekly 1987
ТаІИНPublishtd by tht Ukrainian National A5sociation Inc.. a fraternal non-profit associationу| Vol. LV No.9 THE UKRAINIAN WEEKLY SUNDAY, MARCH 1.1987 25 cent5 Treblinka survivors' testimony begins Gen. Petro Grigorenko dies NEW YORK - Petro Hryhorovych in Demjanjui( trial's second week Grigorenko, a founding member of Special to Svoboda and The Weekly said, wore black uniforms, while the both the Moscow and Ukrainian Hel Germans were dressed in green. He sinki monitoring groups, and a former JERUSALEM - Two survivors of recalled his experiences in the camp Red Army general, died here at Beth the Treblinka death camp testified this dramatically and emotionally as he had Israel Hospital on Saturday, February week at the war crimes trial of John done in German and American courts, 21. He was 79. Demjanjuk, and both identified the at legal proceedings against, among A tireless defender of human and retired autoworker as "Ivan of Tre others, Feodor Fedorenko and Mr. national rights until his death, Gen. blinka" in dramatic appearances. Demjanjuk. Grigorenko was confined for nearly six During cross-examination of both Mr. Epstein pointed at Mr. Demjan years (1963-1964, 1969-1974) in Soviet witnesses, the defense pointed out juk and shouted, "This is the man, the psychiatric hospitals in retaliation for inconsistencies in each witness's own man sitting over there," in identifying such activities. testimony given at various times as well him as a guard at Treblinka named In 1978, while in the United States for as discrepancies between the testimo Ivan. Some of the spectators at the trial medical treatment, he was stripped of nies of both men. -

Boletin De Documentación Nº 37, Marzo De 2009
Su elaboración en formato electrónico, iniciada en julio de 2002, ha supuesto importantes ventajas de cara a ampliar y agilizar su difusión entre los profesionales del sector, permitiendo asimismo la localización de documentación relevante por parte de cualquier ciudadano interesado en el campo de las drogodependencias. Como en los números anteriores, en el boletín de marzo se recogen las principales novedades bibliográficas que, sobre los distintos aspectos relacionados con las adicciones, han tenido entrada en el Centro de Documentación e Información de la Delegación del Gobierno para el Plan Nacional sobre Drogas en los tres últimos meses. El contenido del Boletín está estructurado en tres grandes epígrafes: Novedades bibliográficas (clasificadas por su temática y con indicación de su ruta en el caso de que estén disponibles a texto completo en Internet), Legislación y Sumarios de revistas. Esperamos que el Boletín, cuya difusión se realiza a través de listas de distribución de correo electrónico y de su presencia permanente en la página web de la Delegación del Gobierno para el Plan Nacional sobre Drogas, sea de interés y quedamos a la espera de cualquier sugerencia y/o consulta que sobre el mismo queráis formular. Ministerio de Sanidad y Consumo. Delegación del Gobierno para el Plan Nacional sobre Drogas José del Val – E-correo: [email protected] Jefe de Servicio del Centro de Documentación e Información 1 Aspectos Generales ........................................................................ 4 Aspectos Sociales ............................................................................ -

Use of the Communication Checklist
Psychiatria Danubina, 2020; Vol. 32, Suppl. 1, pp 88-92 Conference paper © Medicinska naklada - Zagreb, Croatia USE OF THE COMMUNICATION CHECKLIST - SELF REPORT (CC-SR) IN SCHIZOPHRENIA: LANGUAGE IMPAIRMENTS CORRELATE WITH POOR PREMORBID SOCIAL ADJUSTMENT Daria Smirnova1,2, Svetlana Zhukova3, Olga Izmailova4, Ilya Fedotov5, Yurii Osadshiy6, Alexander Shustov7, Anna Spikina8, Dmitriy Ubeikon9, Anna Yashikhina2, Natalia Petrova10, Johanna Badcock1, Vera Morgan1 & Assen Jablensky1 1Centre for Clinical Research in Neuropsychiatry, University of Western Australia, Perth, Australia 2Department of Psychiatry, Narcology, Psychotherapy and Clinical Psychology, Samara State Medical University, Samara, Russia 3Department of Psychiatry, Narcology and Psychology, Ivanovo State Medical Academy, Ivanovo, Russia 4Samara District Clinical Psychiatric Hospital, Samara, Russia 5Department of Psychiatry, Ryazan State Medical University n.a. academician I.P. Pavlov, Ryazan, Russia 6Department of Psychiatry, Narcology and Medical Psychology, Rostov State Medical University, Rostov-on-Don, Russia 7National Medical Research Centre of Psychiatry and Narcology n.a. V.P. Serbsky, Moscow, Russia 8Psychoneurological dispensary ʋ2, Saint Petersburg, Russia 9Department of Psychiatry, Narcology and Psychotherapy with the course of General and Medical psychology, S.I. Georgievsky Medical Academy, V.I. Vernadsky Crimean Federal University, Simferopol, Republic of Crimea, Russia 10Department of Psychiatry and Narcology, Saint Petersburg State University, Saint Petersburg, -

