Global Trends of Antimicrobial Susceptibility of Ceftaroline and Ceftazidime-Avibactam: a Surveillance Study from the ATLAS Program (2012- 2016)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Polymyxin B in Combination with Doripenem Against Heteroresistant Acinetobacter Baumannii: Pharmacodynamics of New Dosing Strategies
J Antimicrob Chemother 2016; 71: 3148–3156 doi:10.1093/jac/dkw293 Advance Access publication 3 August 2016 Polymyxin B in combination with doripenem against heteroresistant Acinetobacter baumannii: pharmacodynamics of new dosing strategies Gauri G. Rao1,2, Neang S. Ly1,2,Ju¨rgen B. Bulitta1,3, Rachel L. Soon1,2, Marie D. San Roman1,2, Patricia N. Holden1,2, Cornelia B. Landersdorfer4, Roger L. Nation4, Jian Li4, Alan Forrest1,5 and Brian T. Tsuji1,2* 1Laboratory for Antimicrobial Pharmacodynamics, School of Pharmacy and Pharmaceutical Sciences, University at Buffalo, The State University of New York, Buffalo, NY, USA; 2The New York State Center of Excellence in Bioinformatics & Life Sciences, University at Buffalo, The State University of New York, Buffalo, NY, USA; 3Center for Pharmacometrics and Systems Pharmacology, College of Pharmacy, University of Florida, Orlando, FL, USA; 4Drug Delivery, Disposition and Dynamics, Monash Institute of Pharmaceutical Sciences, Monash University, Melbourne, Australia; 5Eshelman School of Pharmacy, The University of North Carolina at Chapel Hill, NC, USA *Corresponding author. Tel: +1-716-881-7543; Fax: +1-716-849-6890; E-mail: [email protected] Received 13 October 2015; returned 3 January 2016; revised 14 June 2016; accepted 19 June 2016 Objectives: Polymyxin B is being increasingly utilized as a last resort against resistant Gram-negative bacteria. We examined the pharmacodynamics of novel dosing strategies for polymyxin B combinations to maximize efficacy and minimize the emergence of resistance and drug exposure against Acinetobacter baumannii. Methods: The pharmacodynamics of polymyxin B together with doripenem were evaluated in time–kill experi- ments over 48 h against 108 cfu/mL of two polymyxin-heteroresistant A. -

Medical Review(S) Clinical Review
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 200327 MEDICAL REVIEW(S) CLINICAL REVIEW Application Type NDA Application Number(s) 200327 Priority or Standard Standard Submit Date(s) December 29, 2009 Received Date(s) December 30, 2009 PDUFA Goal Date October 30, 2010 Division / Office Division of Anti-Infective and Ophthalmology Products Office of Antimicrobial Products Reviewer Name(s) Ariel Ramirez Porcalla, MD, MPH Neil Rellosa, MD Review Completion October 29, 2010 Date Established Name Ceftaroline fosamil for injection (Proposed) Trade Name Teflaro Therapeutic Class Cephalosporin; ß-lactams Applicant Cerexa, Inc. Forest Laboratories, Inc. Formulation(s) 400 mg/vial and 600 mg/vial Intravenous Dosing Regimen 600 mg every 12 hours by IV infusion Indication(s) Acute Bacterial Skin and Skin Structure Infection (ABSSSI); Community-acquired Bacterial Pneumonia (CABP) Intended Population(s) Adults ≥ 18 years of age Template Version: March 6, 2009 Reference ID: 2857265 Clinical Review Ariel Ramirez Porcalla, MD, MPH Neil Rellosa, MD NDA 200327: Teflaro (ceftaroline fosamil) Table of Contents 1 RECOMMENDATIONS/RISK BENEFIT ASSESSMENT ......................................... 9 1.1 Recommendation on Regulatory Action ........................................................... 10 1.2 Risk Benefit Assessment.................................................................................. 10 1.3 Recommendations for Postmarketing Risk Evaluation and Mitigation Strategies ........................................................................................................................ -

