Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vaginal Breech Birth Mary Olusile Lecturer in Practice
1 Vaginal Breech birth Mary Olusile Lecturer in Practice Breech: is where the fetal buttocks is the presenting part. Occurs in 15% of pregnancies at 28wks reducing to 3-4% at term Usually associated with: Uterine & pelvic anomalies - bicornuate uterus, lax uterus, fibroids and cysts Fetal anomalies - anencephaly, hydrocephaly, multiple gestation, oligohydraminous and polyhydraminous Cornually placed placenta (probably the commonest cause). Diagnosis: by abdominal examination or vaginal examination and confirmed by ultrasound scan Vaginal Breech VS. Caesarean Section Trial by Hannah et al (2001) found CS to produce better outcomes than vaginal breech but does acknowledge that may be due to lost skills of operators Therefore recommended mode of delivery is CS Limitations of trial by Hannah et al have since been highlighted questioning results and conclusion (Kotaska 2004) Now some advocates for vaginal breech birth when selection is based on clear prelabour and intrapartum criteria (Alarab et al 2004) Breech birth is u sually not an option except at clients choice Important considerations are size of fetus, presentation, attitude, size of maternal pelvis and parity of the woman NICE recommendation: External cephalic version (ECV) to be considered and offered if appropriate Produced by CETL 2007 2 Vaginal Breech birth Anterior posterior diameter of the pelvic brim is 11 cm Oblique diameter of the pelvic brim is 12 cm Transverse diameter of the pelvic brim is 13 cm Anterior posterior diameter of the outlet is 13 cm Produced by CETL 2007 3 -

Maternal Movement and Position Changes to Facilitate Labor Progress Have Been Discussed in the Literature for Decades
ELAINE ZWELLING, PHD, RN, LCCE, FACCE Abstract The benefi ts of maternal movement and position changes to facilitate labor progress have been discussed in the literature for decades. Recent routine interventions such as amniotomy, induction, fetal monitoring, and epidural anesthesia, as well as an increase in maternal obesity, have made position changes during labor challenging. The lack of maternal changes in position throughout labor can contribute to dystocia and increase the risk of cesarean births for failure to progress or descend. This article provides a historical review of the research fi ndings related to the effects of maternal positioning on the labor process and uses six physiological principles as a framework to offer sug- gestions for maternal positioning both before and after epidural anesthesia. Key Words Birth; Childbirth; Labor, fi rst stage; Labor, second stage; Maternity nursing; Obstetrical nursing; Maternal postures; Maternal positioning. Overcoming the Challenges: Maternal Movement 72 volume 35 | number 2 March/April 2010 or centuries laboring women chose to remain dural anesthesia, found that women who were able to mobile and upright, using positions such as change positions regularly or maintain upright positions standing, sitting, kneeling, hands and knees, or during labor were more comfortable and required less Fsquatting (Gupta & Nikodem, 2000; Johnson, pain medication (Atwood, 1976; de Jong et al., 1997; En- Johnson, & Gupta, 1991). Today immobility throughout gelmann, 1977; Johnson et al., 1991). For instance, Ada- the labor process has become a common occurrence for chi, Shimada, and Usul (2003) found in their study of 58 many childbearing women. Increased medical manage- laboring women that a sitting position decreased labor ment, obesity, lack of patient understanding about the pain in contrast with supine positioning. -

Variation in Fetal Presentations and Positions Among Women in Warri, Delta State, Nigeria
World Research Journal of Obstetrics and Gynecology ISSN: 2277-6001, Volume 2, Issue 1, 2013, pp.-10-12. Available online at http://www.bioinfopublication.org/jouarchive.php?opt=&jouid=BPJ0000126 VARIATION IN FETAL PRESENTATIONS AND POSITIONS AMONG WOMEN IN WARRI, DELTA STATE, NIGERIA OLANIYAN O.T.1*, MERAIYEBU A.B.1, ALELE J.Y.1, DARE J.B.2, ATSUKWEI D.1 AND ADELAIYE A.B.1 1Department of Physiology, Bingham University, Karu, Nasarawa, Nigeria. 2Department of Anatomy, Bingham University, Karu, Nasarawa, Nigeria. *Corresponding Author: Email- [email protected] Received: November 21, 2013; Accepted: December 23, 2013 Abstract- This study investigates the various fetal presentations among women in Warri and the various predisposing factors which may have possibly brought about these variations; the major positions considered were cephalic, breech and transverse, with the considered influencing factors being gestational age of the fetus, maternal age, amniotic fluid volume, parity, and method of previous deliveries. A total of 105 ultra- sound fetal biometries with a total of 108 fetuses, between 15-40 weeks of gestational age, and maternal age between 19 and 40 were used for this study. Fetal ultrasound biometry was used to find out information about the fetus including gestational age, amniotic fluid volume, presentation of the fetus and a questionnaire was used to take information about the mother including maternal age, parity, and method of previous delivery (ies). The result showed that a total of 82 fetuses (75.9%) were Cephalic babies, 19 (17.6%) were Breech and 7 (6.5%) are transverse. Out of the 105 women, there were 102 (77.1% cephalic, 18.3% breech, 4.8% transverse) women with adequate amniotic fluid volume and 1 woman (with a cephalic fetus) with average amniotic fluid volume and 2 women (with transverse foetuses) with low amniotic fluid volume. -

