Maintenance Culture + Human Factors Training
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Westland Wessex
This article is taken from Wikipedia Westland Wessex This article is about the helicopter. For the fixed-wing for rapid starting and thus faster response times.[1] The aircraft, see Westland IV. Wessex could also operate in a wide range of weather conditions as well as at night, partly due to its use of an automatic pilot system. These same qualities that made The Westland Wessex is a British-built turbine-powered the Wessex well-suited to the anti-submarine role also development of the Sikorsky H-34, it was developed lent themselves to the search and rescue (SAR) mission, and produced under license by Westland Aircraft (later which the type would become heavily used for.[1] Westland Helicopters). One of the main changes from Sikorsky’s H-34 was the replacement of the piston-engine powerplant with a turboshaft engine; the Wessex was the first helicopter in the world to be produced in large num- bers that made use of a gas turbine propulsion system.[1] Early models were powered by a single Napier Gazelle engine, later builds used a pair of Rolls-Royce Gnome engines. The Wessex was initially produced for the Royal Navy (RN) and later for the Royal Air Force (RAF); a limited number of civilian aircraft were also produced, as well as some export sales. The Wessex operated as an anti- submarine warfare and utility helicopter; it is perhaps best recognised for its use as a search and rescue (SAR) he- licopter. The type entered operational service in 1961, A pair of Royal Navy Wessex helicopters in the flight deck of the and had a service life in excess of 40 years before being HMS Intrepid, 1968 retired in Britain. -

FROM CRADLE to GRAVE? the Place of the Aircraft
FROM CRADLE TO GRAVE? The Place of the Aircraft Carrier in Australia's post-war Defence Force Subthesis submitted for the degree of MASTER OF DEFENCE STUDIES at the University College The University of New South Wales Australian Defence Force Academy 1996 by ALLAN DU TOIT ACADEMY LIBRARy UNSW AT ADFA 437104 HMAS Melbourne, 1973. Trackers are parked to port and Skyhawks to starboard Declaration by Candidate I hereby declare that this submission is my own work and that, to the best of my knowledge and belief, it contains no material previously published or written by another person nor material which to a substantial extent has been accepted for the award of any other degree or diploma of a university or other institute of higher learning, except where due acknowledgment is made in the text of the thesis. Allan du Toit Canberra, October 1996 Ill Abstract This subthesis sets out to study the place of the aircraft carrier in Australia's post-war defence force. Few changes in naval warfare have been as all embracing as the role played by the aircraft carrier, which is, without doubt, the most impressive, and at the same time the most controversial, manifestation of sea power. From 1948 until 1983 the aircraft carrier formed a significant component of the Australian Defence Force and the place of an aircraft carrier in defence strategy and the force structure seemed relatively secure. Although cost, especially in comparison to, and in competition with, other major defence projects, was probably the major issue in the demise of the aircraft carrier and an organic fixed-wing naval air capability in the Australian Defence Force, cost alone can obscure the ftindamental reordering of Australia's defence posture and strategic thinking, which significantly contributed to the decision not to replace HMAS Melbourne. -

We Envy No Man on Earth Because We Fly. the Australian Fleet Air
We Envy No Man On Earth Because We Fly. The Australian Fleet Air Arm: A Comparative Operational Study. This thesis is presented for the Degree of Doctor of Philosophy Murdoch University 2016 Sharron Lee Spargo BA (Hons) Murdoch University I declare that this thesis is my own account of my research and contains as its main content work which has not previously been submitted for a degree at any tertiary education institution. …………………………………………………………………………….. Abstract This thesis examines a small component of the Australian Navy, the Fleet Air Arm. Naval aviators have been contributing to Australian military history since 1914 but they remain relatively unheard of in the wider community and in some instances, in Australian military circles. Aviation within the maritime environment was, and remains, a versatile weapon in any modern navy but the struggle to initiate an aviation branch within the Royal Australian Navy was a protracted one. Finally coming into existence in 1947, the Australian Fleet Air Arm operated from the largest of all naval vessels in the post battle ship era; aircraft carriers. HMAS Albatross, Sydney, Vengeance and Melbourne carried, operated and fully maintained various fixed-wing aircraft and the naval personnel needed for operational deployments until 1982. These deployments included contributions to national and multinational combat, peacekeeping and humanitarian operations. With the Australian government’s decision not to replace the last of the aging aircraft carriers, HMAS Melbourne, in 1982, the survival of the Australian Fleet Air Arm, and its highly trained personnel, was in grave doubt. This was a major turning point for Australian Naval Aviation; these versatile flyers and the maintenance and technical crews who supported them retrained on rotary aircraft, or helicopters, and adapted to flight operations utilising small compact ships. -