Ceftazidime for Injection) PHARMACY BULK PACKAGE – NOT for DIRECT INFUSION
PRESCRIBING INFORMATION FORTAZ® (ceftazidime for injection) PHARMACY BULK PACKAGE – NOT FOR DIRECT INFUSION To reduce the development of drug-resistant bacteria and maintain the effectiveness of FORTAZ and other antibacterial drugs, FORTAZ should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria. DESCRIPTION Ceftazidime is a semisynthetic, broad-spectrum, beta-lactam antibacterial drug for parenteral administration. It is the pentahydrate of pyridinium, 1-[[7-[[(2-amino-4 thiazolyl)[(1-carboxy-1-methylethoxy)imino]acetyl]amino]-2-carboxy-8-oxo-5-thia-1 azabicyclo[4.2.0]oct-2-en-3-yl]methyl]-, hydroxide, inner salt, [6R-[6α,7β(Z)]]. It has the following structure: The molecular formula is C22H32N6O12S2, representing a molecular weight of 636.6. FORTAZ is a sterile, dry-powdered mixture of ceftazidime pentahydrate and sodium carbonate. The sodium carbonate at a concentration of 118 mg/g of ceftazidime activity has been admixed to facilitate dissolution. The total sodium content of the mixture is approximately 54 mg (2.3 mEq)/g of ceftazidime activity. The Pharmacy Bulk Package vial contains 709 mg of sodium carbonate. The sodium content is approximately 54 mg (2.3mEq) per gram of ceftazidime. FORTAZ in sterile crystalline form is supplied in Pharmacy Bulk Packages equivalent to 6g of anhydrous ceftazidime. The Pharmacy Bulk Package bottle is a container of sterile preparation for parenteral use that contains many single doses. The contents are intended for use in a pharmacy admixture program and are restricted to the preparation of admixtures for intravenous use. THE PHARMACY BULK PACKAGE IS NOT FOR DIRECT INFUSION, FURTHER DILUTION IS REQUIRED BEFORE USE. -

Activity of Aztreonam in Combination with Ceftazidime-Avibactam Against
Diagnostic Microbiology and Infectious Disease 99 (2021) 115227 Contents lists available at ScienceDirect Diagnostic Microbiology and Infectious Disease journal homepage: www.elsevier.com/locate/diagmicrobio Activity of aztreonam in combination with ceftazidime–avibactam against serine- and metallo-β-lactamase–producing ☆ ☆☆ ★ Pseudomonas aeruginosa , , Michelle Lee a, Taylor Abbey a, Mark Biagi b, Eric Wenzler a,⁎ a College of Pharmacy, University of Illinois at Chicago, Chicago, IL, USA b College of Pharmacy, University of Illinois at Chicago, Rockford, IL, USA article info abstract Article history: Existing data support the combination of aztreonam and ceftazidime–avibactam against serine-β-lactamase Received 29 June 2020 (SBL)– and metallo-β-lactamase (MBL)–producing Enterobacterales, although there is a paucity of data against Received in revised form 15 September 2020 SBL- and MBL-producing Pseudomonas aeruginosa. In this study, 5 SBL- and MBL-producing P. aeruginosa (1 Accepted 19 September 2020 IMP, 4 VIM) were evaluated against aztreonam and ceftazidime–avibactam alone and in combination via broth Available online xxxx microdilution and time-kill analyses. All 5 isolates were nonsusceptible to aztreonam, aztreonam–avibactam, – – Keywords: and ceftazidime avibactam. Combining aztreonam with ceftazidime avibactam at subinhibitory concentrations Metallo-β-lactamase produced synergy and restored bactericidal activity in 4/5 (80%) isolates tested. These results suggest that the VIM combination of aztreonam and ceftazidime–avibactam may be a viable treatment option against SBL- and IMP MBL-producing P. aeruginosa. Aztreonam © 2020 Elsevier Inc. All rights reserved. Ceftazidime–avibactam Synergy 1. Introduction of SBLs and MBLs harbored by P. aeruginosa are fundamentally different than those in Enterobacterales (Alm et al., 2015; Kazmierczak et al., The rapid global dissemination of Ambler class B metallo-β- 2016; Periasamy et al., 2020; Poirel et al., 2000; Watanabe et al., lactamase (MBL) enzymes along with their increasing diversity across 1991). -