OB/GYN – Childbirth/Labor/Delivery Protocol 6 - 2
Section SECTION: Obstetrical and Gynecological Emergencies REVISED: 06/2015 6 1. Physiologic Changes with Pregnancy Protocol 6 - 1 2. OB/GYN – Childbirth/Labor/Delivery Protocol 6 - 2 3. Medical – Newborn/Neonatal Protocol 6 - 3 OB / GYN Resuscitation 4. OB/GYN – Pregnancy Related Protocol 6 - 4 Emergencies (Delivery – Shoulder Dystocia) 5. OB/GYN – Pregnancy Related Protocol 6 - 5 Emergencies (Delivery – Breech Presentation) 6. OB/GYN – Pregnancy Related Protocol 6 - 6 Emergencies (Ectopic Pregnancy/Rupture) 7. OB/GYN – Pregnancy Related Protocol 6 - 7 EMERGENCIES Emergencies (Abruptio Placenta) 8. OB/GYN – Pregnancy Related Protocol 6 - 8 Emergencies (Placenta Previa) 9. OB/GYN – Pregnancy Related Protocol 6 - 9 Emergencies (Umbilical Cord Prolapse) 10. OB/GYN - Eclampsia Protocol 6 - 10 (Hypertension/Eclampsia/HELLPS) 11. OB/GYN – Pregnancy Related Protocol 6 - 11 Emergencies (Premature Rupture of Membranes (PROM)) 12. OB/GYN - Pre-term Labor Protocol 6 - 12 (Pre-term Labor) 13. OB/GYN – Post-partum Hemorrhage Protocol 6 - 13 Created, Developed, and Produced by the Old Dominion EMS Alliance Section 6 Continued This page intentionally left blank. OB / GYN EMERGENCIES Created, Developed, and Produced by the Old Dominion EMS Alliance Protocol SECTION: Obstetrical/Gynecological Emergencies PROTOCOL TITLE: Physiologic Changes with Pregnancy 6-1 REVISED: 06/2017 OVERVIEW: Many changes occur in the pregnant woman’s body, starting from the time of conception and throughout the pregnancy. The most obvious body system to undergo change is the reproductive system, but all of the others will change as well. Brief summaries of the physiologic changes that occur during pregnancy have been listed by system. Most of these physiologic changes will resolve during the postpartum period. -

Psycho-Socio-Cultural Risk Factors for Breech Presentation Caroline Peterson University of South Florida
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School 7-2-2008 Psycho-Socio-Cultural Risk Factors for Breech Presentation Caroline Peterson University of South Florida Follow this and additional works at: https://scholarcommons.usf.edu/etd Part of the American Studies Commons Scholar Commons Citation Peterson, Caroline, "Psycho-Socio-Cultural Risk Factors for Breech Presentation" (2008). Graduate Theses and Dissertations. https://scholarcommons.usf.edu/etd/451 This Dissertation is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. Psycho-Socio-Cultural Risk Factors for Breech Presentation by Caroline Peterson A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Department of Anthropology College of Arts and Science University of South Florida Major Professor: Lorena Madrigal, Ph.D. Wendy Nembhard, Ph.D. Nancy Romero-Daza, Ph.D. David Himmelgreen, Ph.D. Getchew Dagne, Ph.D. Date of Approval: July 2, 2008 Keywords: Maternal Fetal Attachment, Evolution, Developmental Plasticity, Logistic Regression, Personality © Copyright 2008, Caroline Peterson Dedication This dissertation is dedicated to all the moms who long for answers about their babys‟ presentation and to the babies who do their best to get here. Acknowledgments A big thank you to the following folks who made this dissertation possible: Jeffrey Roth who convinced ACHA to let me use their Medicaid data then linked it with the birth registry data. David Darr who persuaded the Florida DOH to let me use the birth registry data for free. -