A-4G Skyhawk
A-4G Skyhawk Fleet Defender NATOPS 4 x AIM 9B FRONT Sidewindewinder PHOTOS s San Diego, 1967 California USA in Dull Light Dove Grey 1 4 x AIM 9B Top/White under & top of 2 ailerons & elevators only 3&4 Sidewinders Delivery Paint Scheme under wing http://www.alternatewars.com/SAC http://www.alternate wars.com/SAC/ AIM-9B_Sidewinder_1 A_SMC_- _January_1972.pdf SAC.htm / Skyhawk Aerial Refuelling http://www.awm.gov.au/collection/F11246/ Screen Grab from a 1968 movie about new A4Gs not long after arrival at NAS http://postimg.org/ image/89v3danxv/ Waiting for official handover with four underwing AIM-9B Sidewinders USofA 26 July 1967 RAN FAA Squadron Prefix Changes c.1970 then 1997 805 Squadron History http://www.navy.gov.au/history/squadron-histories/805-squadron-history “...By now [1970] the RAN had adopted USN prefixes for its Fleet Air Arm squadrons and 805 Squadron became VF805 Squadron, V standing for fixed-wing and F for fighter....” - In 1997 the RAN dropped the USN prefixes that had been attached to FAA Squadrons for the past 28 years i.e. VF-805 (V=Fixed Wing; F=Fighter) and VC-724 (C=Composite [several aircraft types]). H=Helicopter; S=Anti-Submarine; T=Training [I reckon the change was 1969-1970 also]. - 723 Squadron History http://www.navy.gov.au/history/squadron-histories/723-squadron-history “...In 1997 the RAN dropped the prefixes that had been attached to FAA Squadrons for the past 25 [28] years & HC723 Squadron reverted back to 723 Squadron....” Captain Cook Graving Dock open NAVY NEWS 09 October 1981 Cover Photo with HMAS Otway surfacing during http://www.navy.gov.au/sites/default/files/documents/Navy_News-October-9-1981.pdf NAVY WEEK display, 1981 “Eight British Oberon class submarines were ordered in 1964, to be built in Scotland in two batches of four boats. -

