Day 4 Digestive System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Jemds.Com Case Report
Jemds.com Case Report RIGHT SIDED SIGMOID COLON AND REDUNDANT DESCENDING COLON ON CONVENTIONAL AND CT IMAGING Mandeep Singh1, Madhan Kumar2, Daisy Gupta3 1Junior Resident, Department of Radiodiagnosis, Government Medical College, Amritsar, Punjab, India. 2Junior Resident, Department of Radiodiagnosis, Government Medical College, Amritsar, Punjab, India. 3Assistant Professor, Department of Radiodiagnosis, Government Medical College, Amritsar, Punjab, India. HOW TO CITE THIS ARTICLE: Singh M, Kumar M, Gupta D. Right sided sigmoid colon and redundant descending colon on conventional and CT imaging. J. Evolution Med. Dent. Sci. 2018;7(44):5617-5620, DOI: 10.14260/jemds/2018/1073 CASE PRESENTATION Investigations A 62-year-old male presented with history of severe On Plain X-Ray Abdomen constipation, abdominal distension, haemorrhoids and blood No abnormal air-fluid levels were seen. There were no in stool in surgical OPD of Guru Nanak Dev Hospital, abnormal radio-opaque shadows seen. Bilateral psoas Amritsar. The patient was referred for barium studies of shadows and soft tissue shadows were identified as normal. colon, which showed a loop of colon in pelvic region (at normal location of ileal loops) and redundant and long On Barium Enema descending colon extending across midline to reach hepatic After filling the rectum, the contrast was identified as filling flexure on right and continuing as sigmoid colon on right side. the sigmoid colon, which was present anomalously towards Transverse colon and ascending colon were normal in length the right side. Filling of barium outlined the extension of and position. On CECT abdomen of the patient, a long colon from sigmoid on right side with coiling in right iliac segment of descending colon was identified. -

The Herbivore Digestive System Buffalo Zebra
The Herbivore Digestive System Name__________________________ Buffalo Ruminant: The purpose of the digestion system is to ______________________________ _____________________________. Bacteria help because they can digest __________________, a sugar found in the cell walls of________________. Zebra Non- Ruminant: What is the name for the largest section of Organ Color Key a ruminant’s Mouth stomach? Esophagus __________ Stomach Small Intestine Cecum Large Intestine Background Information for the Teacher Two Strategies of Digestion in Hoofed Mammals Ruminant Non‐ruminant Representative species Buffalo, cows, sheep, goats, antelope, camels, Zebra, pigs, horses, asses, hippopotamus, rhinoceros giraffes, deer Does the animal Yes, regurgitation No regurgitation regurgitate its cud to Grass is better prepared for digestion, as grinding Bacteria can not completely digest cell walls as chew material again? motion forms small particles fit for bacteria. material passes quickly through, so stool is fibrous. Where in the system do At the beginning, in the rumen Near the end, in the cecum you find the bacteria This first chamber of its four‐part stomach is In this sac between the two intestines, bacteria digest that digest cellulose? large, and serves to store food between plant material, the products of which pass to the rumination and as site of digestion by bacteria. bloodstream. How would you Higher Nutrition Lower Nutrition compare the nutrition Reaps benefits of immediately absorbing the The digestive products made by the bacteria are obtained via digestion? products of bacterial digestion, such as sugars produced nearer the end of the line, after the small and vitamins, via the small intestine. intestine, the classic organ of nutrient absorption. -
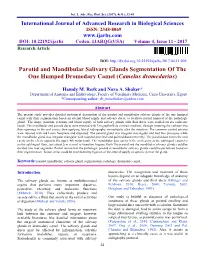
Parotid and Mandibular Salivary Glands Segmentation of the One Humped Dromedary Camel (Camelus Dromedarius)
Int. J. Adv. Res. Biol. Sci. (2017). 4(11): 32-41 International Journal of Advanced Research in Biological Sciences ISSN: 2348-8069 www.ijarbs.com DOI: 10.22192/ijarbs Coden: IJARQG(USA) Volume 4, Issue 11 - 2017 Research Article DOI: http://dx.doi.org/10.22192/ijarbs.2017.04.11.005 Parotid and Mandibular Salivary Glands Segmentation Of The One Humped Dromedary Camel (Camelus dromedarius) Hamdy M. Rezk and Nora A. Shaker* Department of Anatomy and Embryology, Faculty of Veterinary Medicine, Cairo University, Egypt *Corresponding author: [email protected] Abstract The present study provides detailed anatomical description of the parotid and mandibular salivary glands of the one humped camel with their segmentation based on arterial blood supply and salivary ducts; to facilitate partial removal of the pathologic gland. The shape, position, relations and blood supply of both salivary glands with their ducts were studied on six cadaveric heads. The mandibular and parotid ducts were injected with Urographin® as contrast medium; through inserting the catheter into their openings in the oral cavity; then applying lateral radiography immediately after the injection. The common carotid arteries were injected with red Latex Neoprene and dissected. The parotid gland was irregular rectangular and had five processes while the mandibular gland was irregular triangular with rounded proximal and pointed distal extremity. The parotid duct enters the oral cavity on the cheek opposite the upper 4th molar tooth. The mandibular duct opens in the oral cavity at the sublingual caruncles on the sublingual floor, just about 2cm cranial to frenulum linguae. Both The parotid and the mandibular salivary glands could be divided into four segments. -

