The Returns to Nursing: Evidence from a Parental Leave Program
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Teritoriální Uspořádání Policejních Složek V Zemích Evropské Unie: Inspirace Nejen Pro Českou Republiku II – Belgie, Dánsko, Finsko, Francie, Irsko, Itálie1 Mgr
Teritoriální uspořádání policejních složek v zemích Evropské unie: Inspirace nejen pro Českou republiku II – Belgie, Dánsko, Finsko, Francie, Irsko, Itálie1 Mgr. Oldřich Krulík, Ph.D. Abstrakt Po teoretickém „úvodním díle“ se ke čtenářům dostává pokračování volného seriálu o teritoriálním uspořádání policejních sborů ve členských státech Evropské unie. Kryjí nebo nekryjí se „policejní“ (případně i „hasičské“, justiční či dokonce „zpravodajské“) regiony s regiony, vytýčenými v rámci státní správy a samosprávy? Je soulad těchto územních prvků možné považovat za výjimku nebo za pravidlo? Jsou členské státy Unie zmítány neustálými reformami horizontálního uspořádání policejních složek, nebo si tyto systémy udržují dlouhodobou stabilitu? Text se nejprve věnuje „starým členským zemím“ Unie, a to pěkně podle abecedy. Řeč tedy bude o Belgii, Dánsku, Finsku, Francii, Irsku a Itálii. Klíčová slova Policejní síly, územní správa, územní reforma, administrativní mezičlánky Summary After the theoretical “introduction” can the readers to continue with the series describing the territorial organisation of the police force in the Member States of the European Union. Does the “police” regions coincide or not-coincide with the regions outlined in the state administration and local governments? Can the compliance of these local elements to be considered as an exception or the rule? Are the European Union Member States tossed about by constant reforms of the horizontal arrangement of police, or these systems maintain long-term stability? The text deals firstly -

Areal Og Befolkning
1 Areal og befolkning Tabel 1. Danmarks kystlinie, areal og befolkningstæthed. Coast line, area, and density of population. Kystlinie 1906' ArealI. april 1961 Befolknings- Folketal tæthed 26. sept. 1960 pr. km' Geografiske km' Geografiske km mil kv.mil 26. sept. 1960 1 3 4 5 0 A. Sjælland i alt ........................... 1 898,5 255,85 7 542,88 136,9 1 973 108 261,6 Københavns kommune ................... 67,8 9,14 83,38 1,5 721 381 8 651,7 Frederiksberg kommune .................. 8,70 0,2 114 285 13 136,2 Københavns amtsrådskreds ............... 183,1 24,68 493,46 9,0 486 139 985,2 Roskilde amtsrådskreds ................... 142,4 19,20 690,54 12,5 90 337 130,8 Frederiksborg amt ....................... 279,3 37,63 1 343,71 24,4 181 663 135,2 Holbæk amt ............................ 528,9 71,27 1 751,84 31,8 127 747 72,9 Sorø amts .............................. 211,9 28,55 1 478,60 26,8 129 580 87,6 Præstø amt ............................. 485,1 65,38 1692,65 30,7 121 976 72,1 B. Bornholm ............................... 158,3 21,34 587,55 10,7 48 373 82,3 C. Lolland-Falster .......................... 620,2 83,57 1 797,70 32,6 131 699 73,3 D. Fyn i alt ............................... 1 137,2 153,26 3482,10 63,3 413 908 118,9 Svendborg amt .......................... 633,6 85,39 1 666,51 30,3 149 163 89,5 Odense amtsrådskreds .................... 292,0 39,35 1 148,91 20,9 207273 180,4 Assens amtsrådskreds ..................... 211,6 28,52 666,68 12,1 57472 86,2 A-D. -