The Navy Vol 34 Part 2 1972 (Aug-Sep Oct, Nov-Dec 1972-Dec 1973)
AUGUST SEPTEMBER - OCTOBER, 1972 • or posting At a periodica' — Category A Cents THE NAVY. The magazine of tha Navy League of Australia Registered tor posting as a periodical — Category A Vol. 34 AUGUST-SEPTEMBER-OCTOBER, 1972 No. 3 A Special Edition for Navy Week in Australia — Featuring the Royal Australian Navy CONTENTS Page Page The Australian Fleet in the 1980's 3 Message from the Federal President of Message from the Minister for the Navy 5 The Navy League of Australia 27 Message from the Chief of Naval Staff 7 Ecumenical Church Service — Approval of DDL Project 9 Sunday, 8 October — Open to the public . 43 H.M.A.S. Watson — History and Activities 13 H.M.A.S. Penguin — Public Open Day — Programme 17 Public Open Day — Programme 45 Purchase of Sea King Helicopters 19 H.M.A.S. Ntrimba — H.M.A.S. Platypus — History and Activities 23 History and Activities 47 Public Opan Day — Programme 25 Public Open Day — Programme 47 New Survey Ship 35 New Oceanographic Ship — Cook SI Navy Weak in Australia — Sea Cadet Corps News — All States 55 Programmes of Events for all States 29 Navy League of Queensland — Annual Report. 64 Pi US SUNDRY STORIES AND PHOTOGRAPHS The views expressed in artcles appearing m this publication are those ol the authors concerned They do not necessarily represent the views of the editor, the Navy League, or oMicial opinions or policy Published by the Navy League of Australia. Box 1719, G.P.O., Sydney, N.S.W., 2001; Phone: 2411008 All correspondence should be directed to the EdRor. -
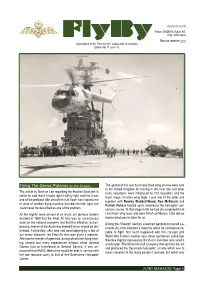
Flyby Jun18 V2
ABN 3007 129 1677 Patron: RADM N. Ralph AO, DSC, RAN Ret’d FlyBy See our website here A periodical of the Fleet Air Arm Association of Australia Edition No 11 June 18. Flying The Genus Platanus by Ken Douglas The upshot of this was that many fixed wing aircrew were sent to the United Kingdom for training in this new role and other The article by Norman Lee regarding the Hawker Seahawk in lucky volunteers were introduced to 723 Squadron and the which he said that if it looks right it will fly right and that it was black magic of rotary wing flight. I was one of the latter and one of the prettiest little aircraft he had flown has inspired me together with Rowley Waddell-Wood, Ron McKenzie and to write of another flying machine that did not look right and Patrick Vickers fronted up to commence the helicopter con- could never be described as one of the prettiest. version course. At that stage in life we had all completed Front As the slightly more ancient of us recall, our glorious leaders Line fixed- wing tours and were full of confidence. Little did we decided in 1959 that the Fleet Air Arm was an unnecessary realise what was in store for us. drain on the national economy and that this effective, but ex- During the Fifteenth Century a learned gentleman named Le- pensive, branch of the Australian Armed Forces should be dis- onardo Da Vinci invented a machine which he considered ca- banded. Fortunately, after long and hard lobbying by a few of pable of flight. -

The Royal Australian Navy (RAN) Fleet Air Arm (FAA) and Objective
CASE STUDY | ROYAL AUSTRALIAN NAVY - FLEET AIR ARM Objective ECM has become so integral to the FAA’s operations that senior officersno longer accept paper to sign unless it is an exception. Joseph Stablum FAA Information Management Project, Navy Fleet Air Arm ORGANISATION The Royal Australian Navy (RAN) Fleet Air Arm (FAA) Royal Australian Navy (RAN) Fleet Air Arm (FAA) and Objective ECM improve operational visibility INDUSTRY and accountability. Defence Even the most rigorous, procedure-based organisation like the Royal Australian Navy USERS (FAN) Fleet Air Arm (FAA) sometimes faces a challenge that forces it to transform itself. 1,100 For the FAA, that challenge came in the form of finding a robust information management solution that would deliver full auditability and traceability, enabling confident decision SOLUTION making and adherence to safety and airworthiness regulatory compliance. This system needed to shape and prepare the organisation for a major change in the safety and airworthiness regulations. The level of improvement required was well beyond the former system capabilities. The FAA’s objective was to have an Australia best information management system that met operational outcomes and enabled regulatory compliance confidence. BENEFITS AT A GLANCE Better visibility to ensure compliance The requirement for assured compliance confidence, and the awareness of a full new suite of safety with mandatory safety and airworthiness and airworthiness regulations around the corner highlighted the need for change to the newly regulations appointed Commander of the Fleet Air Arm, Commodore Chris Smallhorn, who realised after his assuming Command that ponderous processes were perpetuating inefficiencies for the greater than Greater confidence in making informed 1100 FAA staff under his command. -