Workbook Psychiatry and Narcology
Kharkiv National Medical University Department of Psychiatry, Narcology and Medical Psychology WORKBOOK MANUAL FOR INDIVIDUAL WORK FOR MEDICAL STUDENTS PSYCHIATRY AND NARCOLOGY (Part 2) Student ___________________________________________________________ Faculty _________________________________________________________ Course _________________ Group _____________________________________ Kharkiv 2019 Затверджено вченою радою ХНМУ Протокол №5 від 23.05.2019 р. Psychiatry (Part 2) : workbook manual for individual work of students / I. Strelnikova, G. Samardacova, К. Zelenska – Kharkiv, 2019. – 103 p. Копіювання для розповсюдження в будь-якому вигляді частин або повністю можливо тільки з дозволу авторів навчального посібника. CLASS 7. NEUROTIC DISORDERS. CLINICAL FORMS. TREATMENT AND REHABILITATION. POSTTRAUMATIC STRESS DISORDER. TREATMENT AND REHABILITATION. Psychogenic diseases are a large and clinically varied group of diseases resulting from an effect of acute or long-term psychic traumas, which manifest themselves by both mental and somatoneurological disorders and, as a rule, are reversible. Psychogenic diseases are caused by a psychic trauma, i.e. some events which affect significant aspects of existence of the human being and result in deep psychological feelings. These may be subjectively significant events, i.e. those which are pathogenic for the majority of people. Besides, the psyche may be traumatized by conventionally pathogenic events, which cause feelings in an individual because of his peculiar hierarchy of values. Unfavorable psychogenic effects on the human being cause stress in him, i.e. a nonspecific reaction at the physiological, psychological and behavioural levels. Stress may exert some positive, mobilizing influence, but may result in disorganization of the organism activity. The stress, which exerts a negative influence and causes various disturbances and even diseases, is termed distress. Classification of neurotic disorders I. -

WCP 2020 Programme at a Glance Website.Xlsx
ALL TIMES ARE IN ICT (INDOCHINA TIME - GMT+7) Legend Plenary / Presidential Session Special Sessions COVID-19 Session Special Lectures Original Sessions Invited Symposia Lectures in Thai Courses Panel Discussions Company Supported Sessions Interorganizational Symposia Tuesday, 9 March 2021 Time in Bangkok Time in CET Hall A 14:30-17:30 08:30-11:30 Course 01: Assessment and treatment of personality disorders Andrew Chanen, Australia 18:30-21:30 12:30-15:30 Course 02: Mindfulness based therapy and counseling (MBTC) developed from Thailand Wongpiromsarn Yongyud, Thailand Wednesday, 10 March 2021 Time in Bangkok Time in CET Hall A Hall B Hall C Hall D Hall E Hall F Hall G Hall H 16:00-16:30 10:00-10:30 **By invitation only** Meet the Fellowship Awardees Afzal Javed - WPA President Helen Herrman - WPA Past President Norman Sartorius - WCP 2020 Scientific Chairperson Mariana Pinto da Costa - WCP 2020 ECP Chairperson 18:00-18:45 12:00-12:45 Opening Ceremony and Plenary Session 01 (Presidents' Reports) Master of ceremonies - calling the meeting to order Andrea Pound, Australia Thai Psychiatric Society Address Charnsil Chawanun, Thailand Address from Helen Herrman - WPA Past President Address from Afzal Javed - WPA President Norman Sartorius - Introduction to the program Afzal Javed - Declaring the congress open 18:45-19:15 12:45-13:15 BREAK 19:15-20:15 13:15-14:15 Plenary Session 02: Global health and global mental health: a dream too far? Chairs: Helen Herrman, Australia; Nawaporn Hirunviwatgul, Thailand Speaker: Richard Horton, UK Discussants: -

