FSA Supplement March April 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Map Marking Information for Kingaroy, Queensland [All
Map marking information for Kingaroy,Queensland [All] Courtesy of David Jansen Latitude range: -30 19.8 to -23 13.5 Longitude range: 146 15.7 to 153 33.7 File created Tuesday,15June 2021 at 00:58 GMT UNOFFICIAL, USE ATYOUR OWN RISK Do not use for navigation, for flight verification only. Always consult the relevant publications for current and correct information. This service is provided free of charge with no warrantees, expressed or implied. User assumes all risk of use. WayPoint Latitude Longitude ID Distance Bearing Description 95 Cornells Rd Strip 30 19.8 S 152 27.5 E CORNERIP 421 172 Access from Bald Hills Rd 158 Hernani Strip 30 19.4 S 152 25.1 E HERNARIP 420 172 East side, Armidale Rd, South of Hernani NSW 51 Brigalows Station Strip 30 13.0 S 150 22.1 E BRIGARIP 429 199 Access from Trevallyn Rd NSW 151 Guyra Strip 30 11.9 S 151 40.4 E GUYRARIP 402 182 Paddock North of town 79 Clerkness 30 9.9 S151 6.0 ECLERKESS 405 190 Georges Creek Rd, Bundarra NSW 2359 329 Upper Horton ALA 30 6.3 S150 24.2 E UPPERALA 416 199 Upper Horton NSW 2347, Access via Horton Rd 31 Ben Lomond Strip 30 0.7 S151 40.8 E BENLORIP 382 182 414 Inn Rd, Ben Lomond NSW 2365 280 Silent Grove Strip 29 58.1 S 151 38.1 E SILENRIP 377 183 698 Maybole Rd, Ben Lomond NSW 2365 Bed and Breakfast 165 Inverell Airport 29 53.2 S 151 8.7 E YIVL 374 190 Inverell Airport, Aerodrome Access Road, Gilgai NSW 2360 35 Bingara ALA 29 48.9 S 150 32.0 E BINGAALA 381 199 Bingara Airstrip Rd West from B95 55 Brodies Plains AF 29 46.4 S 151 9.9 E YINO 361 190 Inverell North Airport, Inverell NSW 2360. -

Avis Australia Commercial Vehicle Fleet and Location Guide
AVIS AUstralia COMMErcial VEHICLES FLEET SHEET UTILITIES & 4WDS 4X2 SINGLE CAB UTE | A | MPAR 4X2 DUAL CAB UTE | L | MQMD 4X4 WAGON | E | FWND • Auto/Manual • Auto/Manual • Auto/Manual • ABS • ABS • ABS SPECIAL NOTES • Dual Airbags • Dual Airbags • Dual Airbags • Radio/CD • Radio/CD • Radio/CD The vehicles featured here should • Power Steering • Power Steering • Power Steering be used as a guide only. Dimensions, carrying capacities and accessories Tray: Tray: are nominal and vary from location 2.3m (L), 1.8m (W) 1.5m (L), 1.5m (W), 1.1m (wheelarch), tub/styleside to location. All vehicles and optional 4X4 SINGLE CAB UTE | B | MPBD 4X4 DUAL CAB UTE | D | MQND 4X4 DUAL CAB UTE CANOPY | Z | IQBN extras are subject to availability. • Auto/Manual • Auto/Manual • Auto/Manual For full details including prices, vehicle • ABS • ABS • ABS availability and options, please visit • Dual Airbags • Dual Airbags • Dual Airbags • Radio/CD • Radio/CD • Radio/CD www.avis.com.au, call 1800 141 000 • Power Steering • Power Steering • Power Steering or contact your nearest Avis location. Tray: Tray: Tray: 1.5m (L), 1.5m (W), 2.3m (L), 1.8m (W) 1.8m (L), 1.8m (W) 0.9m (H) lockable canopy VANS & BUSES DELIVERY VAN | C | IKAD 12 SEATER BUS | W | GVAD LARGE BUS | K | PVAD • Air Con • Air Con • Air Con • Cargo Barrier • Tow Bar • Tow Bar • Car Licence • Car Licence • LR Licence Specs: 5m3 2.9m (L), 1.5m (W), Specs: 12 People Specs: 1.1m (wheelarch) including Driver 20-25 People HITop VAN | H | SKAD 4.2M MovING VAN | F | FKAD 6.4M MovING VAN | S | PKAD 7.3M VAN | V | PQMR • Air Con • Air Con • Air Con • Air Con • Power Steering • Ramp/Lift • Ramp/Lift • Ramp/Lift • Car Licence • Car Licence • MR Licence • MR Licence Specs: 3.7m (L), 1.75m (W), Specs: Specs: Specs: 19m3, 4.2m (L), 34m3, 6.4m (L), 42m3, 7.3m (L), 1.9m (H), between 2.1m (W), 2.1m (H), 2.3m (W), 2.3m (H), 2.4m (W), 2.4m (H), wheel arch 1.35m (L) up to 3 pallets up to 10 pallets up to 12 pallets *Minimum specs. -