The Vietnam War and the Royal Australian Navy
The Vietnam War and the Royal Australian Navy The following address was delivered by Captain Ralph T. Derbidge MBE RAN (Retired) at the Melbourne Shrine of Remembrance to mark Vietnam Veterans Day on 18 August 2010. It describes the commitment of RAN fleet and air units to that War and the variety of essential tasks and services they provided in support of both the ground and air war. Captain Derbidge concluded his 36 years of service in 1990 as the Director of Facilities Planning-Navy. A specialist Gunnery Officer he served in that capacity in five RAN and RN ships. He had intervening tours as a Staff Officer to the Australian Naval Attache in Washington, as Deputy Director of Surface and Air Weapons and with the Joint Intelligence Organisation. He commanded HMA Ships Stuart, Canberra and Success and the RAN Apprentice Training Establishment, HMAS Nirimba. Vietnam - tropical, alluring, fun-filled, breathtakingly beautiful, gastronomically exciting and friendly – today, a magnetic attraction for numerous tourists, businessmen and capital investors, many of them Australians, including Vietnam War veterans. Ask my wife about Vietnam. She welcomed me home from the war 39 years ago, but in recent times she enjoyed greatly with friends a group bicycle tour from Ho Chi Minh City to Hanoi. I didn’t go – I get sunburnt! But it was not always like that. 1 Vietnam, some 7,500 kilometres to our north west as the crow flies from Melbourne, and three hours behind Australia’s Eastern Standard Time, lies between the Tropic of Cancer and the Equator. It is bordered to the west by Cambodia and Laos, and to the north by China. -

RAN FLEET AIR ARM AIRCRAFT by T.W
Aviation Historical Society of Australia Journal -4- March-April 1974 RAN FLEET AIR ARM AIRCRAFT by T.W. Boughton and N.M. Parnell The relatively small number of aircraft operated by the Royal Australian Navy can be readily classified by colour sch'eme/marking systems as well as by type. These classifications can be sub-divided so that existing records may be interpreted \ to determine the period of operation. As mentioned previously, there is a paucity of information on RAN aircraft and the y4/ following notes are intended to provide a general picture of the subject. lt should be noted that there have been considerable variations in detail markings on individual machines from the stindard schemes described, but these variations are not con- sidered in the following notes. AI RCRAFT COLOUR SCHEMES Training in England The first pilots in RAN Aviationl *.r, experienced airmen who had served with the RN FAA, RAF, RAAF and RNZAF. This group of pilots formed the 20 CAG. Subsequent RAN pilots including trainees who entered and were trained as naval pilots were trained in England with RN units up to 1959. These pilots were given refresher training in England on Fairey Fireflies and Hawker Sea Furies. The machines were from the Royal Navy, on loan, and were painted in the then-current colour schemes - gloss dark grey/dark olive green upper surfaces and sky on the lower surfaces, while a small number were in the better known dark sea grey and sky. These machines used the lOOl2OO series code numbers (single and two seat respectively) and the base letters JR fBruAs Eglington), As they moved on board the newly commissioned - HMAS Sydnq, the base letter was changed to K. -

Order of Battle 2.Indd
205.200.206.202 Order of Battle Credits Contents Introduction 2 Lead Developer Erik Nicely New Rules 3 Motor Torpedo Boats 8 Developers Richard L. Bax, Agis Neugebauer, Erik Nicely Admirals 11 Wulf Corbett, David Manley Advanced Aircraft Operations 15 Editor Scenarios 22 Nick Robinson Hunting the Beast 27 Contents Cover Expanded Fleet List 34 Chris Quilliams Royal Navy 35 Kriegsmarine 58 Interior Illustrations Sherard Jackson, Danilo Moretti, Mike Mumah United States Navy 64 Japan 74 Miniatures Gaming Manager Ian Barstow Italian 88 French 95 Print Manager Ed Russell Soviet Union 100 Civilian Ships 110 Special Thanks Counters 112 Adam Gulwell, Peter Swarbrick of www.shipspictures.co.uk and David Page of www.navyphotos.co.uk Order of Battle (C) 2007 Mongoose Publishing. All rights reserved. Reproduction of this work by any means without the written permission of the publisher is expressly forbidden. All signifi cant art and text herein are copyrighted by Mongoose Publishing. No portion of this work may be reproduced in any form without written permission. This material is copyrighted under the copyright laws of the UK. Printed in the UK. 1 205.200.206.202 Introduction Victory at Sea had a humble beginning as a bare-bones set of free rules in Mongoose Publishing’s Signs and Portents online magazine. That initial free rules set proved to be popular and led to the development of the core rulebook, which was an immediate success. A loyal international fan base developed as Victory at Sea quickly earned itself a place as one of the ‘standards’ of World War II naval wargaming. -