Bøgsted, Bent (DF)
Bøgsted, Bent (DF) Member of the Folketing, The Danish People's Party Semiskilled worker Bakkevænget 2 9750 Østervrå Parliamentary phone: +45 3337 5101 Mobile phone: +45 6162 3360 Email: [email protected] Bent Gunnar Bøgsted, born January 4th 1956 in Brønderslev, Serritslev Parish, son of former farmer Mandrup Verner Bøgsted and Kirsten Margrete Bøgsted. Married to Hanne Bøgsted. The couple has seven children. Member period Member of the Folketing for The Danish People's Party in North Jutland greater constituency from November 13th 2007. Member of the Folketing for The Danish People's Party in North Jutland County constituency, 20. November 2001 – 13. November 2007. Candidate for The Danish People's Party in Frederikshavn nomination district from 2010. Candidate for The Danish People's Party in Brønderslev nomination district, 20072010. Candidate for The Danish People's Party in Fjerritslev nomination district, 20042007. Candidate for The Danish People's Party in Aalborg East nomination district, 20042007. Candidate for The Danish People's Party in Hobro nomination district, 20012004. Parliamentary career Chairman of the Employment Committee, 20152019. Clerk of Parliament from 2007. Spokesman on labour market from 2001. Spokesman on the Home Guard and social dumping. Education Aaalborg Technical School, 19721976. Skolegade School, Brønderslev, 19701972. Serritslev School, Brønderslev, 19631970. Employment Semiskilled worker at Repsol, Brønderslev, 19932001. Shipyard worker, Ørskov Stålskibsværft, 19901993. Farmer, 19861989. Armourer with the North Jutland Artillery Regiment, Skive, 19771986. Avedøre Recruit and NCO School, 19761977. Engineering worker at Uggerby Maskinfabrik, Brønderslev, 19721976. -

Sikre Skoleveje En Undersøgelse Af Børns Trafiksikkerhed Og Transportvaner
Sikre skoleveje En undersøgelse af børns trafiksikkerhed og transportvaner Rapport 3 Søren Underlien Jensen og Camilla Hviid Hummer Sikre skoleveje En undersøgelse af børns trafiksikkerhed og transportvaner Rapport 3 Søren Underlien Jensen og Camilla Hviid Hummer Sikre skoleveje En undersøgelse af børns trafiksikkerhed og transportvaner Rapport 3 2002 Af Søren Underlien Jensen og Camilla Hviid Hummer Fotos: Lars Bahl Søren Underlien Jensen Tryk: Herrmann & Fischer Oplag: 700 Copyright: Eftertryk tilladt med kildeangivelse Udgivet af: Danmarks TransportForskning Knuth-Winterfeldts Allé Bygning 116 Vest 2800 Kgs. Lyngby Email [email protected] www.dtf.dk Rekvireres hos IT- og Telestyrelsen Danmark.dk's netboghandel Tlf.:33 37 92 28 www.netboghandel.dk Pris: kr. 50,00 incl. moms ISSN: 1600-9592 (trykt udgave) ISBN: 87-7327-065-2 (trykt udgave) ISSN: 1601-9458 (elektronisk udgave) ISBN: 87-7327-066-0 (elektronisk udgave) Forord Danmarks TransportForskning (DTF) fik ved en bevilling på kr. 300.000 fra Trafikpulje 2000 til opgave at sætte fokus på sikre skoleveje. Mere konkret bestod opgaven i at indsamle viden om skolebørns transport og udarbejde en samlet oversigt over skolebørns transportvaner i Danmark. DTF definerede projektet til at omhandle fire delstudier: • Et studie om børns trafikulykker i Danmark, • en beskrivelse og konsekvensvurdering af danske kommuners indsats for at forbedre skolebørns trafiksikkerhed og ændre deres transportvaner i årene 1995-2000, • et studie af børns transportvaner i Danmark, og • et litteraturstudie om skolebørn og trafik. Studiet om danske kommuners indsats har omfattet en forespørgsel rettet til samtlige 275 kommuner. DTF vil gerne rette en stor tak til de 201 kommuner, der har svaret på denne forespørgsel, og derved muliggjort en beskrivelse og konsekvensvurdering af kommunernes indsats. -