Year in Review
Queensland Section YEAR IN REVIEW 14/15 Our Mission 3 Our Vision, Our Values 4 Chairman’s Report 5 CEO’s Report 6 2014/15 Highlights 7 2014/15 Overview 10 Health Services 10 Clinical Governance Highlights 10 Integrated Operations 11 Finance 14 People and Corporate Services 14 Marketing and Fundraising 15 Bequests and Trusts In Perpetuity 16 Our Patients > Shannon Smithwick 18 Map > Locations we travelled to 19 The Furthest Corner. The Finest Care. 20 Map > Our primary health care locations 22 Our People 23 Our Patients > Tayla Law 24 Our Bases 25 Our Partners and Supporters 26 About the Royal Flying Doctor Service The Royal Flying Doctor Service of Australia (RFDS) takes the finest care to the furthest corners of our land. Established in 1928 by the Reverend John Flynn, the RFDS has grown to become the largest and most comprehensive aeromedical organisation of its kind in the world, delivering 24-hour emergency aeromedical and primary health care services to all those who live, work and travel throughout Australia. Today, the RFDS conducts more than 290,000 patient consults across Australia every year – that’s one person every two minutes. In Queensland, the RFDS currently operates from nine bases at Brisbane, Bundaberg, Cairns, Charleville, Longreach, Mount Isa, Rockhampton, Roma and Townsville. These bases form a strategic network of aeromedical services as well as delivering a broad range of health care programs including general practice, Aboriginal and Torres Strait Islander health, child and family health, social and emotional wellbeing, mental health, women’s health, oral health and health promotion activities. -

2019-20 Budget Estimates Volume of Additional Information
2019-20 Budget Estimates Volume of Additional Information Reports No. 30 and 31, 56th Parliament Economics and Governance Committee August 2019 Table of Contents Correspondence regarding leave to participate in the hearing Questions on notice and responses Speaker of the Legislative Assembly Questions on notice and responses Premier and Minister for the Trade Questions on notice and responses Deputy Premier, Treasurer and Minister for Aboriginal and Torres Strait Islander Partnerships Questions on notice and responses Minister for Local Government, Minister for Racing and Minister for Multicultural Affairs Answers to questions taken on notice at the hearing 23 July 2019 Responses to requests for additional information taken at the hearing 23 July 2019 Documents tabled at the hearing 23 July 2019 Correspondence regarding leave to participate in the hearing Correspondence 1. 25 June 2019 – Letter from Deb Frecklingon MP, Leader of the Opposition and Shadow Minister for Trade 2. 4 July 2019 – Letter from Sandy Bolton MP, Member for Noosa 3. 16 July 2019 – Letter from Jon Krause MP, Member for Scenic Rim 4. 16 July 2019 – Email from Michael Berkman MP, Member for Maiwar 25 June 2019 Economics and Governance Committee Attention: Mr Linus Power MP, Chair By email: [email protected] Dear Mr Power Reference is made to the consideration of 2019/2020 portfolio budget estimates. Pursuant to section 181(e) of the Standing Rules and Orders of the Legislative Assembly, I seek leave for the following Members to attend the public estimates hearings of the Committee, scheduled for Tuesday 23 July 2019: • Deb Frecklington MP, Member for Nanango • Tim Mander MP, Member for Everton • Jarrod Bleijie MP, Member for Kawana • Dr Christian Rowan MP, Member for Moggill • Ann Leahy MP, Member for Warrego • John-Paul Langbroek MP, Member for Surfers Paradise Should you have any queries, please contact Peter Coulson of my office. -