Kiwi 'Drivers' and 'Lookers' : an Analysis and Examination of the Significant
Copyright is owned by the Author of the thesis. Permission is given for a copy to be downloaded by an individual for the purpose of research and private study only. The thesis may not be reproduced elsewhere without the permission of the Author. Kiwi ‘Drivers’ and ‘Lookers’ An Analysis and Examination of the Significant Contribution of New Zealand Fleet Air Arm Aircrew, of the British Pacific Fleet, to Allied Naval Operations 1944-1945 A thesis presented in partial fulfillment of the requirements for the degree of Master of Arts in History at Massey University, Albany, New Zealand. Patrick Jeremy Lyon Thomson 2012 Abstract This thesis addresses a neglected and under-researched area of New Zealand historiography in World War II: the contribution of New Zealand Fleet Air Arm aircrew serving with the British Pacific Fleet (BPF), from December 1944 to the end of hostilities with Japan in August 1945. The operational experiences, services and sacrifices of these airmen are examined within the wider context of New Zealand’s diplomacy and strategy for the Pacific war. Three research questions are posited. First, what were New Zealand’s different responses to Japanese military aggression in the Pacific, from 1941 to 1944, particularly in association with its allies? Second, what was the genesis of the British Pacific Fleet, and what were its structures and strategic functions? Third, in what ways did New Zealand aircrew contribute to the British Pacific Fleet’s Air Arm operations from 1944 to 1945? In memory of my dearly loved eldest son, James David Lyon Thomson - 15 July 1983 to 12 July 2011. -
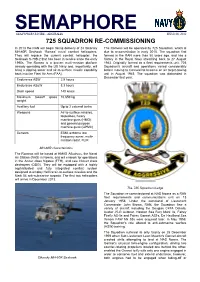
Semaphore 8.Pdf
SEMAPHORE SEA POWER CENTRE - AUSTRALIA ISSUE 08, 2012 725 SQUADRON RE-COMMISSIONING In 2013 the RAN will begin taking delivery of 24 Sikorsky The Romeos will be operated by 725 Squadron, which is MH-60R Seahawk ‘Romeo’ naval combat helicopters. due to re-commission in early 2015. The squadron first They will replace the current combat helicopter, the formed in the RAN more than 50 years ago, and has a Seahawk S-70B-2 that has been in service since the early history in the Royal Navy stretching back to 27 August 1990s. The Romeo is a proven multi-mission platform 1943. Originally formed as a fleet requirements unit, 725 already operating with the US Navy and, importantly, will Squadron's aircraft and operations varied considerably bring a dipping sonar and air-to-surface missile capability before moving to Cornwall to become an air target-towing back into the Fleet Air Arm (FAA). unit in August 1945. The squadron was disbanded in December that year. Endurance ASW 2.9 hours Endurance ASuW 3.3 hours Dash speed 140 knots Maximum takeoff gross 10,659 kg weight Auxiliary fuel Up to 2 external tanks Weapons Air-to-surface missiles, torpedoes, heavy machine guns (HMG) and general purpose machine guns (GPMC) Sensors ESM, airborne low frequency sonar, multi- mission radar, FLIR MH-60R characteristics The Romeos will be based at HMAS Albatross, the Naval Air Station (NAS) in Nowra, and will embark for operations in the Anzac class frigates (FFH), and new Hobart class destroyers (DDG). They will be equipped with a highly sophisticated and fully integrated combat system designed to employ Hellfire air-to-surface missiles and the Mark 54 anti-submarine torpedo.