Activity of Aztreonam in Combination with Ceftazidime-Avibactam Against
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ceftazidime for Injection) PHARMACY BULK PACKAGE – NOT for DIRECT INFUSION
PRESCRIBING INFORMATION FORTAZ® (ceftazidime for injection) PHARMACY BULK PACKAGE – NOT FOR DIRECT INFUSION To reduce the development of drug-resistant bacteria and maintain the effectiveness of FORTAZ and other antibacterial drugs, FORTAZ should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria. DESCRIPTION Ceftazidime is a semisynthetic, broad-spectrum, beta-lactam antibacterial drug for parenteral administration. It is the pentahydrate of pyridinium, 1-[[7-[[(2-amino-4 thiazolyl)[(1-carboxy-1-methylethoxy)imino]acetyl]amino]-2-carboxy-8-oxo-5-thia-1 azabicyclo[4.2.0]oct-2-en-3-yl]methyl]-, hydroxide, inner salt, [6R-[6α,7β(Z)]]. It has the following structure: The molecular formula is C22H32N6O12S2, representing a molecular weight of 636.6. FORTAZ is a sterile, dry-powdered mixture of ceftazidime pentahydrate and sodium carbonate. The sodium carbonate at a concentration of 118 mg/g of ceftazidime activity has been admixed to facilitate dissolution. The total sodium content of the mixture is approximately 54 mg (2.3 mEq)/g of ceftazidime activity. The Pharmacy Bulk Package vial contains 709 mg of sodium carbonate. The sodium content is approximately 54 mg (2.3mEq) per gram of ceftazidime. FORTAZ in sterile crystalline form is supplied in Pharmacy Bulk Packages equivalent to 6g of anhydrous ceftazidime. The Pharmacy Bulk Package bottle is a container of sterile preparation for parenteral use that contains many single doses. The contents are intended for use in a pharmacy admixture program and are restricted to the preparation of admixtures for intravenous use. THE PHARMACY BULK PACKAGE IS NOT FOR DIRECT INFUSION, FURTHER DILUTION IS REQUIRED BEFORE USE. -

Global Assessment of the Antimicrobial Activity of Polymyxin B Against 54 731 Clinical Isolates of Gram-Negative Bacilli
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector ORIGINAL ARTICLE 10.1111/j.1469-0691.2005.01351.x Global assessment of the antimicrobial activity of polymyxin B against 54 731 clinical isolates of Gram-negative bacilli: report from the SENTRY antimicrobial surveillance programme (2001–2004) A. C. Gales1, R. N. Jones2,3 and H. S. Sader1,2 1Division of Infectious Diseases, Universidade Federal de Sa˜o Paulo, Sa˜o Paulo, Brazil, 2JMI Laboratories, North Liberty, IA, USA, and 3Tufts University School of Medicine, Boston, MA, USA ABSTRACT In total, 54 731 Gram-negative bacilli isolated worldwide between 2001 and 2004 from diverse sites of infection were tested for susceptibility to polymyxin B by the broth reference microdilution method, with interpretation of results according to CLSI (formerly NCCLS) guidelines. Polymyxin B showed excellent potency and spectrum against 8705 Pseudomonas aeruginosa and 2621 Acinetobacter spp. isolates (MIC50, £ ⁄ ⁄ 1mg L and MIC90,2mg L for both pathogens). Polymyxin B resistance rates were slightly higher for carbapenem-resistant P. aeruginosa (2.7%) and Acinetobacter spp. (2.8%), or multidrug-resistant (MDR) P. aeruginosa (3.3%) and Acinetobacter spp. (3.2%), when compared with the entire group (1.3% for P. aeruginosa and 2.1% for Acinetobacter spp.). Among P. aeruginosa, polymyxin B resistance rates varied from 2.9% in the Asia-Pacific region to only 1.1% in Europe, Latin America and North America, while polymyxin B resistance rates ranged from 2.7% in Europe to 1.7% in North America and Latin America £ ⁄ % among Acinetobacter spp. -

FDA Drug Safety Communication: FDA Cautions About Dose Confusion and Medication Error with Antibacterial Drug Avycaz (Ceftazidime and Avibactam)