Curriculum Vitae
CURRICULUM VITAE Prof. Robert van Voren PhD FRCPsych (Hon) (pseudonym of Johannes Bax) Personal information Address: a. Totoriu 20-6, 21011 Vilnius, Lithuania b. Graaf Floris V weg 37-62, 3739 NC Hollandsche Rading (NL) tel.: +31-651534123 (mob.) Postal address: P.O.Box 1956, 1200 BZ Hilversum (NL) E-mail: [email protected] Date/place of birth: July 25, 1959, Montréal (Canada) Nationality: Canadian, Dutch, Lithuanian Civil status: married, 3 children Education • Marnix Gymnasium, Rotterdam (The Netherlands). Graduation 1979. • Modern and Theoretical History, University of Amsterdam; specialization in Soviet History, with Russian language. Graduation 1986. Degree: doctorandus (drs), comparable with MSc. • PhD in political science at Kaunas Vytautas Magnus University, October 2010. Languages • Dutch (native) • English (second native language) • Russian (fluent) • German (fluent) • French (good) • Lithuanian (poor) • Italian (poor) Current paid positions: • Chief Executive, Human Rights in Mental Health – FGIP • Professor of Soviet and Post-Soviet Studies, Vytautas Magnus University, Kaunas (LT) • Executive Director of the Andrei Sakharov Research Center on Democratic Development, Kaunas (LT) • Professor of Soviet and Post-Soviet Studies, Ilia State University (GEO) Curriculum vitae Johannes Bax – Robert van Voren 1 Professional activity 1978-1987: Secretary of the Podrabinek Fund in The Netherlands. 1978-1989: Associate of the Bukovsky Foundation in Amsterdam, The Netherlands. 1980: Founding member of the International Association on the Political use of Psychiatry (IAPUP) 1980-1990: Traveled on average four times per year to the USSR to meet with dissidents and relatives of political prisoners. The goals of these trips were to deliver humanitarian aid, to collect evidence on human rights violations and smuggle this and samizdat out of the country. -

Young Psychiatrists' Network Meeting “Stigma from the Yps' Perspective: Hopes and Challenges”, September 27-29 2012, Minsk, Belarus
International conference 3rd Young Psychiatrists’ Network Meeting “Stigma From The YPs' perspective: Hopes and Challenges” September 27-29, 2012 Programme and abstract booklet Ministry of Health of the Republic Of Belarus State Educational Establishment “Belarusian Medical Academy of Post-Graduate Education” Supported by Rotary club “Minsk” International conference 3rd Young Psychiatrists’ Network Meeting “Stigma From The YPs' perspective: Hopes and Challenges” September 27-29, 2012 Programme and abstract booklet Ltd “Magic” Minsk 2012 UDC (УДК) 61 LCN (ББК) 56.14 Scientific edition 3rd Young Psychiatrists' Network Meeting “Stigma From The YPs' perspective: Hopes and Challenges”, September 27-29 2012, Minsk, Belarus. International conference: Programme and abstract booklet. – Minsk: Publishing house “Magic“, 2012. - 84 p. ISBN 978 – 985-6473-81-7 Supported by European Federation of Psychiatrists’ Trainees (EFPT) Supported by Belarusian Medical Academy of Post-Graduate Education (BelMAPGE) Supported by Belarusian Psychiatric Association (BPA) Supported by Rotary club “Minsk” Editorial Board: J. Hanson, MD, PhD, Assoc. Prof., Sweden; D. Krupchanka, MD, PhD student, Belarusian Medical Academy of Postgraduate Education, Minsk, Belarus; N. Bezborodovs, MD, Riga Stradins University, Riga Centre of Psychiatry and Addiction Disorders, Latvia; M. Bendix, MD, Dr. Med., Karolinska University Hospital Huddinge, Sweden; S. Jauhar, MD, MBChB, BSc (Hons), MRCPsych, Department of Psychosis Studies, Institute of Psychiatry, United Kingdom; D. Smirnova, MD, PhD, Samara State Medical University, Russian Federation. ISBN 978 – 985-6473-81-7 © State Educational Establishment “Belarusian Medical Academy of Post- Graduate Education” Anyone who keeps learning stays young. The greatest thing in life is to keep your mind young. (c) There is a story of our meetings. -