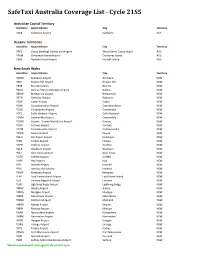
Safetaxi Australia Coverage List - Cycle 21S5
SafeTaxi Australia Coverage List - Cycle 21S5 Australian Capital Territory Identifier Airport Name City Territory YSCB Canberra Airport Canberra ACT Oceanic Territories Identifier Airport Name City Territory YPCC Cocos (Keeling) Islands Intl Airport West Island, Cocos Island AUS YPXM Christmas Island Airport Christmas Island AUS YSNF Norfolk Island Airport Norfolk Island AUS New South Wales Identifier Airport Name City Territory YARM Armidale Airport Armidale NSW YBHI Broken Hill Airport Broken Hill NSW YBKE Bourke Airport Bourke NSW YBNA Ballina / Byron Gateway Airport Ballina NSW YBRW Brewarrina Airport Brewarrina NSW YBTH Bathurst Airport Bathurst NSW YCBA Cobar Airport Cobar NSW YCBB Coonabarabran Airport Coonabarabran NSW YCDO Condobolin Airport Condobolin NSW YCFS Coffs Harbour Airport Coffs Harbour NSW YCNM Coonamble Airport Coonamble NSW YCOM Cooma - Snowy Mountains Airport Cooma NSW YCOR Corowa Airport Corowa NSW YCTM Cootamundra Airport Cootamundra NSW YCWR Cowra Airport Cowra NSW YDLQ Deniliquin Airport Deniliquin NSW YFBS Forbes Airport Forbes NSW YGFN Grafton Airport Grafton NSW YGLB Goulburn Airport Goulburn NSW YGLI Glen Innes Airport Glen Innes NSW YGTH Griffith Airport Griffith NSW YHAY Hay Airport Hay NSW YIVL Inverell Airport Inverell NSW YIVO Ivanhoe Aerodrome Ivanhoe NSW YKMP Kempsey Airport Kempsey NSW YLHI Lord Howe Island Airport Lord Howe Island NSW YLIS Lismore Regional Airport Lismore NSW YLRD Lightning Ridge Airport Lightning Ridge NSW YMAY Albury Airport Albury NSW YMDG Mudgee Airport Mudgee NSW YMER Merimbula -

Budget Car Rental in Australia Location Map
Budget Car Rental in Australia This GPS POI file is available here: https://www.gps-data-team.info/poi/australia/transportation/Budget-AU.html Location Map Budget Adelaide Airport Map Budget Adelaide City Map Budget Adelaide North Map Budget Adelaide South Map Budget Adelaide Trucks Map Budget Airport West Map Budget Albany Map Budget Albany Airport Map Budget Alexandria Map Budget Alice Springs Map Budget Alice Springs Airport Map Budget Alpha Map Budget Armidale Map Budget Armidale Airport Map Budget Artarmon Map Budget Ashmore Map Budget Avalon Airport Map Budget Bairnsdale Map Budget Balcatta Map Budget Ballarat Map Budget Ballina Map Budget Ballina Airport Map Budget Barcaldine Map Budget Bayswater Map Budget Bendigo Map Budget Biloela Map Budget Biloela (Thangool) Ai Map Budget Blacktown Map Budget Blackwater Map Budget Boondall Map Budget Box Hill Map Budget Brisbane Airport Map Budget Brisbane City Map Budget Brisbane East Map Budget Brisbane West Map Budget Broome Airport Map Budget Bunbury Map Budget Bundaberg Map Budget Burswood Map Budget Cairns Airport Map Page 1 Location Map Budget Cairns City Map Budget Caloundra Map Budget Camberwell Map Budget Campbellfield Map Budget Canberra Airport Map Budget Canberra City Map Budget Carnarvon Map Budget Carnarvon Airport Map Budget Ceduna Map Budget Ceduna Airport Map Budget Charleville Airport Map Budget Chinchilla Map Budget Clayton Map Budget Clermont Map Budget Coffs Harbour Map Budget Coffs Harbour Airport Map Budget Coober Pedy Map Budget Coolangatta Airport Map Budget Croydon -