FDA Drug Safety Communication: FDA cautions about dose confusion and medication error with antibacterial drug Avycaz (ceftazidime and avibactam) Safety Announcement [09-22-2015] The U.S. Food and Drug Administration (FDA) is warning health care professionals about the risk for dosing errors with the intravenous antibacterial drug Avycaz (ceftazidime and avibactam) due to confusion about the drug strength displayed on the vial and carton labels. Avycaz was initially approved with the vial and carton labels displaying the individual strengths of the two active ingredients (i.e., 2 gram/0.5 gram); however, the product is dosed based on the sum of the active ingredients (i.e., 2.5 gram). To prevent medication errors, we have revised the labels to indicate that each vial contains Avycaz 2.5 gram, equivalent to ceftazidime 2 gram and avibactam 0.5 gram (see Photos). Avycaz is approved for intravenous administration to treat complicated infections in the urinary tract, or in combination with the antibacterial drug metronidazole to treat complicated infections in the abdomen in patients with limited or no alternative treatment options. Antibacterial drugs work by killing or stopping the growth of bacteria that can cause illness. Since Avycaz’s approval in February 2015, we have received reports of three medication error cases related to confusion on how the strength was displayed on the Avycaz vial and carton labels. Two cases stated that the errors occurred during preparation of the dose in the pharmacy. The third case described concern about the potential for confusion because the strength displayed for Avycaz differs from how the strength is displayed for other beta-lactam/beta-lactamase antibacterial drugs. -
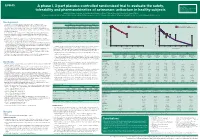
A Phase I, 3-Part Placebo-Controlled Randomised Trial to Evaluate the Safety, Tolerability and Pharmacokinetics of Aztreonam-Av
EV0643 Contactinformation: A phase I, 3-part placebo-controlled randomised trial to evaluate the safety, SeamusO’Brien AstraZenecaResearch&Development Macclesfield,Cheshire,UK tolerability and pharmacokinetics of aztreonam-avibactam in healthy subjects [email protected] Timi Edeki1, Diansong Zhou2, Frans van den Berg3, Helen Broadhurst4, William C. Holmes5, Gary Peters3, Maria Sunzel6, Seamus O’Brien4 1AstraZeneca, Wilmington, DE, USA; 2AstraZeneca, Waltham, MA, USA; 3Hammersmith Medicines Research, London, UK; 4AstraZeneca, Macclesfield, UK; 5AstraZeneca, Gaithersburg, MD, USA; 6Contractor at AstraZeneca, Wilmington, DE, USA Background Table 1.Subjects’baselinecharacteristics Figure 1. Geometricmean(A)aztreonamand(B)avibactamconcentration-timeprofilesinPartAfollowingindividualandcombinedadministrationofaztreonam2000mgandavibactam600mgby1-hIVinfusion Part A Part B Part C • Theemergenceandglobaldisseminationofmetallo-β-lactamase(MBL)-producing (A) (B) Enterobacteriaceae,includingNDM-typeandVIM-type,whichareresistanttocarbapenems, Active Placebo Active Placebo Active Placebo 100 Aztreonam 2000 mg alone (n=7) 100 Avibactam 600 mg alone (n=8) representsanurgentthreattohumanhealthforwhichfewtreatmentoptionscurrentlyexist.1, 2 (n=8) (n=4) (n=40) (n=16) (n=18) (n=6) Aztreonam-avibactam 2000-600 mg (n=7) Aztreonam-avibactam 2000-600 mg (n=7) • Aztreonam,amonobactamβ-lactam,isstabletoAmblerclassBMBLsincludingNDM-typeand Mean(SD)age,years 31(7) 34(7) 30(7) 27(5) 49(19) 51(19) VIM-type.However,bacteriathatexpressMBLsfrequentlyco-expressotherclassesofβ-lactamase -

Penicillin Allergy Guidance Document