Mouth Esophagus Stomach Rectum and Anus Large Intestine Small
1 Liver The liver produces bile, which aids in digestion of fats through a dissolving process known as emulsification. In this process, bile secreted into the small intestine 4 combines with large drops of liquid fat to form Healthy tiny molecular-sized spheres. Within these spheres (micelles), pancreatic enzymes can break down fat (triglycerides) into free fatty acids. Pancreas Digestion The pancreas not only regulates blood glucose 2 levels through production of insulin, but it also manufactures enzymes necessary to break complex The digestive system consists of a long tube (alimen- 5 carbohydrates down into simple sugars (sucrases), tary canal) that varies in shape and purpose as it winds proteins into individual amino acids (proteases), and its way through the body from the mouth to the anus fats into free fatty acids (lipase). These enzymes are (see diagram). The size and shape of the digestive tract secreted into the small intestine. varies in each individual (e.g., age, size, gender, and disease state). The upper part of the GI tract includes the mouth, throat (pharynx), esophagus, and stomach. The lower Gallbladder part includes the small intestine, large intestine, The gallbladder stores bile produced in the liver appendix, and rectum. While not part of the alimentary 6 and releases it into the duodenum in varying canal, the liver, pancreas, and gallbladder are all organs concentrations. that are vital to healthy digestion. 3 Small Intestine Mouth Within the small intestine, millions of tiny finger-like When food enters the mouth, chewing breaks it 4 protrusions called villi, which are covered in hair-like down and mixes it with saliva, thus beginning the first 5 protrusions called microvilli, aid in absorption of of many steps in the digestive process. -

Crohn's Disease of the Colon
Gut, 1968, 9, 164-176 Gut: first published as 10.1136/gut.9.2.164 on 1 April 1968. Downloaded from Crohn's disease of the colon V. J. McGOVERN AND S. J. M. GOULSTON From the Royal Prince Alfred Hospital, Sydney, Australia The fact that Crohn's disease may involve the colon never affected unless there had been surgical inter- either initially or in association with small bowel ference. There was no overt manifestation of mal- disease is now firmly established due largely to the absorption in any of these patients. evidence presented by Lockhart-Mummery and In 18 cases the colon alone was involved. Five had Morson (1960, 1964) and Marshak, Lindner, and universal involvement, five total involvement with Janowitz (1966). This entity is clearly distinct from sparing of the rectum, two involvement of the ulcerative colitis and other forms of colonic disease. descending colon only, two the transverse colon only, Our own experience with this disorder reveals many and in the other four there was variable involvement similarities with that published from the U.K. and of areas of large bowel (Fig. 2). the U.S.A. Thirty patients with Crohn's disease involving the large bowel were seen at the Royal CLINICAL FEATURES Prince Alfred Hospital during the last decade, the majority during the past five years. The criteria for The age incidence varied from 6 to 69 years when the inclusion were based on histological examination of patient was first seen, the majority being between the operative specimens in 28 and on clinical and radio- ages of 11 and 50. -