A Meta Analysis of County, Gender, and Year Specific Effects of Active Labour Market Programmes
A Meta Analysis of County, Gender, and Year Speci…c E¤ects of Active Labour Market Programmes Agne Lauzadyte Department of Economics, University of Aarhus E-Mail: [email protected] and Michael Rosholm Department of Economics, Aarhus School of Business E-Mail: [email protected] 1 1. Introduction Unemployment was high in Denmark during the 1980s and 90s, reaching a record level of 12.3% in 1994. Consequently, there was a perceived need for new actions and policies in the combat of unemployment, and a law Active Labour Market Policies (ALMPs) was enacted in 1994. The instated policy marked a dramatic regime change in the intensity of active labour market policies. After the reform, unemployment has decreased signi…cantly –in 1998 the unemploy- ment rate was 6.6% and in 2002 it was 5.2%. TABLE 1. UNEMPLOYMENT IN DANISH COUNTIES (EXCL. BORNHOLM) IN 1990 - 2004, % 1990 1992 1994 1996 1998 2000 2002 2004 Country 9,7 11,3 12,3 8,9 6,6 5,4 5,2 6,4 Copenhagen and Frederiksberg 12,3 14,9 16 12,8 8,8 5,7 5,8 6,9 Copenhagen county 6,9 9,2 10,6 7,9 5,6 4,2 4,1 5,3 Frederiksborg county 6,6 8,4 9,7 6,9 4,8 3,7 3,7 4,5 Roskilde county 7 8,8 9,7 7,2 4,9 3,8 3,8 4,6 Western Zelland county 10,9 12 13 9,3 6,8 5,6 5,2 6,7 Storstrøms county 11,5 12,8 14,3 10,6 8,3 6,6 6,2 6,6 Funen county 11,1 12,7 14,1 8,9 6,7 6,5 6 7,3 Southern Jutland county 9,6 10,6 10,8 7,2 5,4 5,2 5,3 6,4 Ribe county 9 9,9 9,9 7 5,2 4,6 4,5 5,2 Vejle county 9,2 10,7 11,3 7,6 6 4,8 4,9 6,1 Ringkøbing county 7,7 8,4 8,8 6,4 4,8 4,1 4,1 5,3 Århus county 10,5 12 12,8 9,3 7,2 6,2 6 7,1 Viborg county 8,6 9,5 9,6 7,2 5,1 4,6 4,3 4,9 Northern Jutland county 12,9 14,5 15,1 10,7 8,1 7,2 6,8 8,7 Source: www.statistikbanken.dk However, the unemployment rates and their evolution over time di¤er be- tween Danish counties, see Table 1. -

Canada, 1872-1901
INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bieedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. ProQuest Information and Learning 300 North Zeeb Road, Ann Arbor, Ml 48106-1346 USA 800-521-0600 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. NEW DENMARK, NEW BRUNSWICK: NEW APPROACHES IN THE STUDY OF DANISH MIGRATION TO CANADA, 1872-1901 by Erik John Nielsen Lang, B.A. Hons., B.Ed., AIT A thesis submitted to the Faculty of Graduate Studies in partial fulfilment of the requirements for the degree of Master of Arts Department of Histoiy Carleton University Ottawa, Ontario 25 April 2005 © 2005, Erik John Nielsen Lang Reproduced with permission of the copyright owner. -

The Danish Design Industry Annual Mapping 2005
The Danish Design Industry Annual Mapping 2005 Copenhagen Business School May 2005 Please refer to this report as: ʺA Mapping of the Danish Design Industryʺ published by IMAGINE.. Creative Industries Research at Copenhagen Business School. CBS, May 2005 A Mapping of the Danish Design Industry Copenhagen Business School · May 2005 Preface The present report is part of a series of mappings of Danish creative industries. It has been conducted by staff of the international research network, the Danish Research Unit for Industrial Dynamics, (www.druid.dk), as part of the activities of IMAGINE.. Creative Industries Research at the Copenhagen Business School (www.cbs.dk/imagine). In order to assess the future potential as well as problems of the industries, a series of workshops was held in November 2004 with key representatives from the creative industries covered. We wish to thank all those who gave generously of their time when preparing this report. Special thanks go to Nicolai Sebastian Richter‐Friis, Architect, Lundgaard & Tranberg; Lise Vejse Klint, Chairman of the Board, Danish Designers; Steinar Amland, Director, Danish Designers; Jan Chul Hansen, Designer, Samsøe & Samsøe; and Tom Rossau, Director and Designer, Ichinen. Numerous issues were discussed including, among others, market opportunities, new technologies, and significant current barriers to growth. Special emphasis was placed on identifying bottlenecks related to finance and capital markets, education and skill endowments, labour market dynamics, organizational arrangements and inter‐firm interactions. The first version of the report was drafted by Tina Brandt Husman and Mark Lorenzen, the Danish Research Unit for Industrial Dynamics (DRUID) and Department of Industrial Economics and Strategy, Copenhagen Business School, during the autumn of 2004 and finalized for publication by Julie Vig Albertsen, who has done sterling work as project leader for the entire mapping project. -