Global Assessment of the Antimicrobial Activity of Polymyxin B Against 54 731 Clinical Isolates of Gram-Negative Bacilli
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector ORIGINAL ARTICLE 10.1111/j.1469-0691.2005.01351.x Global assessment of the antimicrobial activity of polymyxin B against 54 731 clinical isolates of Gram-negative bacilli: report from the SENTRY antimicrobial surveillance programme (2001–2004) A. C. Gales1, R. N. Jones2,3 and H. S. Sader1,2 1Division of Infectious Diseases, Universidade Federal de Sa˜o Paulo, Sa˜o Paulo, Brazil, 2JMI Laboratories, North Liberty, IA, USA, and 3Tufts University School of Medicine, Boston, MA, USA ABSTRACT In total, 54 731 Gram-negative bacilli isolated worldwide between 2001 and 2004 from diverse sites of infection were tested for susceptibility to polymyxin B by the broth reference microdilution method, with interpretation of results according to CLSI (formerly NCCLS) guidelines. Polymyxin B showed excellent potency and spectrum against 8705 Pseudomonas aeruginosa and 2621 Acinetobacter spp. isolates (MIC50, £ ⁄ ⁄ 1mg L and MIC90,2mg L for both pathogens). Polymyxin B resistance rates were slightly higher for carbapenem-resistant P. aeruginosa (2.7%) and Acinetobacter spp. (2.8%), or multidrug-resistant (MDR) P. aeruginosa (3.3%) and Acinetobacter spp. (3.2%), when compared with the entire group (1.3% for P. aeruginosa and 2.1% for Acinetobacter spp.). Among P. aeruginosa, polymyxin B resistance rates varied from 2.9% in the Asia-Pacific region to only 1.1% in Europe, Latin America and North America, while polymyxin B resistance rates ranged from 2.7% in Europe to 1.7% in North America and Latin America £ ⁄ % among Acinetobacter spp. -

FDA Drug Safety Communication: FDA Cautions About Dose Confusion and Medication Error with Antibacterial Drug Avycaz (Ceftazidime and Avibactam)
FDA Drug Safety Communication: FDA cautions about dose confusion and medication error with antibacterial drug Avycaz (ceftazidime and avibactam) Safety Announcement [09-22-2015] The U.S. Food and Drug Administration (FDA) is warning health care professionals about the risk for dosing errors with the intravenous antibacterial drug Avycaz (ceftazidime and avibactam) due to confusion about the drug strength displayed on the vial and carton labels. Avycaz was initially approved with the vial and carton labels displaying the individual strengths of the two active ingredients (i.e., 2 gram/0.5 gram); however, the product is dosed based on the sum of the active ingredients (i.e., 2.5 gram). To prevent medication errors, we have revised the labels to indicate that each vial contains Avycaz 2.5 gram, equivalent to ceftazidime 2 gram and avibactam 0.5 gram (see Photos). Avycaz is approved for intravenous administration to treat complicated infections in the urinary tract, or in combination with the antibacterial drug metronidazole to treat complicated infections in the abdomen in patients with limited or no alternative treatment options. Antibacterial drugs work by killing or stopping the growth of bacteria that can cause illness. Since Avycaz’s approval in February 2015, we have received reports of three medication error cases related to confusion on how the strength was displayed on the Avycaz vial and carton labels. Two cases stated that the errors occurred during preparation of the dose in the pharmacy. The third case described concern about the potential for confusion because the strength displayed for Avycaz differs from how the strength is displayed for other beta-lactam/beta-lactamase antibacterial drugs. -