Penicillin Allergy Guidance Document Key Points Background Careful evaluation of antibiotic allergy and prior tolerance history is essential to providing optimal treatment The true incidence of penicillin hypersensitivity amongst patients in the United States is less than 1% Alterations in antibiotic prescribing due to reported penicillin allergy has been shown to result in higher costs, increased risk of antibiotic resistance, and worse patient outcomes Cross-reactivity between truly penicillin allergic patients and later generation cephalosporins and/or carbapenems is rare Evaluation of Penicillin Allergy Obtain a detailed history of allergic reaction Classify the type and severity of the reaction paying particular attention to any IgE-mediated reactions (e.g., anaphylaxis, hives, angioedema, etc.) (Table 1) Evaluate prior tolerance of beta-lactam antibiotics utilizing patient interview or the electronic medical record Recommendations for Challenging Penicillin Allergic Patients See Figure 1 Follow-Up Document tolerance or intolerance in the patient’s allergy history Consider referring to allergy clinic for skin testing Created July 2017 by Macey Wolfe, PharmD; John Schoen, PharmD, BCPS; Scott Bergman, PharmD, BCPS; Sara May, MD; and Trevor Van Schooneveld, MD, FACP Disclaimer: This resource is intended for non-commercial educational and quality improvement purposes. Outside entities may utilize for these purposes, but must acknowledge the source. The guidance is intended to assist practitioners in managing a clinical situation but is not mandatory. The interprofessional group of authors have made considerable efforts to ensure the information upon which they are based is accurate and up to date. Any treatments have some inherent risk. Recommendations are meant to improve quality of patient care yet should not replace clinical judgment. -

Idweek16 CAZ-AVI PSA 1831.Pdf
Helio S. Sader, MD, PhD IDWEEK 2016 Antimicrobial Activity of Ceftazidime-Avibactam Tested Against Pseudomonas aeruginosa Isolates from JMI Laboratories 1831 North Liberty, IA, USA USA Hospitals Stratified by Site of Infection: Results from the INFORM Surveillance Program, 2013-2015 www.jmilabs.com HS SADER, M CASTANHEIRA, MD HUBAND, RK FLAMM ph. 319.665.3370 fax 319.665.3371 JMI Laboratories, North Liberty, Iowa, USA [email protected] Ceftazidime-avibactam is a combination agent consisting of the non-β- Table 1. Activity of ceftazidime-avibactam and comparator antimicrobial Figure 2. Antimicrobial activity of ceftazidime-avibactam, ceftazidime, Abstract lactam β-lactamase inhibitor avibactam and the broad-spectrum Results agents when tested against Pseudomonas aeruginosa from USA meropenem, and piperacillin-tazobactam when tested against P. aeruginosa cephalosporin, ceftazidime. Avibactam is a member of the hospitals (2013-2015). and stratified by site of infection. Background: Ceftazidime (CAZ)-avibactam (AVI) was approved by the United • Isolates were mostly from pneumonia (n=2,903; 52.9%), skin and skin diazabicyclooctanes (DBOs), a novel class of non-β-lactam β-lactamase MIC MIC CLSIa States Food and Drug Administration (US-FDA) for treatment of complicated intra- structure (SSSI; 1,286; 23.4%), bloodstream (BSI; 436; 7.9%), urinary Antimicrobial Agent 50 90 abdominal and urinary tract infections in 2015 and is under clinical development inhibitors which has a different mechanism of action when compared with (μg/mL) %S %I %R 100 tract (UTI; 417; 7.6%) and intra-abdominal infections (IAI; 199; 3.6%). All isolates (5,486) 90 for treatment of hospital-acquired pneumonia. -

Antimicrobial Activity of Ceftaroline Combined with Avibactam Tested Against Contemporary (2012) Helio S