Acute Liver Failure J G O’Grady
148 Postgrad Med J: first published as 10.1136/pgmj.2004.026005 on 4 March 2005. Downloaded from REVIEW Acute liver failure J G O’Grady ............................................................................................................................... Postgrad Med J 2005;81:148–154. doi: 10.1136/pgmj.2004.026005 Acute liver failure is a complex multisystemic illness that account for most cases, but a significant number of patients have no definable cause and are evolves quickly after a catastrophic insult to the liver classified as seronegative or of being of indeter- leading to the development of encephalopathy. The minate aetiology. Paracetamol is the commonest underlying aetiology and the pace of progression strongly cause in the UK and USA.2 Idiosyncratic reac- tions comprise another important group. influence the clinical course. The commonest causes are paracetamol, idiosyncratic drug reactions, hepatitis B, and Viral seronegative hepatitis. The optimal care is multidisciplinary ALF is an uncommon complication of viral and up to half of the cases receive liver transplants, with hepatitis, occurring in 0.2%–4% of cases depend- ing on the underlying aetiology.3 The risk is survival rates around 75%–90%. Artificial liver support lowest with hepatitis A, but it increases with the devices remain unproven in efficacy in acute liver failure. age at time of exposure. Hepatitis B can be associated with ALF through a number of ........................................................................... scenarios (table 2). The commonest are de novo infection and spontaneous surges in viral repli- cation, while the incidence of the delta virus cute liver failure (ALF) is a complex infection seems to be decreasing rapidly. multisystemic illness that evolves after a Vaccination should reduce the incidence of Acatastrophic insult to the liver manifesting hepatitis A and B, while antiviral drugs should in the development of a coagulopathy and ameliorate replication of hepatitis B. -

Variation of Cystic Duct Insertion in Relation to the Extrahepatic Ducts
AbeshaAmbaye et al. / International Journal of Pharma Sciences and Research (IJPSR) Variation of Cystic Duct Insertion in Relation to the Extrahepatic Ducts and Observed Frequency of Double Lumen Apparent Common Bile Duct AbeshaAmbaye1, MueezAbraha2,Bernard A. Anderson2, Amanuel T. Tsegay1 Anatomy Course and Research Team, Institute of Biomedical Sciences, College of Health Sciences, Mekelle University Dep’t of Anatomy, College of Medicine and Health Sciences, University of Gondar, Ethiopia email [email protected] ABSTRACT Background: Variations in the pattern of the extra hepatic biliary tract are common and usually encountered during radiological investigations or during operations on the biliary tree. Having a good knowledge of the possible connections of the cystic duct with the common hepatic duct to form the common bile duct is very important; because variation in this area is common. Objectives: The main aim of this study is to evaluate the frequency of anatomic variations of the cystic duct insertion in relation to the extrahepatic ducts and Observed Frequency of Double Lumen Apparent Common Bile Duct Methods: Institutional based cross-sectional study design with observational data collection tool was conducted in 25 Ethiopian fixed cadavers and Forensic autopsy specimens obtained from Departments of Human Anatomy at University of Gondar, Mekelle and St. Paul Hospital Millennium Medical College Result: From the total 25 specimens dissected 9 (36%) had the ACBD and the 16 (64%) of them had CBD with one lumen. Conclusion: The billiary system formation is very variable, among the variants; the number of the supradoudenal insertion is greater than the infradoudenal insertion. ACBD is more frequent than expected which is 36% of the total data. -