Growing the Aviation Industry in the North and North West Queensland Region
Prepared for Regional Development Australia Townsville and North West Queensland Growing the Aviation Industry in the North and North West Queensland Region Proposal Reference RDATNWQ – Aviation Industry Attraction Plan th 06 August 2019 © QinetiQ Pty Ltd 2019 | Commercial in Confidence This document is supplied in confidence by QinetiQ to the Regional Development Australia Townsville and North West Queensland. Growing the Aviation Industry in the N and NW Queensland Region QinetiQ.com.au Contents 1. Executive Summary _________________________________________________________ 3 2. Overview __________________________________________________________________ 4 2.1. Aviation Sector Forecast Growth ____________________________________________ 6 2.2. References _____________________________________________________________ 8 3. SWOT analysis _____________________________________________________________ 9 3.1. Strengths ______________________________________________________________ 9 3.2. Weaknesses ___________________________________________________________ 9 3.3. Opportunities __________________________________________________________ 10 3.4. Threats _______________________________________________________________ 11 4. Explanatory Notes _________________________________________________________ 12 4.1. Table A. Explanatory Notes - Strengths ______________________________________ 12 4.2. Table B. Explanatory Notes - Weaknesses ___________________________________ 14 4.3. Table 3. Explanatory Notes – Threats _______________________________________ -

Rural and Regional Affairs and Transport References Committee
The Senate Rural and Regional Affairs and Transport References Committee Operation, regulation and funding of air route service delivery to rural, regional and remote communities June 2019 © Commonwealth of Australia 2019 ISBN 978-1-76010-979-0 This document was prepared by the Senate Standing Committee on Rural and Regional Affairs and Transport and printed by the Senate Printing Unit, Department of the Senate, Parliament House, Canberra. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Australia License. The details of this licence are available on the Creative Commons website: http://creativecommons.org/licenses/by-nc-nd/3.0/au/. Membership of the committee Members Senator Glenn Sterle, Chair Western Australia, ALP Senator Barry O'Sullivan, Deputy Chair Queensland, NATS Senator Slade Brockman Western Australia, LP Senator Anthony Chisholm Queensland, ALP Senator Malarndirri McCarthy (to prorogation of Parliament) Northern Territory, ALP Senator Janet Rice Victoria, AG Substitute members for this inquiry Senator Amanda Stoker Queensland, LP to replace Senator Barry O'Sullivan (24 July 2018 only) Senator Peter Whish-Wilson Tasmania, AG to replace Senator Janet Rice Other Senators participating in this inquiry Senator the Hon Richard Colbeck Tasmania, LP Senator Patrick Dodson Western Australia, ALP Senator Rex Patrick South Australia, CA iii Secretariat Dr Jane Thomson, Secretary Ms Sarah Redden, Principal Research Officer Ms Trish Carling, Senior Research Officer Ms Fiona Allen, Senior Research Officer Mr Michael Fisher, Administrative Officer PO Box 6100 Parliament House Canberra ACT 2600 Ph: 02 6277 3511 Fax: 02 6277 5811 E-mail: [email protected] Internet: www.aph.gov.au/senate_rrat iv Table of contents Membership of the committee ........................................................................ -