Antimicrobial Activity of Ceftaroline Combined with Avibactam Tested Against Contemporary (2012) Helio S. Sader, MD, PhD JMI Laboratories Bacteria Collected from USA Patients with Acute Bacterial Skin and Skin Structure Infections (ABSSSIs) North Liberty, IA, USA ECCMID 2013 www.jmilabs.com HS SADER, RK FLAMM, RN JONES ph. 319.665.3370 P1620 fax 319.665.3371 JMI Laboratories, North Liberty, Iowa, USA [email protected] Table 2. Antimicrobial activities of ceftaroline-avibactam, ceftaroline and comparator agents when tested against gram-negative organisms from Abstract Introduction Results skin and skin structure infections (USA, 2012). Conclusions Objective: To evaluate the activity of ceftaroline Ceftaroline, the active metabolite of the prodrug ceftaroline • The most common organisms were S. aureus (3,481; Organism (no tested)/ MIC (mg/L) %S / %I / %R • Ceftaroline-avibactam was highly active antimicrobial agent 50% 90% Range CLSIa EUCASTa (CPT)-avibactam (AVI) tested against bacteria from fosamil, is a cephalosporin with notable in vitro bactericidal 50.5% MRSA), E. coli (444; 13.3% ESBL-phenotype), β- E. coli (444) against ESBL-phenotype and carbapenem- ABSSSI collected in USA hospitals in 2012. CPT activity against organisms commonly responsible for haemolytic streptococci (βHS; 389) and Klebsiella spp. Ceftaroline-avibactam 0.03 0.06 ≤0.015 – 0.5 - / - / - - / - / - non-susceptible Enterobacteriaceae Ceftaroline 0.12 32 ≤0.015 – >32 83.3 / 2.7 / 14.0 83.3 / 0.0 / 16.7 fosamil is a novel parenteral cephalosporin community-acquired -

Cephalosporins Can Be Prescribed Safely for Penicillin-Allergic Patients ▲
JFP_0206_AE_Pichichero.Final 1/23/06 1:26 PM Page 106 APPLIED EVIDENCE New research findings that are changing clinical practice Michael E. Pichichero, MD University of Rochester Cephalosporins can be Medical Center, Rochester, NY prescribed safely for penicillin-allergic patients Practice recommendations an allergic reaction to cephalosporins, ■ The widely quoted cross-allergy risk compared with the incidence of a primary of 10% between penicillin and (and unrelated) cephalosporin allergy. cephalosporins is a myth (A). Most people produce IgG and IgM antibodies in response to exposure to ■ Cephalothin, cephalexin, cefadroxil, penicillin1 that may cross-react with and cefazolin confer an increased risk cephalosporin antigens.2 The presence of of allergic reaction among patients these antibodies does not predict allergic, with penicillin allergy (B). IgE cross-sensitivity to a cephalosporin. ■ Cefprozil, cefuroxime, cefpodoxime, Even penicillin skin testing is generally not ceftazidime, and ceftriaxone do not predictive of cephalosporin allergy.3 increase risk of an allergic reaction (B). Reliably predicting cross-reactivity ndoubtedly you have patients who A comprehensive review of the evidence say they are allergic to penicillin shows that the attributable risk of a cross- U but have difficulty recalling details reactive allergic reaction varies and is of the reactions they experienced. To be strongest when the chemical side chain of safe, we often label these patients as peni- the specific cephalosporin is similar to that cillin-allergic without further questioning of penicillin or amoxicillin. and withhold not only penicillins but Administration of cephalothin, cepha- cephalosporins due to concerns about lexin, cefadroxil, and cefazolin in penicillin- potential cross-reactivity and resultant IgE- allergic patients is associated with a mediated, type I reactions. -

Successful Treatment of Ventriculitis Caused by MDR/XDR Gram-Negative Bacillus Using Ceftazidime/Avibactam: Case Series and Literature Review