Bioethical Differences Between Drug Addiction Treatment Professionals Inside and Outside the Russian Federation Mendelevich
Bioethical differences between drug addiction treatment professionals inside and outside the Russian Federation Mendelevich Mendelevich Harm Reduction Journal 2011, 8:15 http://www.harmreductionjournal.com/content/8/1/15 (10 June 2011) Mendelevich Harm Reduction Journal 2011, 8:15 http://www.harmreductionjournal.com/content/8/1/15 RESEARCH Open Access Bioethical differences between drug addiction treatment professionals inside and outside the Russian Federation Vladimir D Mendelevich Abstract This article provides an overview of a sociological study of the views of 338 drug addiction treatment professionals. A comparison is drawn between the bioethical approaches of Russian and foreign experts from 18 countries. It is concluded that the bioethical priorities of Russian and foreign experts differ significantly. Differences involve attitudes toward confidentiality, informed consent, compulsory treatment, opioid agonist therapy, mandatory testing of students for psychoactive substances, the prevention of mental patients from having children, harm reduction programs (needle and syringe exchange), euthanasia, and abortion. It is proposed that the cardinal dissimilarity between models for providing drug treatment in the Russian Federation versus the majority of the countries of the world stems from differing bioethical attitudes among drug addiction treatment experts. Introduction deontological norms [6,10]. Although there have been Russian and international narcology (addiction medi- calls for adherence to the principles of medical ethics, cine) began to develop along divergent paths during the the procedures put into practicecontinuetobeincom- second half of the twentieth century. Indeed, Russian patible with these principles. Drug addicts still have narcology has ceased to be a part of international nar- even fewer patient rights than the mentally ill. -

American Psychiatric Press Review of Should Be Highly Interactive
1998 SCIENTIFIC PROGRAM COMMITTEE Seated (left to right): Drs. Butterfield, Panzer, Winstead, Muskin, Reifler, Balon. 1st Row Standing (left to right): Drs. Pena, McDowell, Levin, Mega, Shafii, Ishiki, Spitz, Millman, Clark, Goldfinger. 2nd Row Standing (left to right): Drs. Lu, Wick, Ratner, Belfec Hendren, Tamminga, Book, Freebury. 3rd Row Standing (left to right): Drs. Skodol, Greiner, Cutler, Weissman, Schneider, Hamilton. May 30,1998 Dear Colleagues and Guests: Welcome to the 151st Annual Meeting of the American Psychiatric Association. The theme for this meeting, which reflects our determination, vision and concern for every sector of American psychiatry, is: New Challenges for Proven Values: Defending Access, Fairness, Ethics, Decency As we work hard to build a better future for our patients, including children, minorities, the elderly and their families, there are some fundamentals we must keep in mind. Indeed, much of the scientific program addresses these issues. There are sessions on confidentiality, psychiatric education, ethics, the doctor/patient relationship, private practice, economics and managed care, as well as many excellent sessions on the latest developments in research and clinical practice. Two special "Days of Creation" have been planned for Monday and Tuesday, during which several sessions will highlight creativity. On Wednesday, selected sessions will examine "A Time of Violence." I am delighted that our international registration has grown so considerably over the past several years. That so many colleagues from around the world attend our Annual Meeting is a tribute to its high quality and diversity. At this meeting we will have a number of outstanding international guests, including leaders from the World Psychiatric Association, some of whom will make presentations and many of whom will represent their organizations at the Opening Session. -
Mental Health and Work: Impact, Issues and Good Practices Mental Health and Work
NATIONS NATIONS FOR MENTAL HEALTH FOR MENTAL NATIONS FOR MENTAL HEALTH Mental health and work: Impact, issues and good practices Mental health and work Mental Health Policy and Service Development Department of Mental Health and Substance Dependence Noncommunicable Diseases and Mental Health World Health Organization Target Group Unit InFocus Program on Knowledge, Skills and Employability WHO/ILO International Labour Organisation Geneva 2000 Mental health policy and service development team Publications produced or distributed by Nations for Mental Health Objectives and strategies • To strengthen mental health policies, legislation and plans through: increasing awareness of the burden associated with mental health problems and the commitment Publications of governments to reduce this burden; helping to build up the technical capacity of countries to create, review and develop mental health policies, legislation and plans; Gender differences in the epidemiology of affective disorders and schizophrenia. and developing and disseminating advocacy and policy resources. WHO/MSA/NAM/97.1. (Out of print) • To improve the planning and development of services for mental health through: Nations for Mental Health: An overview of a strategy to improve the mental health of strengthening the technical capacity of countries to plan and develop services; underserved populations. supporting demonstration projects for mental health best practices; encouraging WHO/MSA/NAM/97.3. Rev.1 operational research related to service delivery; and developing and disseminating resources related to service development and delivery. Nations for Mental Health: A focus on women.* WHO/MSA/NAM/97.4. ° Financial support is provided from the Eli Lilly and Company Foundation, the Johnson and Order n 1930123. Sw.Fr.