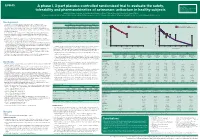
A Phase I, 3-Part Placebo-Controlled Randomised Trial to Evaluate the Safety, Tolerability and Pharmacokinetics of Aztreonam-Av
EV0643 Contactinformation: A phase I, 3-part placebo-controlled randomised trial to evaluate the safety, SeamusO’Brien AstraZenecaResearch&Development Macclesfield,Cheshire,UK tolerability and pharmacokinetics of aztreonam-avibactam in healthy subjects [email protected] Timi Edeki1, Diansong Zhou2, Frans van den Berg3, Helen Broadhurst4, William C. Holmes5, Gary Peters3, Maria Sunzel6, Seamus O’Brien4 1AstraZeneca, Wilmington, DE, USA; 2AstraZeneca, Waltham, MA, USA; 3Hammersmith Medicines Research, London, UK; 4AstraZeneca, Macclesfield, UK; 5AstraZeneca, Gaithersburg, MD, USA; 6Contractor at AstraZeneca, Wilmington, DE, USA Background Table 1.Subjects’baselinecharacteristics Figure 1. Geometricmean(A)aztreonamand(B)avibactamconcentration-timeprofilesinPartAfollowingindividualandcombinedadministrationofaztreonam2000mgandavibactam600mgby1-hIVinfusion Part A Part B Part C • Theemergenceandglobaldisseminationofmetallo-β-lactamase(MBL)-producing (A) (B) Enterobacteriaceae,includingNDM-typeandVIM-type,whichareresistanttocarbapenems, Active Placebo Active Placebo Active Placebo 100 Aztreonam 2000 mg alone (n=7) 100 Avibactam 600 mg alone (n=8) representsanurgentthreattohumanhealthforwhichfewtreatmentoptionscurrentlyexist.1, 2 (n=8) (n=4) (n=40) (n=16) (n=18) (n=6) Aztreonam-avibactam 2000-600 mg (n=7) Aztreonam-avibactam 2000-600 mg (n=7) • Aztreonam,amonobactamβ-lactam,isstabletoAmblerclassBMBLsincludingNDM-typeand Mean(SD)age,years 31(7) 34(7) 30(7) 27(5) 49(19) 51(19) VIM-type.However,bacteriathatexpressMBLsfrequentlyco-expressotherclassesofβ-lactamase -

Colistin Combinations Veterinary Medicinal Products Were Identified with Colistin Doses of Below 50,000 IU Per Kg Body Weight
Annex I List of the names, pharmaceutical forms, strengths of the veterinary medicinal products, animal species, route of administration, and marketing authorisation holders in the Member States Member Marketing Name INN Strength Pharmaceutical Animal Route of State authorisation form species administration EU/EEA holder Bulgaria Farma vet Ltd. Колитетравит / Oxytetracycline 5.0 g Oral solution Chickens and Oral 40 Otec Paisii str. COLI – TETRAVIT hydrochloride pigs administration Shumen Colistin sulphate 3 500 000 Bulgaria UI Bulgaria COOPHAVET S.A.S. Колисултрикс/ Trimethoprim 3.75 g Oral powder Chickens, Oral administration B.P. 7 Saint Herblon COLISULTRIX Colistin sulphate 50 MIU rabbits, pigs, 44153 ANCENIS calves and Cedex lambs France Croatia Arnika Veterina COLISULTRIX Trimethoprim 3.75 g Oral powder Calves, lambs, Oral d.o.o. Colistin sulphate 50 MIU kids, piglets, Vodovodna 20a poultry and 10000 Zagreb rabbits Croatia Croatia Ceva Santé Animale QUINOCOL Enrofloxacin 100 g Oral solution Chicken, Oral 10 Avenue de la Colistin sulphate 41.67 g turkey Ballastière 33500 Libourne France Cyprus FATRO S.p.A. BACOLAM powder Amoxicillin trihydrate 100 mg Powder for oral Calves, sheep, Administer the Via Emilia, 285 for oral solution for Colistin sulphate 500,000 solution goats, pigs, dose subdivided 40064 Ozzano Emilia calves, sheep, I.U. foals, into two (Bologna) goats, pigs, foals, chickens, administrations Italy chickens, turkeys turkeys each day, (excluding layers) (excluding dissolved in layers) drinking water or in milk. 2/24 Member Marketing Name INN Strength Pharmaceutical Animal Route of State authorisation form species administration EU/EEA holder Cyprus Vetoquinol Italia ZEMAMIX premix for Amoxicillin trihydrate 11.48 g Premix for Pigs Premix for S.R.L medicated Colistin sulphate 4.00 g medicated medicated Via Piana, 265 feedingstuff for pigs feedingstuff feedingstuff in 47032 Bertinoro insoluble powder, Italy to be administered orally properly mixed in solid feed. -