Infection and Drug Resistance Dovepress open access to scientific and medical research Open Access Full Text Article CASE SERIES Successful Treatment of Ventriculitis Caused by MDR/XDR Gram-Negative Bacillus Using Ceftazidime/Avibactam: Case Series and Literature Review Qian Zhou1 Background: Central nervous system (CNS) infections caused by multidrug-resistant Hao Wang2 (MDR) and extensively drug-resistant (XDR) Gram-negative bacillus, including carbape Tianxiang Zhan2 nem-resistant Enterobacteriaceae (CRE) and Pseudomonas aeruginosa, are associated with Xiaofeng Yang1,2 high mortality rates. Clinical trials of ceftazidime/avibactam (CAZ/AVI) on infections of Liang Wen2 other systems indicate that they are effective against these infections. However, clinical studies on the efficacies of CAZ/AVI in the treatment of CNS infections have not been done. 1 Department of Emergency and Trauma Case Presentation: We evaluated 3 patients diagnosed with MDR/XDR Gram-negative Center, The International Medical Center, The First Affiliated Hospital, bacillus-associated CNS infections, and effectively treated with CAZ/AVI. Moreover, we Zhejiang University School of Medicine, performed literature reviews. Before the onset of CNS infections, the 3 patients were Hangzhou, Zhejiang Province, 310003, subjected to neurosurgical operations, treated with mechanical ventilation, long-term inten People’s Republic of China; 2Department of Neurosurgery, The First Affiliated sive care unit therapy, and various antibiotics. By intravenously administering CAZ/AVI, Hospital, Zhejiang University School of combined with another antibiotic, the MDR/XDR K. pneumoniae and P. aeruginosa asso Medicine, Hangzhou, Zhejiang Province, 310003, People’s Republic of China ciated ventriculitis was effectively treated in the 3 patients. Conclusion: CAZ/AVI is a viable treatment option for CNS infections caused by MDR/ XDR Gram-negative bacteria. -

辻氏②P1314(900X1900)
P1314 Surveillance of Cefiderocol In Vitro Activity against Gram-Negative Clinical Isolates Collected Contact Information : Masakatsu Tsuji in Europe: SIDERO-WT-2014 Address: 3-1-1, Futaba-cho, Toyonaka, Osaka, 561-0825, JAPAN TEL: +81-6-6331-8272 27th ECCMID 1) 2) 1) 3) 2) FAX: +81-6-6331-8612 Masakatsu Tsuji , Meredith Hackel , Yoshinori Yamano , Roger Echols and Daniel F Sahm E-mail address: [email protected] Vienna, Austria 22-25 April, 2017 1) Shionogi & Co., Ltd., Osaka JP, 2) IHMA, Inc. Schaumburg, IL, US, 3) ID3C, LLC, Easton CT, US Compound testing cefiderocol, iron-deficient cation-adjusted Muller-Hinton Broth ABSTRACT Cefiderocol, cefepime, ceftazidime-avibactam, ceftolozane-tazobactam, (ID-CAMHB) was used according to CLSI approved guidelines (3, 4). The RESULTS Background: ciprofloxacin, colistin and meropenem were used. cefiderocol MIC was read as the first drug well in which the growth was significantly reduced (i.e. a button of < 1 mm or light/faint turbidity) relative • Cefiderocol MIC50 and MIC90 values were the lowest of all compounds tested (Table 2, Figure 3-5). Figure 4. Cumulative percentage of cefiderocol MIC against 570 carbapenem- The emergence and dissemination of potent resistance mechanisms among Gram-negative bacterial Antimicrobial Susceptibility Testing to the growth observed in the growth control. Escherichia coli ATCC 25922 • The cefiderocol MIC90 value was 1 mg/L for all Enterobacteriaceae and 4 mg/L for resistant A. baumanii from EU. species underscores the need for the development of new and effective therapeutic choices to treat Antimicrobial susceptibility testing was done using broth microdilution meropenem-resistant Enterobacteriaceae. -

CLSI AST News Update Janet A