• Chapter 8 • Nursing Care of Women with Complications During Labor and Birth • Obstetric Procedures • Amnioinfusion –
• Chapter 8 • Nursing Care of Women with Complications During Labor and Birth • Obstetric Procedures • Amnioinfusion – Oligohydramnios – Umbilical cord compression – Reduction of recurrent variable decelerations – Dilution of meconium-stained amniotic fluid – Replaces the “cushion ” for the umbilical cord and relieves the variable decelerations • Obstetric Procedures (cont.) • Amniotomy – The artificial rupture of membranes – Done to stimulate or enhance contractions – Commits the woman to delivery – Stimulates prostaglandin secretion – Complications • Prolapse of the umbilical cord • Infection • Abruptio placentae • Obstetric Procedures (cont.) • Observe for complications post-amniotomy – Fetal heart rate outside normal range (110-160 beats/min) suggests umbilical cord prolapse – Observe color, odor, amount, and character of amniotic fluid – Woman ’s temperature 38 ° C (100.4 ° F) or higher is suggestive of infection – Green fluid may indicate that the fetus has passed a meconium stool • Nursing Tip • Observe for wet underpads and linens after the membranes rupture. Change them as often as needed to keep the woman relatively dry and to reduce the risk for infection or skin breakdown. • Induction or Augmentation of Labor • Induction is the initiation of labor before it begins naturally • Augmentation is the stimulation of contractions after they have begun naturally • Indications for Labor Induction • Gestational hypertension • Ruptured membranes without spontaneous onset of labor • Infection within the uterus • Medical problems in the -

Module Presentation
Module Presentation How to best use the Modules To make the best use of this training we encourage you to complete each Module in order following the format below: 1. Read Module Presentation. Added explanations can be found in the HELPER Guidelines and in the extra information section if there is one. 2. Complete the Extraction/Scenario training exercises. The extraction exercises use de-identified and altered patient medical records. Enter the requested information into the provided section from the Birth Certificate Workbook. The Scenarios are situations you may encounter as you collect information from your patients’ medical records. 3. Check your responses using the answer sheets immediately following the segment completed 4. Complete the Module specific Evaluation, as before the answers are immediately following the Evaluation 5. If not already done, read extra training materials, if available. If you have questions about how to answer any of the requests for information in the NYS Certification of Live Birth Training Modules, please contact Rosemary Varga (585-275-8737). *”Coding” is a convenient although slightly misleading term for entering the needed information in the Statewide Perinatal Data system. True “coding” is the entry of predetermined numbers into a system that can then rate the material. We do not use numbers rather we enter the requested information. Module Three Labor & Delivery Part I Labor & Delivery Fields •Labor & Delivery information is found in the mother’s chart with much of the information on the L & D flowsheet/summary. A copy of this information may also be found in the infant’s chart. 2 Mother Transferred in Antepartum •Only complete these fields if the mother was transferred for medical reasons NYS GUIDELINES 3 Mother’s Weight at Delivery •Mother’s weight at delivery will often be found on the L&D flowsheet If you can’t find mother’s weight at delivery in the L&D information you can use the mother’s weight at her last prenatal visit if the visit was within 2 weeks of delivery. -

Metaphysical Anatomy Table of Contents
EVETTE ROSE TABLE OF CONTENTS Table of Contents .......................................................................................................................... iv Introduction..................................................................................................................................... 3 Healing, Reference Point Therapy and Religion........................................................................ 5 Understanding and “completing” trauma................................................................................... 6 The difference between completing trauma and surviving trauma.................................... 7 Disassociating from trauma...................................................................................................... 8 Secondary Trauma...................................................................................................................... 9 Emotions and Ancestral Trauma ................................................................................................. 9 Why do I have such emotional conflict? .............................................................................. 10 Can my ancestors’ abuse manifest in my life? .......................................................................... 10 Key Emotions during a session.................................................................................................. 11 Working with Injuries.................................................................................................................. -