Penicillin Allergy Guidance Document
Penicillin Allergy Guidance Document Key Points Background Careful evaluation of antibiotic allergy and prior tolerance history is essential to providing optimal treatment The true incidence of penicillin hypersensitivity amongst patients in the United States is less than 1% Alterations in antibiotic prescribing due to reported penicillin allergy has been shown to result in higher costs, increased risk of antibiotic resistance, and worse patient outcomes Cross-reactivity between truly penicillin allergic patients and later generation cephalosporins and/or carbapenems is rare Evaluation of Penicillin Allergy Obtain a detailed history of allergic reaction Classify the type and severity of the reaction paying particular attention to any IgE-mediated reactions (e.g., anaphylaxis, hives, angioedema, etc.) (Table 1) Evaluate prior tolerance of beta-lactam antibiotics utilizing patient interview or the electronic medical record Recommendations for Challenging Penicillin Allergic Patients See Figure 1 Follow-Up Document tolerance or intolerance in the patient’s allergy history Consider referring to allergy clinic for skin testing Created July 2017 by Macey Wolfe, PharmD; John Schoen, PharmD, BCPS; Scott Bergman, PharmD, BCPS; Sara May, MD; and Trevor Van Schooneveld, MD, FACP Disclaimer: This resource is intended for non-commercial educational and quality improvement purposes. Outside entities may utilize for these purposes, but must acknowledge the source. The guidance is intended to assist practitioners in managing a clinical situation but is not mandatory. The interprofessional group of authors have made considerable efforts to ensure the information upon which they are based is accurate and up to date. Any treatments have some inherent risk. Recommendations are meant to improve quality of patient care yet should not replace clinical judgment. -

Polymyxin B & Colistin Dosing Tip Sheet
Stanford Antimicrobial Safety & Sustainability Program Polymyxin B & Colistin Dosing Tip Sheet What: Polymyxin B is preferred over Colistin (polymyxin E) for infections due to multidrug resistant gram- negative bacilli at Stanford Health Care. SHC formulary restriction criteria – Polymyxin B 1. Infectious Disease Consultation and ID recommendation for use 2. Cystic Fibrosis team SHC formulary restriction criteria – Colistin 1. Treatment of urinary tract infections 2. Inhalation route Why: Polymyxin B and Colistin have the same spectrum of activity. However, Polymyxin B has favorable clinical pharmacologic properties compared to Colistin o Polymyxin B is an active drug, whereas Colistin is administered as the prodrug colistimethate sodium (CMS) and has variable and slow (hours) conversion to the active moiety o Polymyxin B may be less nephrotoxic How: Polymyxin B and Colistin dosing is NOT interchangeable o Polymyxin B is usually dosed by “unit”, not “mg” o Note that with Polymyxin B, each 500,000 units is diluted in 300-500mL: a typical dose may result in 1L of fluid o Consult ID pharmacists if MIC ≥ 2 for alternative dosing strategies Dosing 50-79 30-49 10-29 IHD Route ≥80 mL/min mL/min mL/min mL/min CRRT Polymyxin B No Data; Use actual body IV 7,500 – 12,500 units/kg Q12H Consult ID weight; adjusted body wt for obese pharmacist 2.5 mg/kg 1.5 mg/kg 5 mg/kg/day 1.25–1.9 mg/kg Q24H 1.5 mg/kg Q24-48h Colistin IV in 2-3 divided -OR- Use ideal body Q12H Q36H 2.5 mg/kg weight doses 1.25 mg/kg Q12h Q12-24H Doses expressed in colistin base activity Inhalation 150 mg inhalation Q12H Conversions: Colistimethate sodium 1 mg = ~12,500 units of colistimethate sodium Colistimethate sodium ~2.67 mg = 1 mg of colistin base activity 1 mg colistin base activity (CBA) = 30,000 IU colistin 1 mg polymyxin B = 10,000 IU polymyxin B Orig date: 2/23/2015 LM, EM Stanford Antimicrobial Safety & Sustainability Program References: Micromedex online, accessed 2/17/2016 Nelson, Brian C., et al. -