Multiple Epithelia Are Required to Develop Teeth Deep Inside the Pharynx
Multiple epithelia are required to develop teeth deep inside the pharynx Veronika Oralováa,1, Joana Teixeira Rosaa,2, Daria Larionovaa, P. Eckhard Wittena, and Ann Huysseunea,3 aResearch Group Evolutionary Developmental Biology, Biology Department, Ghent University, B-9000 Ghent, Belgium Edited by Irma Thesleff, Institute of Biotechnology, University of Helsinki, Helsinki, Finland, and approved April 1, 2020 (received for review January 7, 2020) To explain the evolutionary origin of vertebrate teeth from closure of the gill slits (15). Consequently, previous studies have odontodes, it has been proposed that competent epithelium spread stressed the importance of gill slits for pharyngeal tooth formation into the oropharyngeal cavity via the mouth and other possible (12, 13). channels such as the gill slits [Huysseune et al., 2009, J. Anat. 214, Gill slits arise in areas where ectoderm meets endoderm. In 465–476]. Whether tooth formation deep inside the pharynx in ex- vertebrates, the endodermal epithelium of the developing pharynx tant vertebrates continues to require external epithelia has not produces a series of bilateral outpocketings, called pharyngeal been addressed so far. Using zebrafish we have previously demon- pouches, that eventually contact the skin ectoderm at corre- strated that cells derived from the periderm penetrate the oropha- sponding clefts (16). In primary aquatic osteichthyans, most ryngeal cavity via the mouth and via the endodermal pouches and pouch–cleft contacts eventually break through to create openings, connect to periderm-like cells that subsequently cover the entire or gill slits (17–19). In teleost fishes, such as the zebrafish, six endoderm-derived pharyngeal epithelium [Rosa et al., 2019, Sci. -

Overview of Gastrointestinal Function
Overview of Gastrointestinal Function George N. DeMartino, Ph.D. Department of Physiology University of Texas Southwestern Medical Center Dallas, TX 75390 The gastrointestinal system Functions of the gastrointestinal system • Digestion • Absorption • Secretion • Motility • Immune surveillance and tolerance GI-OP-13 Histology of the GI tract Blood or Lumenal Serosal Side or Mucosal Side Structure of a villus Villus Lamina propria Movement of substances across the epithelial layer Tight junctions X Lumen Blood Apical membrane Basolateral membrane X X transcellular X X paracellular GI-OP-19 Histology of the GI tract Blood or Lumenal Serosal Side or Mucosal Side Motility in the gastrointestinal system Propulsion net movement by peristalsis Mixing for digestion and absorption Separation sphincters Storage decreased pressure GI-OP-42 Intercellular signaling in the gastrointestinal system • Neural • Hormonal • Paracrine GI-OP-10 Neural control of the GI system • Extrinsic nervous system autonomic central nervous system • Intrinsic (enteric) nervous system entirely with the GI system GI-OP-14 The extrinsic nervous system The intrinsic nervous system forms complete functional circuits Sensory neurons Interneurons Motor neurons (excitatory and inhibitory) Parasympathetic nerves regulate functions of the intrinsic nervous system Y Reflex control of gastrointestinal functions Vago-vagal Afferent reflex Salivary Glands Composition of Saliva O Proteins α−amylase lactoferrin lipase RNase lysozyme et al mucus O Electrolyte solution water Na+ , K + - HCO3 -