Regional Innovation and Industrial Policies and Strategies - a Selective Comparative European Study
REGIONAL INNOVATION AND INDUSTRIAL POLICIES AND STRATEGIES - A SELECTIVE COMPARATIVE EUROPEAN STUDY By Patricia Doherty B. A. (Mgmt.) Thesis submitted for the award of M.B.S. (Master of Business Studies) to the Dublin Business School, Dublin City University. October 1997. Supervisors: Mr. Joseph Davis, Senior Lecturer, Faculty of the Built Environment, Dublin Institute of Technology, Bolton Street. Mr. Gerry Sweeney, Managing Director, SICA Innovation Consultants. I hereby certify that this material which I now submit for assessment on the programme of study leading to the award of M.B.S. is entirely my own work and has not been taken from the work of others save and to the extent that such work has been cited and acknowledged within the text of my work. Signed : PryWuitx QoU/A-m Date : 6 ^ IQ? To the memory of Edith Acknowledgements There are a number of people without whose assistance this thesis could not have been completed. Firstly, I wish to express my thanks to my supervisors, Mr. Joe Davis and Mr. Gerry Sweeney, whose guidance, support and encouragement was vital to the completion of this study. I wish to thank Mr. Bob Kavanagh, Ms. Mary Sheridan, Ms. Christiane Brennan and all in D.I.T. Head Office for making this study possible. My thanks also, to the library and administrative staff of D.I.T. Bolton Street for all their help over the last two years. Sincerest thanks are due to all those in Denmark and the Mid-West region who gave their time for interview and special thanks is due to Mr. -
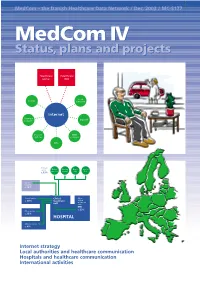
Medcom IV Status, Plans and Projects
MedCom – the Danish Healthcare Data Network / Dec. 2003 / MC-S177 MedComMedCom IV IV Status,Status, plans plans andand projectsprojects Healthcare Healthcare portal DIX Local County authority Internet Pharmacy Dan Net network Doctors’ KMD systems network KPLL Primary sector Medical Nursing Home Specia- practice homes care lists c. 13% Other hospitals c. 10% Clinical service Clinical Other c. 40% treatment clinical treatment unit units EPR c. 23% Other service c. 13% HOSPITAL Administration c. 4% ● Internet strategy ● Local authorities and healthcare communication ● Hospitals and healthcare communication ● International activities 2 MedCom IV – status, plans and projects Contents Aims of MedCom 2 The local authorities and healthcare communication 20 Introduction 3 The Hospital-Local Authority XML project 20 Healthcare on the move 3 The Hospital-Local Authority project and Common Language 22 History 4 Commentary: The Minister of Social Affairs, Henriette Kjær 22 The MedCom steering group 6 The LÆ form project 23 Commentary: The Minister of the Interior and Commentary: The Chairman of the National Health, Lars Løkke Rasmussen 7 Association of Local Authorities, Perspective: MedCom certifies communication 8 Ejgil W. Rasmussen 24 Perspective: The IT Lighthouse’s local authority- The Internet strategy 9 medical practice communication 24 The infrastructure project 9 The hospitals and Commentary: The Chairman of the Association of healthcare communication 25 County Councils, Kristian Ebbensgaard 12 Perspective: The Internet strategy and the From -