Reducing Alcohol Use During Pregnancy Saves Lives
WICWORKS REDUCING ALCOHOL USE DURING PREGNANCY SAVES LIVES women drink no alcohol at all if pregnant or planning to become pregnant.7 Low-income women, whose children are most at risk for negative health outcomes, are less likely to receive appropriate counseling regarding alcohol use in pregnancy.8.9 The Supplemental Nutrition Program for Women, Infants and Children (WIC) serves more than 9 million low-income participants each month, including more than half of all infants born in the United States.10 Given its reach into a high- risk population during this critical period of the life nfants exposed to alcohol before birth can cycle, WIC can play a major role in reducing alcohol have serious life-long problems. WIC is in consumption during pregnancy. Along with food and Ian excellent position to screen pregnant nutrition education, WIC agencies are mandated by women for alcohol use during pregnancy and federal law to provide individual screening for drug and help women change their drinking behaviors. alcohol use and to make referrals to substance abuse In collaboration with UCLA, the largest local treatment programs when needed.11 The challenge with agency WIC program in the country designed such screening and referral is that only heavy users of and conducted a randomized study of a brief alcohol qualify for substance abuse treatment programs, intervention program to reduce prenatal yet lower levels of alcohol use can also be harmful to the alcohol use among WIC participants. Results developing fetus. Until now, WIC screening has often documented that brief intervention conducted led to recognition of prenatal alcohol use—with no in the WIC setting led to significant reductions accompanying intervention tools available. -
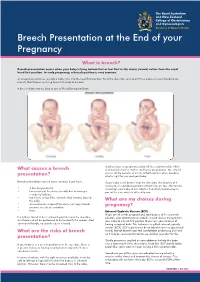
Breech Presentation at the End of Your Pregnancy
Breech Presentation at the End of your Pregnancy What is breech? Breech presentation occurs when your baby is lying bottom first or feet first in the uterus (womb) rather than the usual head first position. In early pregnancy, a breech position is very common. As pregnancy continues, usually a baby turns into the head first position. Near the due date, only about three babies in every hundred are breech. Most babies are lying head first ready to be born. A breech baby may be lying in one of the following positions: In other cases a caesarean section will be recommended, which What causes a breech also has risks for the mother and future pregnancies. You should discuss all the benefits and risks of both options when deciding presentation? what is right for you and your baby. Breech presentation may be more common if you have: If your baby is still breech near the due date, the chances of it turning to a head down position without help are low. Attempts to • a low-lying placenta encourage your baby to turn into the head first position may be • lax muscles of the uterus (usually due to having a part of the care which is offered to you. number of babies) • too much, or too little, amniotic fluid (waters) around the baby What are my choices during • an uncommon shape of the uterus, or large fibroids pregnancy? • previous breech presentation • twins External Cephalic Version (ECV) If you are 36 weeks pregnant and your baby is still in a breech If a baby is found to be in a breech position near the due date, position, your obstetrician or midwife should discuss trying to turn an ultrasound will be performed to try to identify the reason. -

Contribution of Changing Risk Factors to the Trend in Breech Presentation
1 The final version of this paper was published in Australian New Zealand Journal of Obstetrics and Gynaecology 2016 56(6): 564-570 MANUSCRIPT TITLE: Contribution of Changing Risk Factors to the Trend in Breech Presentation at Term SHORT TITLE: Trend in Term Breech Presentation WORD COUNTS Abstract= 247/250 Main text= 2262/2500 References=30/30 Tables=2/4 Figures=2 KEYWORDS (MESH TERMS) (1) breech presentation, (2) trends, (3) risk factors, (4) external cephalic version 2 ABSTRACT Background: Recent population-wide changes in perinatal risk factors may affect rates of breech presentation at birth, and have implications for the provision of breech services and clinical training in breech management. Aims: To determine the trend in breech presentation at term and investigate whether changes in maternal and pregnancy characteristics explain the observed trend. Materials and Methods: All singleton term (≥37 week) births in New South Wales during 2002 – 2012 were identified through birth and associated hospital records. Annual rates of breech presentation were determined. Logistic regression modelling was used to predict expected rates of breech presentation over time and these were compared with observed rates. A priori predictors included maternal age, country of birth, parity, smoking during pregnancy, diabetes, pregnancy hypertension, placenta praevia, previous singleton term breech, previous caesarean section, infant sex, gestational age, birthweight, and congenital anomalies. Hospital and Medicare data were used to assess trends in external cephalic version. Results: Among 914,147 singleton term births, 3.1% were breech at delivery. Rates declined from 3.6% in 2002 to 2.7% in 2012 (test for trend p<0.001). -

Management of Breech Presentation
Management of Breech Presentation Green-top Guideline No. 20b March 2017 Please cite this paper as: Impey LWM, Murphy DJ, Griffiths M, Penna LK on behalf of the Royal College of Obstetricians and Gynaecologists. Management of Breech Presentation. BJOG 2017; DOI: 10.1111/1471-0528.14465. DOI: 10.1111/1471-0528.14465 Management of Breech Presentation This is the fourth edition of this guideline originally published in 1999 and revised in 2001 and 2006 under the same title. Executive summary of recommendations What information should be given to women with breech presentation at term? Women with a breech presentation at term should be offered external cephalic version (ECV) A unless there is an absolute contraindication. They should be advised on the risks and benefits of ECV and the implications for mode of delivery. [New 2017] Women who have a breech presentation at term following an unsuccessful or declined offer of ECV should be counselled on the risks and benefits of planned vaginal breech delivery versus planned caesarean section. What information about the baby should be given to women with breech presentation at term regarding mode of delivery? Women should be informed that planned caesarean section leads to a small reduction in A perinatal mortality compared with planned vaginal breech delivery. Any decision to perform a caesarean section needs to be balanced against the potential adverse consequences that may result from this. Women should be informed that the reduced risk is due to three factors: the avoidance of B stillbirth after 39 weeks of gestation, the avoidance of intrapartum risks and the risks of vaginal breech birth, and that only the last is unique to a breech baby.