Differential Metabolism of Alprazolam by Liver and Brain Cytochrome (P4503A) to Pharmacologically Active Metabolite
The Pharmacogenomics Journal (2002) 2, 243–258 2002 Nature Publishing Group All rights reserved 1470-269X/02 $25.00 www.nature.com/tpj ORIGINAL ARTICLE Differential metabolism of alprazolam by liver and brain cytochrome (P4503A) to pharmacologically active metabolite HV Pai1,2* ABSTRACT SC Upadhya1,2* Cytochrome P450 (P450) is a superfamily of enzymes which mediates metab- 1 olism of xenobiotics including drugs. Alprazolam, an anti-anxiety agent, is SJ Chinta * metabolized in rat and human liver by P4503A1 and P4503A4 respectively, SN Hegde1 to 4-hydroxy alprazolam (4-OHALP, pharmacologically less active) and ␣- V Ravindranath1,2 hydroxy alprazolam (␣-OHALP, pharmacologically more active). We exam- ined P450 mediated metabolism of alprazolam by rat and human brain 1Department of Neurochemistry, National microsomes and observed that the relative amount of ␣-OHALP formed in Institute of Mental Health & Neurosciences, brain was higher than liver. This biotransformation was mediated by a P450 Bangalore, India; 2National Brain Research Centre, ICGEB Campus, Aruna Asaf Ali Marg, isoform belonging to P4503A subfamily, which is constitutively expressed in New Delhi , India neuronal cells in rat and human brain. The formation of larger amounts of ␣-OHALP in neurons points to local modulation of pharmacological activity Correspondence: in brain, at the site of action of the anti-anxiety drug. Since hydroxy metab- V Ravindranath, National Brain Research olites of alprazolam are hydrophilic and not easily cleared through blood- Centre, ICGEB Campus, Aruna Asaf Ali ␣ Marg, New Delhi - 110 067, India CSF barrier, -OHALP would potentially have a longer half-life in brain. Tel: +91 124 630 8317 The Pharmacogenomics Journal (2002) 2, 243–258. -

Sporadic (Nonhereditary) Colorectal Cancer: Introduction
Sporadic (Nonhereditary) Colorectal Cancer: Introduction Colorectal cancer affects about 5% of the population, with up to 150,000 new cases per year in the United States alone. Cancer of the large intestine accounts for 21% of all cancers in the US, ranking second only to lung cancer in mortality in both males and females. It is, however, one of the most potentially curable of gastrointestinal cancers. Colorectal cancer is detected through screening procedures or when the patient presents with symptoms. Screening is vital to prevention and should be a part of routine care for adults over the age of 50 who are at average risk. High-risk individuals (those with previous colon cancer , family history of colon cancer , inflammatory bowel disease, or history of colorectal polyps) require careful follow-up. There is great variability in the worldwide incidence and mortality rates. Industrialized nations appear to have the greatest risk while most developing nations have lower rates. Unfortunately, this incidence is on the increase. North America, Western Europe, Australia and New Zealand have high rates for colorectal neoplasms (Figure 2). Figure 1. Location of the colon in the body. Figure 2. Geographic distribution of sporadic colon cancer . Symptoms Colorectal cancer does not usually produce symptoms early in the disease process. Symptoms are dependent upon the site of the primary tumor. Cancers of the proximal colon tend to grow larger than those of the left colon and rectum before they produce symptoms. Abnormal vasculature and trauma from the fecal stream may result in bleeding as the tumor expands in the intestinal lumen. -

Fact Sheet - Symptoms of Pancreatic Cancer
Fact Sheet - Symptoms of Pancreatic Cancer Diagnosis Pancreatic cancer is often difficult to diagnose, because the pancreas lies deep in the abdomen, behind the stomach, so tumors are not felt during a physical exam. Pancreatic cancer is often called the “silent” cancer because the tumor can grow for many years before it causes pressure, pain, or other signs of illness. When symptoms do appear, they can vary depending on the size of the tumor and where it is located on the pancreas. For these reasons, the symptoms of pancreatic cancer are seldom recognized until the cancer has progressed to an advanced stage and often spread to other areas of the body. General Symptoms Pain The first symptom of pancreatic cancer is often pain, because the tumors invade nerve clusters. Pain can be felt in the stomach area and/or in the back. The pain is generally worse after eating and when lying down, and is sometimes relieved by bending forward. Pain is more common in cancers of the body and tail of the pancreas. The abdomen may also be generally tender or painful if the liver, pancreas or gall bladder are inflamed or enlarged. It is important to keep in mind that there are many other causes of abdominal and back pain! Jaundice More than half of pancreatic cancer sufferers have jaundice, a yellowing of the skin and whites of the eyes. Jaundice is caused by a build-up bilirubin, a substance which is made in the liver and a component of bile. Bilirubin contains a lot of yellow pigment, and gives bile it’s color.