KODY LOTNISK ICAO Niniejsze Zestawienie Zawiera 8372 Kody Lotnisk
KODY LOTNISK ICAO Niniejsze zestawienie zawiera 8372 kody lotnisk. Zestawienie uszeregowano: Kod ICAO = Nazwa portu lotniczego = Lokalizacja portu lotniczego AGAF=Afutara Airport=Afutara AGAR=Ulawa Airport=Arona, Ulawa Island AGAT=Uru Harbour=Atoifi, Malaita AGBA=Barakoma Airport=Barakoma AGBT=Batuna Airport=Batuna AGEV=Geva Airport=Geva AGGA=Auki Airport=Auki AGGB=Bellona/Anua Airport=Bellona/Anua AGGC=Choiseul Bay Airport=Choiseul Bay, Taro Island AGGD=Mbambanakira Airport=Mbambanakira AGGE=Balalae Airport=Shortland Island AGGF=Fera/Maringe Airport=Fera Island, Santa Isabel Island AGGG=Honiara FIR=Honiara, Guadalcanal AGGH=Honiara International Airport=Honiara, Guadalcanal AGGI=Babanakira Airport=Babanakira AGGJ=Avu Avu Airport=Avu Avu AGGK=Kirakira Airport=Kirakira AGGL=Santa Cruz/Graciosa Bay/Luova Airport=Santa Cruz/Graciosa Bay/Luova, Santa Cruz Island AGGM=Munda Airport=Munda, New Georgia Island AGGN=Nusatupe Airport=Gizo Island AGGO=Mono Airport=Mono Island AGGP=Marau Sound Airport=Marau Sound AGGQ=Ontong Java Airport=Ontong Java AGGR=Rennell/Tingoa Airport=Rennell/Tingoa, Rennell Island AGGS=Seghe Airport=Seghe AGGT=Santa Anna Airport=Santa Anna AGGU=Marau Airport=Marau AGGV=Suavanao Airport=Suavanao AGGY=Yandina Airport=Yandina AGIN=Isuna Heliport=Isuna AGKG=Kaghau Airport=Kaghau AGKU=Kukudu Airport=Kukudu AGOK=Gatokae Aerodrome=Gatokae AGRC=Ringi Cove Airport=Ringi Cove AGRM=Ramata Airport=Ramata ANYN=Nauru International Airport=Yaren (ICAO code formerly ANAU) AYBK=Buka Airport=Buka AYCH=Chimbu Airport=Kundiawa AYDU=Daru Airport=Daru -

R20 Takes Flight Across Australia
cover winter 18.indd 1 08-May-18 8:57:56 AM INSIDE Master Volume 70 No 2 AIR FORCE ASSOCIATION PUBLICATION Editor Mark Eaton [email protected] PO Box 1269 Bondi Junction NSW 1355 57 President Carl Schiller OAMCSM Vice Presidents Governance Bob Bunney Advocacy & Entitlements Richard Kelloway OBE Communications & Media Lance Halvorson MBE Secretary Peter Colliver 22 10 [email protected] Treasurer Bob Robertson Publisher Flight Publishing Pty Ltd FEATURES REGULARS [email protected] DIVISION CONTACTS ACT [email protected] 0428 622 105 NSW [email protected] 10 6 National Council 02 9393 3485 The F-35A Lightning II QLD [email protected] 45 Air Force Today 0417 452 643 16 The Domino Theory SA [email protected] 08 8227 0980 52 Defence Talk TAS [email protected] 22 The Great Flight of the 03 6234 3862 Vimy 55 Australian Air League VIC [email protected] 03 9813 4600 28 Record of Luck 57 Air Force Cadets WA [email protected] 08 9288 4710 42 Magpie Painting 59 Briefing Room JOIN THE AIR FORCE ASSOCIATION 64 History Subscribe online at www.raafa.org.au, click on “ ” and follow Wings Archive Front Cover: 71 Veterans Information the prompts; pay via BPay or funds transfer via your bank. A 12 month A F-35A Lightning II departs RAAF subscription is $28.00, incl GST, within Base Amberley. 75 Books in Brief Australia and AUD36.00 for Asia and Pacific regional addresses. Photo Casey Gaul. Disclaimer All content in this Image has been digitally publication is copyright and may manipulated. -