Idweek16 CAZ-AVI PSA 1831.Pdf
Helio S. Sader, MD, PhD IDWEEK 2016 Antimicrobial Activity of Ceftazidime-Avibactam Tested Against Pseudomonas aeruginosa Isolates from JMI Laboratories 1831 North Liberty, IA, USA USA Hospitals Stratified by Site of Infection: Results from the INFORM Surveillance Program, 2013-2015 www.jmilabs.com HS SADER, M CASTANHEIRA, MD HUBAND, RK FLAMM ph. 319.665.3370 fax 319.665.3371 JMI Laboratories, North Liberty, Iowa, USA [email protected] Ceftazidime-avibactam is a combination agent consisting of the non-β- Table 1. Activity of ceftazidime-avibactam and comparator antimicrobial Figure 2. Antimicrobial activity of ceftazidime-avibactam, ceftazidime, Abstract lactam β-lactamase inhibitor avibactam and the broad-spectrum Results agents when tested against Pseudomonas aeruginosa from USA meropenem, and piperacillin-tazobactam when tested against P. aeruginosa cephalosporin, ceftazidime. Avibactam is a member of the hospitals (2013-2015). and stratified by site of infection. Background: Ceftazidime (CAZ)-avibactam (AVI) was approved by the United • Isolates were mostly from pneumonia (n=2,903; 52.9%), skin and skin diazabicyclooctanes (DBOs), a novel class of non-β-lactam β-lactamase MIC MIC CLSIa States Food and Drug Administration (US-FDA) for treatment of complicated intra- structure (SSSI; 1,286; 23.4%), bloodstream (BSI; 436; 7.9%), urinary Antimicrobial Agent 50 90 abdominal and urinary tract infections in 2015 and is under clinical development inhibitors which has a different mechanism of action when compared with (μg/mL) %S %I %R 100 tract (UTI; 417; 7.6%) and intra-abdominal infections (IAI; 199; 3.6%). All isolates (5,486) 90 for treatment of hospital-acquired pneumonia. -

Antimicrobial Activity of Ceftaroline Combined with Avibactam Tested Against Contemporary (2012) Helio S
Antimicrobial Activity of Ceftaroline Combined with Avibactam Tested Against Contemporary (2012) Helio S. Sader, MD, PhD JMI Laboratories Bacteria Collected from USA Patients with Acute Bacterial Skin and Skin Structure Infections (ABSSSIs) North Liberty, IA, USA ECCMID 2013 www.jmilabs.com HS SADER, RK FLAMM, RN JONES ph. 319.665.3370 P1620 fax 319.665.3371 JMI Laboratories, North Liberty, Iowa, USA [email protected] Table 2. Antimicrobial activities of ceftaroline-avibactam, ceftaroline and comparator agents when tested against gram-negative organisms from Abstract Introduction Results skin and skin structure infections (USA, 2012). Conclusions Objective: To evaluate the activity of ceftaroline Ceftaroline, the active metabolite of the prodrug ceftaroline • The most common organisms were S. aureus (3,481; Organism (no tested)/ MIC (mg/L) %S / %I / %R • Ceftaroline-avibactam was highly active antimicrobial agent 50% 90% Range CLSIa EUCASTa (CPT)-avibactam (AVI) tested against bacteria from fosamil, is a cephalosporin with notable in vitro bactericidal 50.5% MRSA), E. coli (444; 13.3% ESBL-phenotype), β- E. coli (444) against ESBL-phenotype and carbapenem- ABSSSI collected in USA hospitals in 2012. CPT activity against organisms commonly responsible for haemolytic streptococci (βHS; 389) and Klebsiella spp. Ceftaroline-avibactam 0.03 0.06 ≤0.015 – 0.5 - / - / - - / - / - non-susceptible Enterobacteriaceae Ceftaroline 0.12 32 ≤0.015 – >32 83.3 / 2.7 / 14.0 83.3 / 0.0 / 16.7 fosamil is a novel parenteral cephalosporin community-acquired