Volume 3, Issue 2 Spring 2018 CLSI Subcommittee on Antimicrobial Susceptibility Testing CLSI AST News Update Janet A. Hindler, MCLS MT(ASCP) F(AAM), Editor Audrey N. Schuetz, MD, MPH, D(ABMM), Editor The CLSI Outreach Working Group (ORWG) is providing this Newsletter to highlight some recent issues related to antimicrobial susceptibility testing Inside This Issue: and reporting. We are listing links to some new educational materials and reminding you where you can find information about the CLSI AST Featured Article: Part 1 Subcommittee proceedings. New β-lactam combination agents for the treatment of Gram-negative bacterial infections: what the clinical microbiologist needs to know! ..................................................4 Upcoming Webinar: Featured Article: Part 2 Why all the fuss over quality control of Preparation, Presentation, and Promotion of Cumulative Antibiograms To β-lactam combination agents? ........................8 Support Antimicrobial Stewardship Programs Case Study: Cefazolin, Urine, and October 16, 2018 | 1:00–2:00 PM Eastern (US) Time Escherichia coli, Klebsiella pneumoniae, and Presenters: Proteus mirabilis: Entertaining Solutions Sharon Erdman, PharmD for Antimicrobial Susceptibility Testing and Clinical Professor, Purdue University College of Pharmacy Reporting ..........................................................12 Infectious Diseases Clinical Pharmacist/Co-Director OPAT Program, Eskenazi Health Burning Question: What Should Clinical Laboratorians Know About Gonorrhea in Patricia J. Simner, PhD, D(ABMM) 2018? ................................................................15 Associate Professor of Pathology, Johns Hopkins University Director of Medical Bacteriology and Parasitology Laboratories, Johns Hopkins Hot Topic: It’s Enough to mec You Crazy! ...18 Hospital What does the CLSI AST Subcommittee do? The first edition of the CLSI AST News Update (Vol 1, Issue 1, Spring 2016) described details about the organization and operation of the CLSI AST Subcommittee. -

Determining the Optimal Dosing of a Novel Combination Regimen of Ceftazidime/Avibactam with Aztreonam Against NDM-1-Producing En
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/341736616 Determining the optimal dosing of a novel combination regimen of ceftazidime/avibactam with aztreonam against NDM-1-producing Enterobacteriaceae using a hollow-fibre infection mode... Article in Journal of Antimicrobial Chemotherapy · May 2020 DOI: 10.1093/jac/dkaa197 CITATIONS READS 2 52 13 authors, including: Thomas Lodise Nicholas M. Smith Albany College of Pharmacy and Health Sciences University at Buffalo, The State University of New York 282 PUBLICATIONS 7,722 CITATIONS 14 PUBLICATIONS 71 CITATIONS SEE PROFILE SEE PROFILE John Nicholas O'Donnell Patricia N Holden Albany College of Pharmacy and Health Sciences University at Buffalo, The State University of New York 35 PUBLICATIONS 193 CITATIONS 34 PUBLICATIONS 439 CITATIONS SEE PROFILE SEE PROFILE Some of the authors of this publication are also working on these related projects: Biochemical and structural studies on beta-lactamases from pathogens and metagenomic origin View project Clarifying the role of cephalosporins in the management of MSSA infection View project All content following this page was uploaded by Jieqiang Zhou on 12 October 2020. The user has requested enhancement of the downloaded file. J Antimicrob Chemother 2020; 75: 2622–2632 doi:10.1093/jac/dkaa197 Advance Access publication 28 May 2020 Determining the optimal dosing of a novel combination regimen of ceftazidime/avibactam with aztreonam against NDM-1-producing Enterobacteriaceae using a hollow-fibre infection model Downloaded from https://academic.oup.com/jac/article/75/9/2622/5848380 by University of Florida user on 12 October 2020 Thomas P.