List of Airports in Australia - Wikipedia
List of airports in Australia - Wikipedia https://en.wikipedia.org/wiki/List_of_airports_in_Australia List of airports in Australia This is a list of airports in Australia . It includes licensed airports, with the exception of private airports. Aerodromes here are listed with their 4-letter ICAO code, and 3-letter IATA code (where available). A more extensive list can be found in the En Route Supplement Australia (ERSA), available online from the Airservices Australia [1] web site and in the individual lists for each state or territory. Contents 1 Airports 1.1 Australian Capital Territory (ACT) 1.2 New South Wales (NSW) 1.3 Northern Territory (NT) 1.4 Queensland (QLD) 1.5 South Australia (SA) 1.6 Tasmania (TAS) 1.7 Victoria (VIC) 1.8 Western Australia (WA) 1.9 Other territories 1.10 Military: Air Force 1.11 Military: Army Aviation 1.12 Military: Naval Aviation 2 See also 3 References 4 Other sources Airports ICAO location indicators link to the Aeronautical Information Publication Enroute Supplement – Australia (ERSA) facilities (FAC) document, where available. Airport names shown in bold indicate the airport has scheduled passenger service on commercial airlines. Australian Capital Territory (ACT) City ICAO IATA Airport name served/location YSCB (https://www.airservicesaustralia.com/aip/current Canberra Canberra CBR /ersa/FAC_YSCB_17-Aug-2017.pdf) International Airport 1 of 32 11/28/2017 8:06 AM List of airports in Australia - Wikipedia https://en.wikipedia.org/wiki/List_of_airports_in_Australia New South Wales (NSW) City ICAO IATA Airport -
Answers to Questions on Notice Environment Portfolio
Senate Standing Committee on Environment and Communications Legislation Committee Answers to questions on notice Environment portfolio Question No: 203 Hearing: Budget Estimates Outcome: Corporate Programme: Corporate Strategies Division (CSD) Topic: Portfolio wide – land costs Hansard Page: N/A Question Date: 26 May 2014 Question Type: Written Senator Ludwig asked: How much land (if any) does the Department or agencies or authorities or Government corporation within each portfolio own or lease? a) Please list by each individual land holding, the size of the piece of land, the location of that piece of land and the latest valuation of that piece of land, where that land is owned or leased by the Department, or agency or authority or Government Corporation within that portfolio? (In regards to this question please ignore land upon which Australian Defence force bases are located. Non Defence Force base land is to be included) b) List the current assets, items or purse (buildings, facilities or other) on the land identified above. c) What is the current occupancy level and occupant of the items identified in (b)? d) What is the value of the items identified in (b)? e) What contractual or other arrangements are in place for the items identified in (b)? Answer: See attached tables. Senate Standing Committee on Environment and Communications Legislation Committee Answers to questions on notice Environment portfolio The Department of the Environment 1.2 hectares (a) Location Size Land Valuation (b) (c) (d) (e) Property (ha) Assets Occupancy Contractual Buildings arrangements Valuation Jabiru Field Station Ranger mine Estimate of Not Available 2 Laboratories, 40% Not Available Nil lease, East 1.2 Hectare 5 out buildings Department of Jabiru, NT the Environment.