KV Süddänemark-Dänisch Ohne Bild
Ministerium für Justiz, Arbeit und Europa des Landes Schleswig-Holstein Grænseoverskridende samarbejde med Region Syddanmark Rapport fra delstatsregeringen i Schleswig-Holstein om det grænseoverskridende samarbejde med Region Syddanmark ”At vokse sammen“ er det fælles anliggende for den slesvig-holstenske delstatsregering og Region Syddanmark. Begge sider er overbeviste om, at det grænseoverskridende samarbejde leverer betydelige impulser til den økonomiske, sociale og kulturelle udvikling i hele grænseregionen. Rapporten om det grænseoverskridende samarbejde med Region Syddanmark, som den slesvig-holstenske delstatsre-gering forelægger, viser tydeligt, med hvilke store skridt samarbejdet på tværs af landegrænser i de seneste år er gået fremad. De i rapporten beskrevne aktiviteter viser, at det stærke netværk i det dansk-tyske samarbejde, som dækker over mange emner, herved har en central rolle. Endvidere kan der også ses tydeligt, at dette partnerskab i høj grad fyldes med liv gennem et stort antal af lokale grænseoverskridende projekter. Det tysk-danske partnerskab er således et af de bedste eksempler på, hvordan samarbejdet på tværs af landegrænser får Europas medlemsstater til at vokse tættere sammen. Lad os i fællesskab fortsat arbejdere videre på dette. 2 Indholdsfortegnelse Forord............................................................................................................................ .....5 1. Indledning................................................................................................................. -

The Parliamentary Electoral System in Denmark
The Parliamentary Electoral System in Denmark GUIDE TO THE DANISH ELECTORAL SYSTEM 00 Contents 1 Contents Preface ....................................................................................................................................................................................................3 1. The Parliamentary Electoral System in Denmark ..................................................................................................4 1.1. Electoral Districts and Local Distribution of Seats ......................................................................................................4 1.2. The Electoral System Step by Step ..................................................................................................................................6 1.2.1. Step One: Allocating Constituency Seats ......................................................................................................................6 1.2.2. Step Two: Determining of Passing the Threshold .......................................................................................................7 1.2.3. Step Three: Allocating Compensatory Seats to Parties ...........................................................................................7 1.2.4. Step Four: Allocating Compensatory Seats to Provinces .........................................................................................8 1.2.5. Step Five: Allocating Compensatory Seats to Constituencies ...............................................................................8 -

Screening for Chlamydia Trachomatis in Denmark
Screening for Chlamydia trachomatis in Denmark Attitudes among professionals and youth towards a strategy for sexual and reproductive health The potential of ‘The Aarhus Model’ for healthy public policy Master of Public Health Thesis Mette Kjer Kaltoft Date: 23rd of December 2003 Supervisor: Michael Væth, professor of biostatistics, Ph.d., Aarhus University Master of Public Health, Aarhus University, Denmark 2003 I Table of Contents Acknowledgements III English summary IV Danish summary VII Background 1 Aim of study 10 Part I. Danish public policy towards sexual & reproductive health 11 Material and Method 11 Result and discussion 11 Part II. Doctors 2001 study 16 Material and Method 16 Results 19 Discussion 21 Part III. Youth99 study 26 Material and Method 26 Results 29 Discussion 41 General discussion and conclusions 48 Reference list 59 List over tables 67 Appendices 68 II Acknowledgements I wish to express my gratitude and thanks to the following persons that enabled finishing my MPH thesis, each by a different route: project leader Bjarne Rasmussen who was responsible for ‘Youth 99 - a sexual profile’ study for granting access to the data; project leader and members of the national HTA Chlamydia research group, Lars Østergaard, Berit Andersen, Jens Kleist Møller, and Frede Olesen for letting me join their team and providing a superb and supportive work environment and last not least my MPH supervisor Michael Vaeth, professor of biostatistics, University of Aarhus, for human, humorous and literally numerous advice, in particular with the recoding of data and statistical analysis. Also, I want to send warm thoughts and thanks to all 7355 pupils who answered the ’youth 99’ questionnaire and the 401 physicians who despite not being reimbursed answered the questionnaire ‘doctors 2001’.